Blood transfusion checklist sania
•Download as DOCX, PDF•
1 like•5,448 views

To safeguard the health of patients with thalassaemia, blood should be obtained from carefully selected regular voluntary, non-remunerated donors and should be collected, processed, stored and distributed, by dedicated, quality assured blood transfusion centres.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Blood transfusion checklist sania
Similar to Blood transfusion checklist sania (20)
More from anjalatchi
More from anjalatchi (20)
Recently uploaded
Recently uploaded (20)
Blood transfusion checklist sania
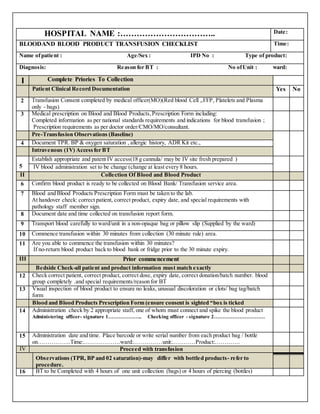
- 1. HOSPITAL NAME :…………………………….. Date: BLOODAND BLOOD PRODUCT TRANSFUSION CHECKLIST Time: Name ofpatient : Age/Sex : IPD No : Type of product: Diagnosis: Reason for BT : No ofUnit : ward: I Complete Priories To Collection Patient Clinical Record Documentation Yes No 2 Transfusion Consent completed by medical officer(MO)(Red blood Cell ,.FFP, Platelets and Plasma only - bags) 3 Medical prescription on Blood and Blood Products,Prescription Form including: Completed information as per national standards requirements and indications for blood transfusion ; Prescription requirements as per doctor order/CMO/MO/consultant. Pre-Transfusion Observations (Baseline) 4 Document TPR. BP & oxygen saturation , allergic history, ADR Kit etc., Intravenous (1V) Access for BT 5 Establish appropriate and patent IV access(18 g cannula/ may be IV site fresh prepared ) IV blood administration set to be change (change at least every 8 hours. II Collection Of Blood and Blood Product 6 Confirm blood product is ready to be collected on Blood Bank/ Transfusion service area. 7 Blood and Blood Products Prescription Form must be taken to the lab. At handover check: correct patient, correct product, expiry date, and special requirements with pathology staff member sign. 8 Document date and time collected on transfusion report form. 9 Transport blood carefully to ward/unit in a non-opaque bag or pillow slip (Supplied by the ward) 10 Commence transfusion within 30 minutes from collection (30 minute rule) area. 11 Are you able to commence the transfusion within 30 minutes? If no-return blood product back to blood bank or fridge prior to the 30 minute expiry. III Prior commencement Bedside Check-all patient and product information must match exactly 12 Check correct patient, correct product, correct dose, expiry date, correct donation/batch number. blood group completely .and special requirements/reason for BT 13 Visual inspection of blood product to ensure no leaks, unusual discoloration or clots/ bag tag/batch form Blood and Blood Products Prescription Form (ensure consent is sighted “box is ticked 14 Administration check by 2 appropriate staff, one of whom must connect and spike the blood product Administering officer- signature 1……………….. Checking officer - signature 2………………………… 15 Administration date and time. Place barcode or write serial number from each product bag / bottle on……………..Time:……………….ward:……………unit:…………Product:…………. IV Proceed with transfusion Observations (TPR, BP and 02 saturation)-may differ with bottled products- refer to procedure. 16 BT to be Completed with 4 hours of one unit collection (bags) or 4 hours of piercing (bottles)
- 2. Visual observation for the first 15 minutes. Document observations at every 15-30 minutes. 17 Hourly observations TPR/BP/Spo2 chart to be completion 18 Post transfusion observations report V. Post Transfusion 19 Document the completion time and volume infused. 20 Document procedure in the patient health record including outcome and any adverse event VI Suspected Transfusion Reactions (If ADR occurs) Transfusion reactions or Suspected Reactions 21 Refer to Transfusion Reaction Chart and Blood Product Administration Procedure. 22 Stop transfusion immediately leave giving set attached and keep cannula in-situ and patent. 23 Monitor and document vital signs 15 minutely or as often as required. 24 Re-check identification of the patient blood product and compatibility Notify medical officer. 25 Notify Blood Bank Transfusion services (fractionated product suppliers and private blood suppliers must be notified of suspected reactions) Obtain and complete reaction forms as required: 1. Pathology ADR Transfusion Reaction Form 2.(Indian Red Cross Blood Service) Transfusion Reacting form. 26. Mild reactions:(temperature rise of38"C to< 39"C with no other symptoms;or localized rash over <2/3 body). May be recommenced post medical officer review and once patient symptoms subside. Monitor closely for the initial 15 minutes .If reaction recommences cease transfusion and treat as a major reaction 27. Major Reactions: (temperature rise >38"C and other symptoms or >39C with/without other symptoms; or rash over >2/3 body; or more than 1single symptom) Collect all appropriate samples for investigation, ie. blood samples, cultures, MSU and chest x-ray Return remaining blood product /bag/ bottle and administration set to Blood Bank/Transfusion reporting centre. Report all suspected transfusion reactions into ADR report form database 28. Document patient reaction including symptoms, investigations, interventions, and outcomes Etc REMARKS: 1. ………………………………………………………………………………………………………… 2. ………………………………………………………………………………………………………… 3. ………………………………………………………………………………………………………… 4. ………………………………………………………………………………………………………. SIGN OF PERFORMER : SIGN OF SUPERVISOR: DATE : DATE:
- 3. SYMBOL NAME OF THE HOSPITAL:………………. ADDRESS:…………………………………. ADR /VITAL SIGN MONITORING CHECKLIST Name of patient :- …………………………. IPD:-………………………… Age/Sex:- ………………… ………………. Diagnosis:-………………….. Ref . Dr…………........................................... Dept:………………………... S.no. Time Temp. PR RR B.P Drop set Remark Sign.
- 4. BLOOD TRANSFUSION VERIFICATION CHECKLIST Reasonfor B.T:- Type of Bloodproduct:- Date/Time :- No. of Unit:- Bag tag:- Sign of Nursing Officer Sign of Supervisor Date:- Date :- Starting time: RH Factor: Cross matching: Blood Group: End time