
Recommended
More Related Content
Similar to 17971_27.2_Aneurysm.ppt
Similar to 17971_27.2_Aneurysm.ppt (20)
Recently uploaded
Recently uploaded (20)
17971_27.2_Aneurysm.ppt
- 2. • PA 27.2: Describe the etiology, dynamics, pathology types and complications of aneurysms including aortic aneurysms • SPECIFIC LEARNING OBJECTIVES: • Define aneurysm, classify it based on anatomical and macroscopic features with help of an illustration • Discuss pathogenesis of aneurysms with special reference to Abdominal Aortic Aneursyms,its morphological variants and clinical complications • Explain the Aortic Dissections types and its outcome
- 3. Aneurysms are congenital or acquired dilations of blood vessels or the heart It can be • Congenital • acquired.
- 4. pseudo-aneurysm A false aneurysm results when a wall defect leads to the formation of an extravascular hematoma that communicates with the intravascular space (“pulsating hematoma”) a leak at the suture site of a vascular graft with a natural artery may also be a cause
- 5. True Aneurysm True aneurysm involves an intact attenuated arterial wall or thinned ventricular wall of the heart Predisposing Factors Aortic Aneurysms: Atherosclerosis (AS)(abdominal) Hypertension (HT) (ascending aorta) Tertiary syphilis (now rare) (ascending aorta) Ventricular – Post Transmural MI Other conditions include trauma, vasculitis, congenital defects (Berry) infections (mycotic)
- 6. Types of Aneurysms Saccular aneurysms: Eccentric spherical outpouchings; 5 to 20 cm in diameter & often contain thrombus. Fusiform aneurysms: diffuse, circumferential dilation of a long segment; vary in diameter (up to 20 cm) & length, involve the aortic arch, abdominal aorta, or the iliac arteries.
- 7. Pathogenesis Inadequate or abnormal connective tissue synthesis. Excessive connective tissue degradation. loss of smooth muscle/inappropriate synthesis of ECM.
- 8. Inadequate or abnormal connective tissue synthesis. • Marfan syndrome: defective fibrillin synthesis leads to elastic tissue weakening • Loeys-Dietz syndrome: mutations in TGF-β receptors in fibroblasts lead to abnormalities in elastin & collagen I/III formation. • Ehlers- Danlos syndrome: Weak vessel walls due to defective type III collagen synthesis • vitamin C deficiency altered collagen cross-linking PATHOGENESIS
- 9. Excessive connective tissue degradation. • By inflammatory infiltrates & increased ^ MMP production, by macrophages in atherosclerotic plaque or in vasculitis. • Decreased tissue inhibitor of metalloproteinase (TIMP) expression can contribute to the ECM degradation. • Genetic predisposition to aneurysm formation - polymorphisms of MMP &/or TIMP genes are noted. Adventitial inflammatory infiltrate and thickening of the vasa-vasorum (HE staining)
- 10. Weakened vascular wall due to loss of smooth muscle/inappropriate synthesis of ECM. Ischemia due to atherosclerosis (the inner media blood supply is compromised) or hypertension (outermedia vaso- vasorum) leads to smooth muscle cell loss (ischemia) & “degenerative changes,” (fibrosis, loss of elastic fibres, inadequate ECM synthesis, and production of excessive amorphous ground substance - glycosaminoglycan) • Histologically these nonspecific changes are collectively called cystic medial degeneration (also seen in Marfan disease and scurvy)
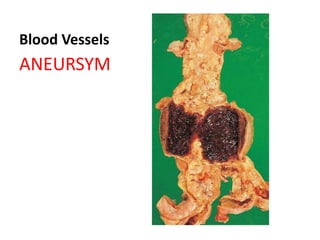
- 11. ABDOMINAL AORTIC ANEURYSM • Atherosclerosis (1st) is a major cause. • More frequently in men and smokers, and rare before 50 years of age • Usually positioned below the renal arteries and above the bifurcation of the aorta, can be saccular or fusiform, – Inflammatory (2) AAAs • Mycotic AAAs (3) occur when circulating microorganisms (as in bacteremia from a Salmonella gastroenteritis) seed the aneurysm wall or the associated thrombus; up to 15 cm in diameter, and up to 25 cm in length frequently contains a bland, laminated, mural thrombus
- 12. The Clinical Consequences Of AAA • Rupture into the peritoneal cavity or retroperitoneal tissues with massive, potentially fatal haemorrhage • Obstruction of a branch vessel resulting in ischemic injury of downstream tissues: iliac (leg), renal, mesenteric (GIT) or vertebral arteries • Embolism from atheroma or mural thrombus • Compression of an adjacent structure, e.g., of a ureter or erosion of vertebrae • Simulates an abdominal tumor (often pulsating)
- 13. Thoracic Aortic Aneurysms • Most commonly with hypertension, Marfan, Loeys -Dietz syndromes • Signs & symptoms referable to encroachment – on mediastinal structures, – On lungs & airways with respiratory difficulties – On oesophagus with difficulty in swallowing – On recurrent laryngeal nerve with persistent cough – On ribs and vertebrae with erosion & bone pain • Aortic valve dilation (syphilitic) with valvular insufficiency or narrowing of the coronary ostia leads to MI
- 14. Arterial dissection • Occurs when blood enters the arterial wall itself, as a hematoma dissecting between its layers. Dissections are often but not always aneurysmal. • Dissections can rupture, often with catastrophic consequences.
- 15. Aortic Dissection Occurs principally in two groups: • men aged 40 to 60, with antecedent hypertension (more than 90% of cases of dissection); • younger patients with connective tissue abnormalities of affecting the aorta (Marfan’s) Iatrogenic: complicating arterial cannulations during catheterization or cardiopulmonary bypass Rarely, for unknown reasons, during or after pregnancy.
- 16. Aortic Dissection • starts with an intimal tear. • In majority of cases the tear is in the ascending aorta, usually within 10 cm of the aortic valve, transverse or oblique, 1 to 5 cm in length. • The dissecting hematoma spreads usually between the middle & outer thirds of laminar planes
- 17. Aortic Dissection Proximal lesions (type A dissections) (More common and dangerous), involving the ascending aorta with or without descending aorta (types I and II of the DeBakey) Distal lesions beginning distal to the subclavian artery (type B dissections or DeBakey type III)
- 18. Symptoms & Outcome of Aortic Dissection • Sudden onset of excruciating pain, mimicking MI • The most common cause of death is rupture of the dissection outward into the pericardial (cardiac tamponade), pleural, or peritoneal cavities. • Rapid diagnosis and institution of intensive antihypertensive therapy, coupled with surgical procedures involving plication of the aortic wall, permit 65% to 75% survival