1. 1
CHAPTER ONE
INTRODUCTION
1.1 Background of study
Hensen disease also widely known as Leprosy is a chronic disease caused by the
bacteria mycobacterium lepromatus after physician Gerhard Armauer, leprosy is primarily
granulomatus disease of the peripheral nerves and mucosa of the upper respiratory tract,
causing permanent damage to the skin nerves, limbs and contrary to the folklore, leprosy does
not cause body parts to fall off although they can become numb or diseased as a result of
infection, this results in tissue loss, so fingers and toes become shortened and deformed as the
cartilage is absorbed into the body. Although the mode of transmission of Hensen's disease
remains uncertain, most investigators think that Mycobacterium leprea is usually spread from
person to person in respiratory droplets. Studies have shown that leprosy can be transmitted
to humans by ARMADILLOS and also known to be neither sexually transmitted nor highly
infectious after treatment.
Approximately 95% are naturally immune and suffers are no longer infectious as little as 2
weeks of treatment. The minimum incubation period reported is as short as a few weeks
based on the very occasional occurrence of leprosy among young infants. The maximum
incubation period is as long as 30years, or over, as it is observed, (Joplin, 2008).
1.2 Statement of the problem
Over the years, leprosy has been under researched. This has lead to adverse effect towards
enlightening the society about the disease. As a result, there has been several misconception
or misunderstanding by the people and society causing negligence of the infected patients.
The need for this research has arise, so as to educate the society about the disease, the various
causes and the prevalence rate of the disease over time, and the possible control measures
using Time series analysis.
2. 2
1.3 Aim and objectives
The main aim of this dissertation is to find out the pattern of incidence of leprosy disease as
seen in National Tuberculosis and Leprosy Center, Zaria between January 2005 and
December 2014 and objectives are:
i) To examine and forecast the prevalence of the disease
ii) To analyze and present the age distribution amongst reported cases
iii) To obtain an estimate of gender distribution amongst reported cases
iv) To determine the cause of the disease and provide a possible control measures
1.4 Scope and limitation of the study
The scope of this study is a review case of leprosy treated at the National Tuberculosis and
Leprosy Training Center, Saye Between 2005 - 2014. The means of reviewing in this study
were through the study of hospital case notes and treatment cards from the medical records
office.
1.5 Justification of the study
The findings of this research will help in establishing the performance of the scheme and to
find out about operational problem facing the leprosy control program. This gives a new
insight about better understanding the leprosy disease, means of infection and measures to set
so as to regulate the epidemic of the disease. That will encourage eliminating leprosy as a
public health issue, reducing the stigmatization associated with the disease once people have
been equipped with the necessary knowledge and understanding of the leprosy phenomenon.
Improvement can be implemented and also serve as a good reference to future researchers.
3. 3
1.6 Definition of term
Mycobacterium leprea: -Agent of leprosy; the small brick-red rods in clusters, taken from a
skin lesion which causes leprosy
Granulomatus disease: - This is an inherited disorder in which immune system cells do not
function properly.
Mucos: - This a mucous membrane involved with absorption and secretion at several place
contiguous with skin: at the nostrils, the lips of the mouth, the eye lids, the genital area, and
the anus.
Armadillos: - An animal carrier of leprosy, naturally infected with the disease, bacterial
transmission to people can occur when we handle or eat the animal.
4. 4
CHAPTER TWO
LITERATURE REVIEW
2.1 Conceptual framework
Leprosy has tormented human existence throughout recorded history. The earliest
possible account of a disease that many scholars believe is "leprosy", which is a disease that
has been with mankind from time immemorial, (ILEP, 2015). While in the past it was
regarded as incurable, hereditary, the disease has benefited immensely from scientific
research and breakthroughs that have now made a cure possible. Notably, the major
breakthrough owes much to the works of Norwegian physician, Gerhard Armauer Hansen,
who identified the bacterium that causes the disease. Though from the on-set, leprosy has
been feared and misunderstood as most believes is hereditary disease, a curse, or a
punishment from God. Before and even after the discovery of its biological cause, leprosy
patients were stigmatized and shunned. In Europe during the middle Ages, leprosy sufferers
had to wear special clothing while modern time’s leprosy treatment occurs in separate
hospitals because of the stigma of the disease, (Joplin, 2008).
Leprosy, also known as Hansen’s disease, is an infectious disease caused by a slow-growing
type of bacterium (bacillus) known as Mycobacterium Leprae. The disease, which is
associated with severe disability and social stigma, affects the skin, peripheral nerves outside
the brain, the spinal cord and the upper respiratory tract. The main symptoms include the
appearance of disfiguring skin sores, lumps and bumps that last for weeks or months. Nerve
damage results in loss of feelings in the arms and legs as well as the weakening of muscles.
Ultimately, the patient ends up with major disabilities. Contracted through frequent contacts
with droplets from the nose and mouth of an infected but untreated persons, it normally takes
three to five years for the symptoms to manifest. In some cases, this incubation period could
5. 5
stretch to 20 years. Although not highly infectious, children are considered more susceptible
to leprosy infection than adults, (WHO, 1999).
Through the concerted efforts of the World Health Organization(WHO) and international
donor agencies has helped achievement of the drastic reduction in the number of leprosy
patients, from 5.2 million in 1985 to a mere 189,000 by 2012. Rather than keep pace with the
global trend, Nigeria has been losing the battle to contain the disease.
Nigeria adopted multi-drug therapy as the means to treat persons affected by leprosy
in 1993. Among the control program is the long term plan of providing community-based
treatment programs. Of those who have left colonies, some are living in roadside huts and
begging from passing motorists. A study conducted in 2002, revealed health workers
knowledge of leprosy to be inadequate and identified the need for suitable training programs
on leprosy. The country achieved less than one case of leprosy per ten thousand people in
2003. However, since then it has been struggling to overcome discrimination against people
with obvious signs of the disease and to address the disability it causes. Many find it hard to
seek help because they fear being stigmatized. In 2006 Nigeria was one of seven countries in
Africa reporting more than 1,000 new cases a year, (ILEP, 2015).
Today, there are plans to enhance control measures into the tuberculosis and leprosy program
so as to facilitate early case detection of the disease. Though, patients with leprosy are still
many and there is still complication in the control of leprosy.
According to Udo (2014), in no country so far as we know is the incidence of leprosy
so far as Nigeria. Leprosy is infectious but not contagious; it is only a person with untreated
leprosy than can transmit the diseases. Once treated with antibiotics (Multi Drug Therapy),
the person is free of the bacteria,” leprosy remained a disease of public health importance in
Nigeria as it constitutes serious causes of high morbidity and mortality. The social stigma
6. 6
associated with these diseases further compounds the problem. The effort of the Government
of Nigeria in the fight against these diseases is being supported by the following development
partners: World Health Organization (WHO), The Leprosy Mission Nigeria (TLMN),
Netherlands Leprosy Relief (NLR), and other voluntary organization for the effective
implementation of the National Tuberculosis and Leprosy Control Program (NTBLCP).
The fact that it is curable encouraged the World Health Assembly, in 1991, to pass an
ambitious resolution to eliminate leprosy as a public health problem by 2000. As at 1997,
Nigeria had already eliminated leprosy in all states except in Taraba state. The strategy
employed by Nigeria was based on early detection and treatment, with considerable level of
success witnessed so far has been made possible by the use of a multi drug therapy. The
health ministry should come out with a policy that would also lead to an increase in the
number of skilled workers providing services for the patients, (Chukwu, 2014).
Since early detection and treatment are very important, efforts should be made to
reduce stigmatization so that infected people can come out on their own and seek treatment.
In cases where people have been cured, there should also be efforts to re integrate them so
that they can be useful both to themselves and the society. Nigeria should move out of a
situation where infectious diseases, especially those with identifiable cure, continue to be a
health burden, (Rose, 2012).
In a goal of eradicating the disease, the Government launched the National
Tuberculosis and Leprosy Control Program to control the increasing prevalence of
tuberculosis and leprosy. The Control Program was launched in 1989, but became fully
operational in 1991. Between 1991 and 2012, a total of 111,788 leprosy patients have been
successfully treated.
7. 7
This institution called the National Tuberculosis and Leprosy training centre Zaria, receives
financial and technical support from ILEP, for training and re-training LGA supervisors,
State control officers and every other personnel essential for effective program
implementation. Although, the National policy is for program staff to be retrained at yearly
intervals to ensure they stay abreast with new developments in the field, this policy has not
been implemented as desire, (NTBLC, 2013).
Notable individuals who participated immensely in the advances of leprosy treatment:
Hogerzeil 1955; Well known for its trials in anti-leprosy medicines, Lowe 1947; pioneer the
use of dapsone as a new drug for leprosy taken by mouth (until then most treatment was
given by injection).
2.2 The cause of leprosy
Leprosy is caused by a specific germ (mycobacterium leprea), discovered in 1873 by
Hensens in Norway. In those days leprosy was thought to be hereditary disease or a
punishment from God. Hensen (1868), working in a leprosy Hospital at Bergen in Norway,
did not believe in this theory in his spare time; he used to study specimen tissues of leprosy
patients with a microscope. He observed brown rods in tissues fixed with osmic acid, which
he believed were the causative germ of leprosy, at the age of thirty three he published the
results of the studies. Hansen's discovery was accepted six years later by Albert Niesser of
Germany who, in 1879, at the age of twenty four, stained the organism with fuchsine and
gentian violet. This was before Robert Koch demonstrated the tubercle bacillus. The leprosy
bacillus closely resembles the tubercle bacillus, which causes Tuberculosis, and was the first
bacillus identified as the cause of chronic human disease. After the discovery of the leprosy
bacilli, Hansen not only tried hard to grow them on artificial media in the laboratory but also
made repeated unsuccessful attempts to infect himself as well as his chief and father-in-law,
Danielson, with the materials from leprosy infections patients. Because of his firm faith in the
8. 8
hereditary theory of the causation of leprosy, Danielson was sure that Hansen's experiment
would fail and he agreed to be inoculated with leprosy bacilli. Danielson had 4 inoculations
and as he had expected, all ended in negative result because leprosy is not easily
communicable. Leprosy bacilli are straight or slightly curved rod-like bacteria. In stained skin
smears or sections, they are seen lying single as pink lines, in clumps or in bright pink
compact masses know as "Globi".
Although the discovery of leprosy bacilli was reported as early as 1873, they can still not be
grown on artificial culture media in the laboratory. Leprosy bacilli multiply very slowly.
Therefore their doubling time (generation tome) in the mouse foot pad is 12-13 days 9 the
longest of any known bacterium. In comparison with this, the doubling time of the tubercle
bacillus is only 20 hour, (Norihisa, 2001).
2.3 Epidemiology
Leprosy is most prevalent in tropical countries. This is not due to the climate, because
the disease was formerly also common in cold countries. Because of the fear, shame and
social isolation associated with the disease, leprosy is under reported and some countries are
reluctant to reveal its true prevalence. The exact number of leprosy suffers is therefore not
known. Of the estimated case, Asia has the largest share with about 62% followed by Africa
with about 34%, South America with about 3% and the rest of the world about 1%. However,
in terms of intensity of the disease in the population i.e. mean prevalence of leprosy is at least
one per 1000. Due to the increasing movement of people e.g. Immigrants, refugees, etc.
Leprosy can today occur at least occasionally, anywhere in the world, (Ridley, 2008).
Globally speaking, India has the greatest number of leprosy sufferers the prevalence is
high in the south-eastern Area (e.g. west Bengal) and low in the North- western areas of
9. 9
India. Brazil has the highest number of leprosy sufferers in South America. An occasional
pocket of the disease exists in the USA in Texas, Louisiana and Hawaii.
The WHO targeted leprosy for elimination as a public health problem i.e. reducing
prevalence to less than 1 in 10,000 populations by the end of the year 2000 in 1985; there
were 122 countries with a national prevalence of greater than 1 in 10,000 populations.
Over 85% of all the leprosy cases in the world are concentrated in on six countries in the
following order of magnitude:
1. India2. Brazil 3. Bangladesh4.Indonesia 5.Myanmar 6.Nigeria
Leprosy, which was endemic in western Europe in the medieval period was
eliminated from Scandinavian countries only as the recently as the twentieth century, before
the advent of antibiotic therapy obviously, this decline must be attributed to improvements in
living standards, better housing, cleared supplies and improved nutrition and hygiene.
Currently, very few newly registered patients are found in developing countries and when
detected, a significant proportion of them immigrants from countries where the disease is still
endemic. Today, Leprosy is found mainly in developing countries, around the subtropical and
tropical zone, where the sufficient to support the living standards needed to limit the disease.
10. 10
CHAPTER THREE
RESEARCH METHODOLOGY
3.1 Introduction
This chapter present the method used in this study. The following were covered: methods of
data collection, method of data reduction and method of data analysis.
3.2 Data collection
The data used for the study is a secondary data, taken from the information obtained from
case notes made available from the medical records office for this study. All 474 cases were
collected covering a year period (January 2005 - December 2014). The following items of
information were then extracted from the case notes with respect to patients’ sex, age. The
statistical tool applied in this study is restricted to the time series analysis. Analytical
technique include cross tabulation, simple descriptive statistics such as graph, MINITAB,
Microsoft Excel were used to draw graph and the analysis.
3.3 Methodology
3.3.1 Time series analysis
Time series is a sequence of data points, measured typically at successive times spaced at
uniform time intervals. Examples of time series are the daily closing value of the Dow Jones
index or the annual flow volume of the Nile River at Aswan. Time series analysis comprises
methods for analyzing time series data in order to extract meaningful statistics and other
characteristics of the data. Time series forecasting is the use of a model to forecast future
events based on known past events to predict data points before they are measured. Time
series are very frequently plotted via line charts.
11. 11
3.3.2 Components of Time series
1. Secular or Trend variation (Tt): A times series data may show upward trend or
downward trend for a period of years and this may be due to factors like increase in
population, change in technological progress, and large scale shift in consumers'
demands. Etc
2. Seasonal Variation (St): Seasonal variations are short-term fluctuation in a time
series which occur periodically in a year. This continues to repeat year after year. The
major factors that are responsible for the repetitive pattern of seasonal variations are
weather conditions and customs of people. More woolen clothes are sold in winter
than in the season of summer.
3.3.3 Methods of combining components:
There are 3 methods of combining components considered in time series analysis:
1) Additive model: This model assumes that the actual values are the sum of the 4
separate effects. This assumption is probably true when short period or where the rate
of growth or decline in the trend is small. Additive model is combined in the form;
Xt = Tt + St
2) Multiplicative model: This model suggests that the actual value are the product of
the separate effects, it indicate when there is a sharp growth or decline in a time
series data. Multiplicative model is combined in the form; Xt = Tt * St
3) Mixed model: This include both additive and multiplicative model.
3.3.4 Estimation of trend:
In this project, trend analysis would be computed using the least square method, which is the
most widely used in practice. When this method is applied, a trend line is fitted to data in
12. 12
such a manner that the following two conditions are satisfied: The sum of deviations of the
actual values of y and computed values of y is zero. The fitted line model given by:
Yt = β0+ βtXt + εt
Where Yt: is the observed values in reference to time, β0: is the intercept, βt: is the slope
either decreasing or increasing order, Xt : is the observation over the period of time(t) and εt:
white noise error term.
3.3.5 Estimation of Seasonal Variation:
The method to be adopted in this project is the average percentage method. In this method,
the data for each month is expressed as percentages of the average of the year. The
percentages for corresponding months of different year are then averaged using mean and
must all sum to 1200%. If not, necessary adjustment is done to the means.
3.4 Forecasting: Forecasting is the process of making statements about events whose actual
outcomes (typically) have not yet been observed. A common place example might be
estimation for some variable of interest at some specified future date. There are many types
of forecasting procedures. Forecast in this project is univariate, as it base entirely on past
observations. Linear regression model is used to fit the data and extrapolating.
13. 13
CHAPTER FOUR
DATA PRESENTATION AND RESULT ANALYSIS
4.1 Data presentation
The data of monthly reported cases of leprosy in the National Tuberculosis and Leprosy
center, Saye. Zaria. A secondary data covering a period of 10years collected from the center
and presented for analysis.
TABLE 4.1: Reported Leprosy cases in National Tuberculosis and Leprosy center, saye.
Zaria, from (January 2005 – December 2014)
YEAR MONTH MALE FEMALE TOTAL
2005 January 6 3 9
February 1 2 3
March 5 0 5
April 2 2 4
May 3 0 3
June 2 1 3
July 3 1 4
August 1 1 2
September 1 0 1
October 2 0 2
November 4 2 6
December 2 0 2
2006 January 1 0 1
February 5 0 5
March 6 0 6
April 3 1 4
May 0 0 0
June 3 0 3
July 0 1 1
14. 14
August 3 0 3
September 4 0 4
October 3 0 3
November 6 2 8
December 4 0 4
2007 January 3 0 3
February 11 2 13
March 4 1 5
April 2 2 4
May 4 1 5
June 3 1 4
July 4 3 7
August 5 1 6
September 2 1 3
October 1 1 2
November 1 2 3
December 8 1 9
2008 January 9 0 9
February 3 2 5
March 6 0 6
April 3 2 5
May 3 1 4
June 0 0 0
July 2 2 4
August 2 1 3
September 0 2 2
October 5 2 7
November 0 0 0
December 6 3 9
2009 January 1 2 3
February 5 0 5
15. 15
March 2 2 4
April 3 0 3
May 2 1 3
June 4 1 5
July 1 1 2
August 1 0 1
September 2 0 2
October 3 3 6
November 2 0 2
December 2 1 3
2010 January 1 0 1
February 5 0 5
March 6 0 6
April 3 1 4
May 2 0 2
June 1 0 1
July 1 1 2
August 2 0 2
September 4 0 4
October 3 0 3
November 8 2 10
December 2 0 2
2011 January 1 1 2
February 3 1 4
March 1 2 3
April 2 1 3
May 3 2 5
June 4 5 9
July 0 1 1
August 3 1 4
September 3 2 5
16. 16
October 1 2 3
November 6 2 8
December 0 1 1
2012 January 3 1 4
February 3 0 3
March 4 0 4
April 4 0 4
May 3 2 5
June 2 1 3
July 5 1 6
August 6 3 9
September 5 1 6
October 2 1 3
November 1 0 1
December 4 0 4
2013 January 1 5 6
February 1 2 3
March 1 1 2
April 2 2 4
May 9 1 10
June 2 2 4
July 2 3 5
August 1 0 1
September 0 1 1
October 0 4 4
November 2 0 2
December 4 1 5
2014 January 2 3 5
February 2 0 2
March 1 4 5
April 1 0 1
17. 17
May 2 2 4
June 4 0 4
July 0 0 0
August 4 0 4
September 1 2 3
October 6 6 12
November 1 0 1
December 0 1 1
TOTAL 120 341 133 474
Source: National Tuberculosis and Leprosy center, saye. Zaria
TABLE 4.1.1: Distribution of patients according to age for the study period of (January
2005 - December 2014)
AGE 0-14 15-24 25-34 35-44 45-above Total
Patients 46 85 116 88 139 474
Source: National Tuberculosis and Leprosy center, saye. Zaria
18. 18
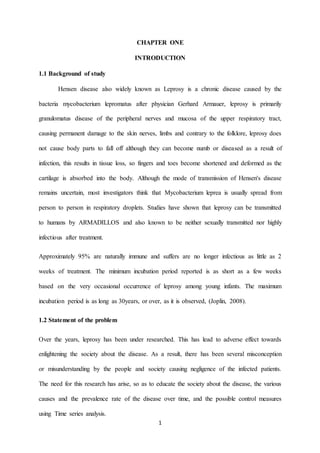
From Table 4.1.1
FIG 4.1.1 Time series plot of distribution of patients according to age
The time series plot in Fig 4.1.1 shows that 45-Above have the highest number of reported
Cases followed by ages 25-34 and 35-44. Ages’ 0-14years has the lowest number of reported
cases as illustrated by the graph for the study period. Generally, children are susceptible to
the disease. Scientific research has shown that infections can occur or travels from person to
person by way of the respiratory tract, through discharges from the nose or mouth, such as
sneezing or coughing. The result of lack of attentiveness to ones’ health status, causes the
body immune system to fight against the bacteria to get weak, as the incubation period, from
the time of infection until the disease sets in, is very long, usually from 1 to 10 years or more.
Children are not exposed to this and that what makes them susceptible, ages 15-24 and 25-34
get more mixed up with the society which inhabits even the infected individuals. All though
95% are naturally immune, the body have tendency to fight of the bacteria. But, lack of
attentiveness to ones’ health status can cause one system to housing the bacteria. Which
manifest in their later years of ages 45- above, ages 35-44 witness a decline as most patients
are discharged and freed from the disease after treatment.
19. 19
TABLE 4.1.2: Average annual infections for the study period of (2005 - 2014)
YEAR 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Patients 4 5 5 3 4 4 4 4 4 4
FIG 4.1.2 Graph of the average annual recorded infections for the study period of (2005
- 2014)
From Fig 4.1.2, year 2007 had the highest number of reported cases. 2008 had a reduction in
the number of reported cases which extended to consequent years.
0
1
2
3
4
5
6
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Numberofpatients
AVERAGE ANNUAL INFECTIONS
20. 20
FIG 4.1.3 Monthly Distribution of patients for the study period (2005-2014) showing the
pattern of incidence of cases in the National Tuberculosis and leprosy center, Saye.
Zaria
Fig I: Graph of Monthly reported leprosy cases in 2005
As shown in the graph of Fig I, January had the highest recorded cases in the center as at
2005. There following months experienced a decrement, but had a sharp increment in
November of the year 2005.
Fig II: Graph of Monthly reported leprosy cases in 2006
0
1
2
3
4
5
6
7
8
9
10
jan feb march april may june july august sept oct nov dec
Numberofpatients
MONTHLY REPORTED CASES IN 2005
0
1
2
3
4
5
6
7
8
9
jan feb march april may june july august sept oct nov dec
Numberofpatients
MONTHLY REPORTED CASES IN 2006
21. 21
The graph in Fig II; shows the highest reported cases to be in the month of November. The
beginning months of the year 2006 had an increment to April, which experienced a decline in
the reported cases. As at the month of May, there were no recorded cases at the center as at
the year 2006.
Fig III: Graph of Monthly reported leprosy cases in 2007
Similar to the previous figures, increment tends to be common with the beginning of the year
(January to March), and maintains a stable decline towards the middle months (April to
September) and again rises at the last part of the year (October to December).
0
2
4
6
8
10
12
14
jan feb march april may june july august sept oct nov dec
Numberofpatients
MONTHLY REPORTED CASES IN 2007
22. 22
Fig IV: Graph of Monthly reported leprosy cases in 2008
The Fig IV above shows highest recorded cases in the months of January and December with
9patients in general, February to October had average of 4patients for the period while
months June and November had no reported cases, as at the year 2008 in the National
Tuberculosis and Leprosy Center, Saye. Zaria.
Fig V: Graph of Monthly reported leprosy cases in 2009
In the Fig V, there was an average of 3 infections for the whole year. The line graph pattern
exhibits a zigzag movement, with its highest cases at 3 points (February, June and October),
months July and September had a tie in the number of patients whole enrolled for treatment at
the center.
0
1
2
3
4
5
6
7
8
9
10
jan feb march april may june july august sept oct nov dec
Numberofpatients MONTHLY REPORTED CASES IN 2008
0
1
2
3
4
5
6
7
jan feb march april may june july august sept oct nov dec
Numberofpatients
MONTHLY REPORTED CASES IN 2009
23. 23
Fig VI: Graph of Monthly reported leprosy cases in 2010
As shown in Fig VI, months May to October experienced the lowest number of reported
cases, the line graph climbed up at the month of November and had a sudden decrease at
December.
Fig VII: Graph of Monthly reported leprosy cases in 2011
In line graph Fig VII, the year 2011 experienced an average of 5 patients and its peak at the
month of June with 9 patients in total.
0
2
4
6
8
10
12
jan feb march april may june july august sept oct nov dec
Numberofpatients MONTHLY REPORTED CASES IN 2010
0
1
2
3
4
5
6
7
8
9
10
jan feb march april may june july august sept oct nov dec
Numberofpatients
MONTHLY REPORTED CASES IN 2011
24. 24
Fig VIII: Graph of Monthly reported leprosy cases in 2012
The peak recorded case was at August with 9 patients and lowest was in the month of
November with 1 patient and an average of 4 patients in total for the year 2012.
Fig IX: Graph of Monthly reported leprosy cases in 2013
The reported cases as seen in the line graph of Fig IX above as of the year 2013 had its peak
recorded cases in the month of May with a total of 10 infections.
0
1
2
3
4
5
6
7
8
9
10
jan feb march april may june july august sept oct nov dec
Numberofpatients MONTHLY REPORTED CASES IN 2012
0
2
4
6
8
10
12
jan feb march april may june july august sept oct nov dec
Numberofpatients
MONTHLY REPORTED CASES IN 2013
25. 25
Fig X: Graph of Monthly reported leprosy cases in 2014
As of the monthly trend of 2014, the disease seems to have been gradually going to
extinction. There have been a fewer reported cases from the beginning of the month, from
January to July which had no cases of leprosy in the center. The plot experienced an irregular
movement in the trend as the month of October had a sharp increment and a sudden decline
in the month of November. This sudden increment could have been as a result of factors
beyond explanation.
In conclusion, the monthly reported cases in the center for the years 2005 to 2014 tends to
exhibit similar pattern of fluctuations as shown in the time series plot above. Most of the
cases are high during the first and last period of the year. The middle part of the years
maintains uniformity as shown in the line graph analysis of above.
0
2
4
6
8
10
12
14
jan feb march april may june july august sept oct nov dec
Numberofpatients MONTHLY REPORTED CASES IN 2014
26. 26
TABLE 4.1.3: Distribution of patients according to gender for the study period (2005 -
2014)
Year 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Male 3 3 4 3 2 3 2 4 2 2
Female 1 0 1 1 1 0 2 1 2 2
FIG 4.1.4 Distribution of patients according to gender for the study period (2005 – 2014)
From FIG 4.1.4, the male have the highest number of reported cases of leprosy infections
than the female. For the study period, the male had 71.94% while the female had 28.06% of
the total population. Although leprosy affects both sexes, in most parts of the world males are
affected more frequently than females often in the ratio of 2:1 (WHO, 2015). As seen by the
graph in FIG 4.1.4, year 2006 and 2010 had no female reported cases, and year 2011, 2013
and 2014 had a tie in the average annual infection cases reported.
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Numberofpatients
AVERAGEYEARLY INFECTION OF GENDER
Male
Female
27. 27
The diagnosis caused an intensely negative emotional reaction among sexes, but self-
stigmatization was greater among women. Women express greater concern than men about
their physical appearance and more often refrained from social activities or even worse,
refusal to report for treatment. The economic activities of women were also more severely
affected, both within and outside at home. Women hid the disease more from their families,
but once they had reported for treatment, they were slightly more likely to complete treatment
regimens than men. Although the majority of all patients were on multidrug therapy (MDT),
a slightly higher proportion of men were on MDT. Women were more concerned about the
side effects of MDT in relation to alteration in skin pigmentation. The above graph of
proportion of gender infections has demonstrated the constraints facing men and women in
relation to leprosy and it makes useful recommendations for health providers and the families
of leprosy patients.
28. 28
4.2 Data analysis
4.2.1 Estimation of Trend
Using the method of least square, the linear model:
Yt = β0+ βtXt + εt
Setting the independent variable (x) as the period (t) and dependent variable (y) as the
patients, SPSS output:
Coefficientsa
Model Unstandardized Coefficients Standardized
Coefficients
t Sig.
B Std. Error Beta
1
Intercept 4.128 .461 8.945 .000
Slope -.003 .007 -.041 -.444 .658
a. DependentVariable:PATIENTS
The trend line model becomes: Yt = 4.128 - 0.003*t
TABLE 4.2.1: Trend of the monthly leprosy reported cases from (January 2005 -
December 2014) in National Tuberculosis and Leprosy center, Saye. Zaria
Period (Xt) Patients (Y) Trend Line Period Patients Trend Line
1 9 4.125 61 1 3.945
2 3 4.122 62 5 3.942
3 5 4.119 63 6 3.939
4 4 4.116 64 4 3.936
5 3 4.113 65 2 3.933
6 3 4.110 66 1 3.930
7 4 4.107 67 2 3.927
8 2 4.104 68 2 3.924
9 1 4.101 69 4 3.921
10 2 4.098 70 3 3.918
11 6 4.095 71 10 3.915
12 2 4.092 72 2 3.912
31. 31
FIG 4.2.1 Graph of the trend movement, in the monthly reported cases of leprosy from
(January 2005 - December 2014) in National Tuberculosis and Leprosy center, Saye.
Zaria
The graph of the long term trend in the monthly leprosy reported cases, which apart from
minor fluctuations; closely approximate a straight line although there is a slight downward
tendency. The fitted trend line in the above graph is on the decrease at a slope of 0.003.
0
2
4
6
8
10
12
14 1
5
9
13
17
21
25
29
33
37
41
45
49
53
57
61
65
69
73
77
81
85
89
93
97
101
105
109
113
117
Numberofpatients
Monthly Index
Trend Analysis of Total Infection
Yt = 4.128 - 0.003*t
32. 32
4.2.2 Estimation of seasonal variation
Seasonal index of the monthly leprosy reported cases from (January 2005 - December 2014)
in National Tuberculosis and Leprosy center, Saye. Zaria; using the average percentage
method, given total infection as:
Jan Feb March April May June July Aug Sept Oct Nov Dec Total: Avg
2005 9 3 5 4 3 3 4 2 1 2 6 2 44 3.67
2006 1 5 6 4 0 3 1 3 4 3 8 4 42 3.5
2007 3 13 5 4 5 4 7 6 3 2 3 9 64 5.33
2008 9 5 6 5 4 0 4 3 2 7 0 9 54 4.5
2009 3 5 4 3 3 5 2 1 2 6 2 3 39 3.25
2010 1 5 6 4 2 1 2 2 4 3 10 2 42 3.5
2011 2 4 3 3 5 9 1 4 5 3 8 1 48 4
2012 4 3 4 4 5 3 6 9 6 3 1 4 52 4.33
2013 6 3 2 4 10 4 5 1 1 4 2 5 47 3.92
2014 5 2 5 1 4 4 0 4 3 12 1 1 42 3.5
Total: 474
The averages become:
Year 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
Total 44 42 64 54 39 42 48 52 47 42
Average 3.67 3.5 5.33 4.5 3.25 3.5 4 4.33 3.92 3.5
33. 33
Dividing each entry by the corresponding monthly averages
yields: For example; January 2005 = 9 ÷ 3.67 = 2.45
February 2005 = 3 ÷ 3.67 = 0.82
March 2007 = 5 ÷ 5.33 = 0.94
And its represented in the table below:
Years Jan Feb March April May June July August Sept Oct Nov Dec
2005 2.45 0.82 1.36 1.09 0.82 0.82 1.09 0.54 0.27 0.54 1.63 0.54
2006 0.29 1.43 1.71 1.14 0 0.86 0.29 0.86 1.14 0.86 2.29 1.14
2007 0.56 2.44 0.94 0.75 0.94 0.75 1.31 1.13 0.56 0.38 0.56 1.69
2008 2 1.11 1.33 1.11 0.89 0 0.89 0.67 0.44 1.56 0 0.44
2009 0.92 1.54 1.23 0.92 0.92 1.54 0.62 0.31 0.62 1.85 0.62 0.92
2010 0.29 1.43 1.71 1.14 0.57 0.29 0.57 0.57 1.14 0.86 2.86 0.57
2011 0.5 1 0.75 0.75 1.25 2.25 0.25 1 1.25 0.75 2 0.25
2012 0.92 0.69 0.92 0.92 1.15 0.69 1.39 2.08 1.39 0.69 0.23 0.92
2013 1.53 0.77 0.51 1.02 2.55 1.02 1.23 0.26 0.26 1.02 0.51 1.23
2014 1.43 0.57 1.43 0.29 1.14 1.14 0 1.14 0.86 3.43 0.29 0.29
Totals: 10.89 11.8 11.89 9.13 10.23 9.36 7.64 8.56 7.93 11.94 10.99 7.99
Mean: 1.089 1.18 1.189 0.913 1.023 0.936 0.764 0.856 0.793 1.194 1.099 0.799
The total mean = 1.089 + 1.18 + 1.189 + 0.913 + 1.023 + 0.936 + 0.764 + 0.856 + 0.793 +
1.194 + 1.099 + 0.799 = 11.835
The mean percentage (%) = 1183.5, the required for each month: 1200
Adjusting to fit the required for each month, we have: 1200 ÷ 1183.5 = 1.014. Then, multiply
each seasonal index by 1.014 to adjust to the required index.
34. 34
The seasonal index becomes:
Table 4.2.2: Seasonal index of the monthly reported cases
Month: Jan Feb March April May June July Aug Sept Oct Nov Dec
Mean: 1.104 1.197 1.206 0.926 1.037 0.949 0.775 0.868 0.804 1.211 1.114 0.81
Total monthly index = 12.001, which is so close to the required 1200, that no adjustment is
necessary.
FIG 4.2.2 Graph of seasonal index in the reported cases of leprosy, from (January 2005
- December 2014) in National Tuberculosis and Leprosy center, Saye. Zaria
As represented in Fig 4.2.2, it shows that there is an increase from the month of January to
March, April to September witness a decrease in the cases and October to December
experienced another increment in the number of reported cases at the center. Scientific
research has shown that leprosy disease is rampant at the tropical region which is warm
throughout the period of the year, this region experiences a period referred to as “Harmattan”.
Nigeria is an example of tropical region which experience the period of Harmattan from
October to February of the year after. As earlier mentioned, transmission of the disease can
0
0.2
0.4
0.6
0.8
1
1.2
1.4
Jan Feb March April May June July Aug Sept Oct Nov Dec
NUMBEROFCASES
SEASONAL INDEX
35. 35
occur from person to person through respiratory tract, this through discharges from the nose
or mouth, such as sneezing or coughing. Inhabitants of the tropical region experience
sneezing and coughing during the Harmattan period. For this reason, leprosy is endemic in the
tropical region, and reported cases are higher during the Harmattan months (i.e. October – February),
as the period masterminds several factors which serve as a mechanism for transmission of
leprosy disease, such as the Cough and Catarrh.
4.2.3 Deseasonalization
In obtaining the deseasonalized data, I adjusted the data for seasonal variation by dividing
entry in the original data by the seasonal index of the corresponding month.
Illustration: The seasonal index of month of January = 1.104, Deseasonalizing for January
2005 = 9 ÷ 1.104 = 8.152, January 2006 = 1 ÷ 1.104 = 0.906. Similar procedure is computed
on the rest of the data to obtain the deseasonalized reported cases shown in the table 4.2.3
below:
TABLE 4.2.3: Deseasonalized monthly leprosy reported cases from (January 2005 -
December 2014) in National Tuberculosis and Leprosy Center, Saye. Zaria
JAN Feb Mar April May June July August Sept Oct Nov Dec
2005 8.152 2.506 4.146 4.32 2.893 3.161 5.161 2.304 1.244 1.652 5.386 2.469
2006 0.906 4.177 4.975 4.32 0 3.161 1.29 3.456 4.975 2.477 7.181 4.938
2007 2.717 10.86 4.146 4.32 4.822 4.215 9.032 6.912 3.731 1.652 2.693 11.111
2008 8.152 4.177 4.975 5.4 3.857 0 5.161 3.456 2.488 5.78 0 11.111
2009 2.717 4.177 3.317 3.24 2.893 5.269 2.581 1.152 2.488 4.955 1.795 3.704
2010 0.906 4.177 4.975 4.32 1.929 1.054 2.581 2.304 4.975 2.477 8.977 2.469
2011 1.812 3.342 2.488 3.24 4.822 9.484 1.29 4.608 6.219 2.477 7.181 1.235
2012 3.623 2.506 3.317 4.32 4.822 3.161 7.742 10.369 7.463 2.477 0.898 4.938
2013 5.435 2.506 1.658 4.32 9.643 4.215 6.452 1.152 1.244 3.303 1.795 6.173
36. 36
2014 4.529 1.671 4.146 1.08 3.857 4.215 0 4.608 3.731 9.909 0.898 1.235
Assume a multiplicative model, the original data is denoted by Yt = Tt * St
Where; Yt = Actual value in time, Tt = Trend component with time, St = Seasonal component
with time. The table above represents the seasonally adjusted data, denoted by Y/S = T, and
thus contain the long term Trend.
4.3 Forecasting
First obtaining the trend equation so as to aid in forecasting, the trend line given as:
Yt = β0+ βtXt + εt
Where; Yt = Number of observations, β0 = intercept, βt = slope with respect to time, Xt =
observations over the period of time (t), 𝜀t = Error residual and t = Time or period.
Estimating the parameters: X = period or time (t), Y = Deseasonalized data
Using the simple linear regression, Intercept (β0) = 3.96605 and Slope (β) = -0.000421. The
trend equation becomes:
Yt = 3.96605 - 0.000421(t), after substituting period (t) into the equation to obtain the trend,
subsequent values is then multiplied by the seasonal component (St) to obtain the forecast as
shown in the table below.
TABLE 4.3: Forecasting for the monthly leprosy cases for period of (January 2015 -
December 2020) in National Tuberculosis and Leprosy Center, Saye. Zaria
Period(t) Years Month
Seasonal
index
Trend
equation Forecast
121 2015 Jan 1.104 3.915 4
122 Feb 1.197 3.915 5
123 march 1.206 3.914 5
124 April 0.926 3.914 4
37. 37
125 may 1.037 3.913 4
126 June 0.949 3.913 4
127 July 0.775 3.913 3
128 august 0.868 3.912 3
129 Sept 0.804 3.912 3
130 Oct 1.211 3.911 5
131 Nov 1.114 3.911 4
132 Dec 0.81 3.911 3
133 2016 Jan 1.104 3.910 4
134 Feb 1.197 3.910 5
135 march 1.206 3.909 5
136 April 0.926 3.909 4
137 may 1.037 3.908 4
138 June 0.949 3.908 4
139 July 0.775 3.908 3
140 august 0.868 3.907 3
141 Sept 0.804 3.907 3
142 Oct 1.211 3.906 5
143 Nov 1.114 3.906 4
144 Dec 0.81 3.905 3
145 2017 Jan 1.104 3.905 4
146 Feb 1.197 3.905 5
147 march 1.206 3.904 5
148 April 0.926 3.904 4
149 may 1.037 3.903 4
150 June 0.949 3.903 4
151 July 0.775 3.903 3
152 august 0.868 3.902 3
153 Sept 0.804 3.902 3
154 Oct 1.211 3.901 5
38. 38
155 Nov 1.114 3.901 4
156 Dec 0.81 3.900 3
157 2018 Jan 1.104 3.900 4
158 Feb 1.197 3.900 5
159 march 1.206 3.899 5
160 April 0.926 3.899 4
161 may 1.037 3.898 4
162 June 0.949 3.898 4
163 July 0.775 3.897 3
164 august 0.868 3.897 3
165 Sept 0.804 3.897 3
166 Oct 1.211 3.896 5
167 Nov 1.114 3.896 4
168 Dec 0.81 3.895 3
169 2019 Jan 1.104 3.895 4
170 Feb 1.197 3.895 5
171 march 1.206 3.894 5
172 April 0.926 3.894 4
173 may 1.037 3.893 4
174 June 0.949 3.893 4
175 July 0.775 3.892 3
176 august 0.868 3.892 3
177 Sept 0.804 3.892 3
178 Oct 1.211 3.891 5
179 Nov 1.114 3.891 4
180 Dec 0.81 3.890 3
181 2020 Jan 1.104 3.890 4
182 Feb 1.197 3.889 5
183 march 1.206 3.889 5
184 April 0.926 3.889 4
39. 39
185 may 1.037 3.888 4
186 June 0.949 3.888 4
187 July 0.775 3.887 3
188 august 0.868 3.887 3
189 Sept 0.804 3.887 3
190 Oct 1.211 3.886 5
191 Nov 1.114 3.886 4
192 Dec 0.81 3.885 3
Fig 4.3: Graph of forecast for the monthly leprosy cases for period of (January 2015 -
December 2020) in National Tuberculosis and Leprosy Center, Saye. Zaria
The above analysis shows that the forecast for (January 2015 - December 2020)
would have an average of 4 infective in total, and also suggest that the total number of
infected persons would lie between 5 at most and 3 minimum for the period of January 2015
and December 2020 in the National Tuberculosis and Leprosy Center, Saye. Zaria. Kaduna
State. The implication of this as suggested by the forecast is that, there would be a continuous
decline in the cases of leprosy in the center. As with time, there are chances of the disease
0
1
2
3
4
5
6
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65 67 69 71
NUMBEROFPATIENTS
MONTHLY INDEX
Forecasting for leprosy cases for period of (January 2015- December 2020)
40. 40
going into extinction as suggested by the above forecast. This is probably as result of increase
in awareness, improvement in medical facilities, sanitation of the environment etc.
4.4 Discussion of results
Leprosy epidemic is on the decrease as seen in the analysis. There has been a monthly
decrease of 0.33% so far from January 2005 - December 2014 in the reported leprosy cases.
Having put all the variation into consideration (Trend, Seasonal, Cyclical and Irregular
variations), I was able to forecast using time series analysis the number of cases between
January 2015 - December 2020 to be at maximum of 5 and minimum of 3 cases of patients,
with an average of 4 leprosy cases per month in the National Tuberculosis and Leprosy
Center, Saye. Zaria
The method adopted for forecasting in the analysis is using Deseasonalized data to obtain a
trend equation, where X = period (t), (ranging from 1 - 120) and Y = Deseasonalized data,
then a simple linear regression was computed using Microsoft excel, to obtain the trend
equation. Values of the forecasting period ranging from 121 - 192 is then substituted in to the
trend equation to get the trend values, which only contains the trend or secular variation. In
other to obtain the forecast estimate, trend values is then multiplied with the seasonal
component which corresponds to the multiplicative model (Yt = Tt * St).
41. 41
CHAPTER FIVE
SUMMARY OF FINDINGS, CONCLUSION AND RECOMMENDATION
5.1 Summary of findings
The study shows that the male gender is mostly affected by the scourge due to the fact that
most of the distributions gotten from cross tabulation indicate that the male has a higher
prevalence than the female. Leprosy epidemic is on the decrease as seen in the research.
WHO reported that, there is a decrease in leprosy cases according to report, in Nigeria there
was a 91.95% decrease in leprosy cases from 1990 – 1997, (WHO, 1990).
Distribution in terms of age indicates that the disease is high among the age group of 40 and
above. A major reason for the high prevalence among this group is due to late report by
patients, due to late coming of people, illiteracy. There are few cases of infection among
people with age group of 0-14. Awareness about leprosy was quite high in Kaduna with 70%
of the people having heard about LEPROSY. Specific detailed knowledge about LEPROSY
was average, but there is still need to translate the knowledge to enable adopt preventive
behavior.
Finally the analysis clearly states that the leprosy epidemic is affected by seasonal variations,
and there is presence of irregularities in the movement of the series as anyone can be infected
by leprosy disease contrary to the most believe that it is heredity. The leprosy case is on the
decrease, though the decrease is small or slightly, without any fluctuation, the number of
leprosy cases will be reduced to barest minimal if decrease is kept at constant.
42. 42
5.2 Conclusion
One of the major challenges facing leprosy epidemics is the monitoring, evaluating and
reporting of leprosy activities and their impact. Adequate measures should be taken to reduce
the rate of infections of the virus by proper collection, analysis, dissemination and utilization
of data and information in order to check mate the scourge.
The analysis shows that the present elimination strategy will reduce transmission, although
the decline may be slow. Early case detection is the key factor in the success of the strategy.
If the target of elimination of leprosy as a public health problem is set to be achieved in all
countries is justified, a long term strategy for leprosy control should be adopted.
43. 43
5.3 Recommendation
The following recommendations is made in respect to the research and discussions made
above
1. The private sector should be more involved in the awareness and prevention of
leprosy due to fact that government cannot tackle the scourge alone. There should be
more public-private partnerships involved in the struggle for a leprosy free generation.
2. More sentinel surveys should be conducted to monitor the trend of the epidemic;
surveys should always be carried out on male and female at a time of attendance.
3. I will recommend that the entire surveys should be carried out annually with quarterly
assessments reports to obtain accurate statistics on the rate of infection.
4. The federal government should also carry out behavioral sentinel surveys of high risk
groups including sex workers. The National Population Commission (N.P.C) should
be actively involved in carrying out sentinel surveys periodically which will help
inform the denominator in many of the core indicators that are chosen. The
commission should also intensify demographic health surveys taken in order to
provide vital data.
5. Finally, research work on LEPROSY should be supported in which the management
information system (MIS) should provide continuous flow of data and information
from various program sites and decision makers and program managers, Central
database system using appropriate software should be established and encouraged in
order to facilitate research work.
44. 44
REFERENCES
African journal, (2008) Role of Substance Abuse in the African Leprosy Epidemic.
Chatfield, C. (1997), Analysis of Time Series: Theory and Practice.
Hamilton J.D, (1994) Time series analysis, Princeton University press. (Chapter 3,4,5,6).
Harvey, A. (1993), Time series models, London: Harvester, (chapter 8)
Muir, E. (1944) Preliminary Report on Diasone in Treatment of Leprosy, International
Journal of Leprosy 12:1-6.
Norihisa Ishii. (2001) Recent Advances in the treatment of Leprosy, Dermatology Online
Journal. 9(2):5
Ridley D.S. and W.H. Joplin 1996, Classification of Leprosy According to Immunity- A five
group system, International Journal Leprosy; 54:255-73
The Nigerian Journal of Guidance and Counseling II (2008), Pp. 118-176.
World Health Organization (WHO). Leprosy - global situation. Weekly epidemiological
record 2000; 75:226-31.
World Health Organization (WHO), Trend in Leprosy detection.Weekly epidemiological
record 1998; 73; 169-75.