

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Gout
Similar to Gout (20)
More from Anant Layall
More from Anant Layall (13)
Recently uploaded
Recently uploaded (20)
Gout
- 1. GOUT
- 2. Gout is a heterogeneous group of conditions related to a genetic defect of purine metabolism resulting in hyperuricemia. Over secretion of uric acid or a renal defect resulting in decreased excretion of uric acid, or a combination of both, occurs.
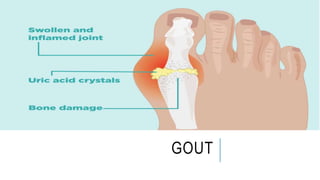
- 3. DEFINITION It is a form of arthritis characterized by severe pain, redness and tenderness in joints. Pain and inflammation occur when too much uric acid crystallizes and deposits in the joints.
- 4. INCIDENCE The prevalence of gout is reported to be 1.6 to 13.6 per thousand. The incidence increases with age and body mass index. It occurs more commonly in males than females.
- 5. TYPES 1. Primary Hyperuricemia In primary hyperuricemia, elevated serum urate levels or manifestations of urate deposition appear to be consequences of faulty uric acid metabolism. Primary hyperuricemia may be due to severe dieting or starvation, excessive intake of foods that are high in purines (shellfish, organ meats), or heredity. 1. Secondary Hyperuricemia In secondary hyperuricemia, gout is a clinical feature secondary to any of a number of genetic or acquired processes, including conditions in which there is an increase in cell turnover.
- 6. ETIOLOGY It may be either the body produces too much uric acid or the kidneys excrete too little uric acid. •Diet. Eating a diet rich in meat and seafood and drinking beverages sweetened with fruit sugar (fructose) increase levels of uric acid •Alcohol consumption, especially of beer, also increases the risk of gout. •Obesity. In Obesity body produces more uric acid and the kidneys have a more difficult time eliminating uric acid. •Medical conditions. Untreated high blood pressure and chronic conditions such as diabetes, metabolic syndrome, and heart and kidney diseases. •Certain medications. The use of thiazide diuretics and low-dose aspirin also can increase uric acid levels.. •Family history of gout. Severe dieting Starvation
- 7. CLINICAL MANIFESTATIONS The signs and symptoms of gout almost always occur suddenly, and often at night. It includes: Intense joint pain. Usually in the big toe joint discomfort Inflammation and redness. The affected joint or joints become swollen, tender, warm and red. Limited range of motion
- 8. PATHOPHYSIOLOGY Due to etiological factors. Such as, starvation, genetic process etc. Uric acid levels rise, risk increases. Urate crystals precipitate within a joint. An inflammatory response occurs and an attack of gout begins. Repeated attacks, .
- 9. DIAGNOSTIC MEASURES •History and Physical Examination •Serum Uric Acid •A definitive diagnosis of gouty arthritis is established by polarized light microscopy of the synovial fluid of the involved joint. Uric acid crystals are seen within the polymorph nuclear leukocytes within the fluid.
- 10. MEDICAL MANAGEMENT Analgesics- an NSAID such as indomethacin is used to relieve an acute attack of gout. Colchicine (oral or parenteral) - Lowers the deposition of uric acid . Uricosuric agents, such as probenecid, correct hyperuricemia and dissolve deposited urate. Allopurinol- interrupts the breakdown of purines before uric acid is formed Corticosteroids may be used in resistant cases.
- 11. NURSING MANAGEMENT •Limit sweetened beverages, especially those sweetened with high-fructose corn syrup. •Limit or avoid alcohol. •Limit intake of meat, fish and poultry. •Maintain Ideal Body Weight •During the inter critical period, the patient feels well and may abandon preventive behaviors, which may result in an acute attack.