
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Giant cell tumor
Similar to Giant cell tumor (20)
Recently uploaded
Recently uploaded (20)
Giant cell tumor
- 1. GIANT CELL TUMOR Dr. PATEL YAHYA ISMAIL
- 2. INTRODUCTION One of the most common bone tumors Benign tumor, but locally aggressive and has malignant potential First described by Sir Astley Cooper in 1818
- 3. DEFINITION Neoplasm arising from non-bone forming supportive connective tissue of marrow with network of stromal cells regularly interspersed with giant cells Tumor is called GCT because Giant cells are found These Giant cells resemble osteoclasts, hence called as OSTEOCLASTOMA
- 4. EPIDEMOLOGY Only 5% of PRIMARY bone tumors & 20% of benign bone tumors Skeletally mature patients in the age group of 15 to 40 with peak incidence in later half of 3rd decade Female to male ratio 1.5 : 1 But malignant GCT more common in MALES GCT of small bones occur in younger age group with high incidence of multicentricity
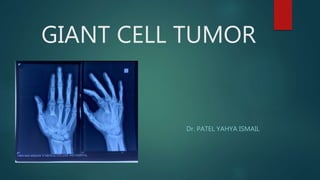
- 5. SITE OF INVOVLMENT Solitary or multicentric (1%) 1. distal end of femur 2. proximal end of tibia 3. distal end of radius 4. upper end of humerus 5. lower end of tibia cancellous disposed bone ends which are sites of high bone turn over & osteoclastic activity Others like hand , spine and pelvis
- 6. CLINICAL FEATURES 1. SWELLING : An epiphyseo- metaphyseal , eccentric swelling is seen at the ends of long bones Overlying Skin is stretched & shiny but no engorged veins On palpation, swelling is warm ,tenderness present with bony consistency EGG SHELL CRACKLING may be elicitable when there is too much thinning of cortex/pathological fracture
- 7. CLINICAL FEATURES PAIN : Vague persistent pain at the end of long bones in relation to activity of the joint Pain may increase after a pathological fracture Limitation of joint movements due to mechanical block Pathological fracture : usually uni-cortical than a complete Neurological deficit may be seen in cases involving the spine and sacrum. Metastasis is present in 1-5% cases. most common site being lung..k/a LUNG IMPLANTS
- 8. INVESTIGATIONS serum calcium, phosphorus, ALK.PHOSPHATASE To rule out hyperparathyroidism
- 9. PLAIN RADIOGRAPHS Epiphyseo-metaphyseal Expansible lesion Eccentrically situated Confined to bone cortical break-through indicates more aggressiveness of tumor Lysis with or without trabeculations giving rise to soap bubble appearance Geographic distribution rarely extending to articular cartilage Absence of margin of bone sclerosis or punctuate calcification Absence of intra- lesional bone formation or ominous periosteal reaction
- 10. COMPUTED TOMOGRAPHY Confirms the integrity of cortex and outline tumor extent Sub-cortical destruction can be well appreciated Soft tissue extension & relationship to adjacent structures cannot be studied!!
- 11. MRI Morphologic analysis & extent of tumor can be assessed. Intra-medullary tumors are best seen in T1 weighted images Extra osseous portion is best appreciated on T2 weighted images
- 12. ANGIOGRAPHY Not routinely done To assess the relationship of major vessels to large tumors To know major feeding vessels to tumor
- 13. BONE SCAN Gct takes up increased uptake of technetium 99 Does not correlate to grading or nature of tumor Useful when multi-centric lesions suspected
- 14. BIOPSY Final diagnostic tool for GCT 1. Types FNAC (22 GAUGE NEEDLE) 2. CORE NEEDLE BIOPSY (14 GAUGE NEEDLE) 3. OPEN INCISIONAL BIOPSY
- 15. OPEN INCISIONAL BIOPSY Reliable Allows pathologists to evaluate cellular morphologic features & tissue architecture from different sites of lesion Use the smallest longitudinal incision Use a cautery knife & avoid crushing specimen texture Use meticulous heamostasis
- 16. PATHOLOGY : GROSS APPEARANCE EARLY LESION: Homogenous ,friable ,reddish brown mass LATE LESION: Variegated appearance ,blood filled areas
- 17. HISTIOGENESIS & MICROSCOPY Composed of many multi-nucleated Giant cells (40-60 nuclei/cell) in a sea of mono- nuclear stromal cells Stromal cells are the main neoplastic component of the tumor which regulate giant cell mediated bone destruction. Nuclei of stromal cells are identical to that of nuclei of giant cells, a feature that distinguishes from other tumors containing giant cells
- 18. HISTIOGENESIS & MICROSCOPY Stromal & giant cells in the GCT contain ACID PHOSPHATASE (TUMOR MARKER) Where as other giant cell variants contains ALKALINE PHOSPHATSE Areas of storiform spindle cell formation, reactive bone formation or foamy macrophages may be seen Secondarily ANEURYSMAL BONE CYSTS may be present Indicators of aggressiveness: Increased no. of stromal cells, hyperchromatism, greater mitotic activity
- 19. GRADING OF GIANT CELL TUMOR CAMPANNCI’S RADIOGRAPHIC GRADING JAFFE et al PATHOLOGICAL GRADING ENNEKING STAGING OF GCT
- 20. CAMPANACCI RADIOGRAPHIC GRADING GRADE I: CYSTIC LESION GRADE II: Expansile lytic lesion with THIN CORTEX but no break in cortex GRADE III: Destructive radiolucent lesion with cortical break and soft tissue extension
- 21. JAFFE et al PATHOLOGICAL GRADES Based on mitosis & atypia of stromal cells GRADE 1: numerous giant cells mononuclear cells are rare mitotic activity is absent GRADE 2: mononuclear cells are numerous moderate atypia & mitotic activity GRADE 3: giant cells are few& small atypia & pleomorphism are common high mitotic activity
- 22. ENNEKING : STAGING OF GCT
- 23. GIANT CELL TUMOUR VARIANTS 1.Brown tumor of hyperparathyroidism Osteopenia, sub-periosteal resorption, resorptive changes at distal phalanges loss of lamina Dura of teeth Elevated AKP & serum calcium levels & Decreased phoshophorus levels
- 24. 2.Chondroblastoma adolescent with open physis polygonal stromal cells multiple punctuate calcifications CHICKEN WIRE APPEARANCE on radiograph 3.Aneursymal bone cyst 75% located in metaphysis double density fluid-fluid level on CT/MRI • 4.Unicameral bone cyst below 20 years of age metaphyseal lesion fallen fragment sign on radiographs
- 25. 5. Giant cell rich osteosarcoma metaphyseal lesion aggressive bone destruction ill-defined margin 6.Chondromyxiod fibroma metaphyseal lesion 10 to 30 age group pseudo-trabeculations are denser & thicker 7. Non-ossifying fibroma less than 15 years age open physis metaphyseal or diaphyseal lesion well defined scalloped margins rim of reactive host bone sclerosis
- 26. TREATMENT The Tumour Is Invasive And Aggressive It commonly recurs, may become malignant after unsuccessful removal. Recurrence is treated with en bloc excision. En bloc excision is also indicated if the tumour has eroded the cortex and extended into the soft tissues. Eradicate the growth completely at the initial surgery
- 27. PRE-OP PLANNING Malignancy should be ruled out by prior biopsy and other investigation. OPERATIVE PLAN MUST INCLUDE THIS THREE FACTORS 1.type of resection. 2.The use of adjuvant therapy 3.Type of material to be used to fill the defect
- 28. TREATMENT OPTIONS SIMPLE CURETTAGE: Intra- lesional curettage alone EXTENDED CURETTAGE : curettage along with use of adjuvants to augment curettage EN BLOCK EXCISION IRRADIATION THERAPY EMBOLISATION BISPHOSPHONATES AMPUTATION
- 29. INTRA LESIONAL CURRETAGE Adequate exposure with large cortical window High power burr Pulsatile jet lavage Curettage alone has high recurrence rate
- 30. ADJUVANTS TO CURRETAGE Advantage of using adjuvants It eliminate the microscopic disease and reduces recurrence Curettage and cementation causes a 2mm osteolytic lesion zone surrounding the cement due to thermal injury PHENOL-12-50% conc Easily absorbed Nephrotoxic Soft tissue complication HYDROGEN PEROXIDE
- 31. ADJUVANTS TO CURRETAGE PMMA BONE CEMENT Bone cement +ADRIAMYCIN+METHOTREXATE to reduce recurrences PRINICIPLE: heat of polymerization or direct toxicity of monomer CRYOSURGERY WITH LIQUID NITROGEN it create 1-2cm zone of tissue necrosis. Local complicationS 1. thermal shock, 2. dehydration, 3. wound healing problems Not easily available & costly Storage difficulties
- 32. RECONSTRUCTION OF RESIDUAL DEFECT Bone grafting autogenous bone graft allograft artificial bone graft substitutes demineralised bone matrix Bone cement
- 33. BONE GRAFT ADVANTAGE DRAWBACK Remodelling along stress lines Auto graft quantity is less Reconstruction is permanent Donor site morbidity Restores bone stock Allograft is expensive..requires bone bank Restores normal biomechanics at joint surface Recurrence is difficult to distinguish from graft resorption
- 34. PMMA BONE CEMENT ADVANTAGE DISADVANTAGE Immediate structural support and early ambulation MMA monomer is cytotoxic Thermal effect Radiographic detection of recurrence is easier Not a biological material. Though strong in compression but weak when subjected to shear and torsional forces Fear of long term degeneration of articular cartilage in sub-chondral lesion in wt bearing stress
- 35. SANDWICH TECHNIQUE when tumor is <1cm from articular surface, the incidence of degenerative changes in cartilage after the use of cement alone is 2.5 times greater than when tumor is >1cm away In such conditions, multilayer reconstruction technique is recommended Interposing bone graft between the cartilage & cement reduces heat damage and the resultant degenerative changes
- 36. EN BLOC RESECTION AND SUBSEQUENT RECONSTRUCTION/ARTHODESIS Initial procedure of choice in more aggressive tumors. 2 cm of normal tissue is also excised. Defects are filled with cancellous bone grafts, freeze dried allografts or prosthesis. This technique has low recurrence rate
- 37. Resection :Indications stage 3 lesions cortex destroyed and soft tissue extension present Recurrences Large defects are expected Joint surface destroyed or cannot be salvaged Certain bones which can be sacrificed such as Lower end of ulna Upper end of fibula
- 38. RECONSTRUCTION OPTIONS BIOLOGIC AUTOGRAFT ARTHRODESIS LIVE MICROVASCULAR FIBULAR GRAFT OSTEO-ARTICULAR ALLOGRAFTS ILIZAROV METHOD ENDOPROSTHETIC JOINT REPLACEMENT eg: custom mega prosthesis
- 39. EMBOLISATION Trans-catheter Embolisation of blood supply of Certain un-resectable tumors like sacrum & pelvis PREOP EMBOLIZATION also Brings down size of tumor & provides pain relief Re-embolisation needed at monthly intervals
- 40. AMPUTATION Malignant tumour Fungation Recurrence after surgery and irradiation Deep seated associated infection Extensive destruction of bone Severe disability
- 41. RADIOTHERAPY When complete excision or curettage is not possible Aggressive, multiple/ recurrent tumor Lesions of spine & sacrum The recommended dosage is 1,500 to 5,000 rads for 5 to 6 weeks using mega voltage therapy cobalt 62 It may induces malignant change if it is given to the benign lesion
- 42. BISPHOSPHONATES Pamidronate / Zoledronate can be given They target osteoclast-like giant cells. Limit tumor progression
- 43. THANK YOU