
Recommended
More Related Content
What's hot
What's hot (20)
Similar to EUS in Pancreatic cystic lesions.pptx
Similar to EUS in Pancreatic cystic lesions.pptx (20)
Recently uploaded
Recently uploaded (20)
EUS in Pancreatic cystic lesions.pptx
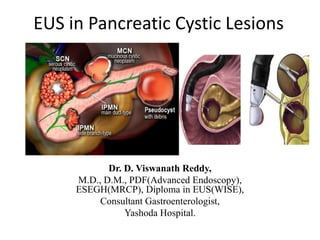
- 1. EUS in Pancreatic Cystic Lesions Dr. D. Viswanath Reddy, M.D., D.M., PDF(Advanced Endoscopy), ESEGH(MRCP), Diploma in EUS(WISE), Consultant Gastroenterologist, Yashoda Hospital.
- 2. Synopsis • PCLs – Magnitude, Types • Challenge: Benign or Malignant!, Surgery? • Radiology • EUS-Diagnosis of PCLs • Newer tools • EUS in Therapy of PCLs • Case snippets
- 3. PCLs • 2–45% of general population(24% Autopsy) • Reported prevalence 2.1–2.6% for CT & 13.5–45% for MRI/MRCP. • Age, Asians, Pancreatitis, Family history.... • Incidental, Asym., benign malignant. • Earlier 40% resection was of benign, still ~15-20% • Early detection paramount for early treatment.
- 6. • 45 year old ethanol consumer presented with acute abdominal pain 4 weeks back with SIRS recovered and now has persistent pain.
- 7. Pseudocyst • 20%-49% • 5th decade • 7:3 Body/tail > Head/uncinate • Well-defined • Peripancreatic fluid collection of homogenously low attenuation
- 9. Case: 50 year old female, nonalcoholic, nonsmoker with pain abdomen, jaundice or weight loss. Lap. Chole. done considering Biliary Pancreatitis. Collection considered as Pseudocyst. • Well-defined, unilocular/ • Macrolacunae • Mural Nodule/mass
- 10. Mucinous Cystadenoma • 11-18% • 5th decade • 1:9 M:F • Body/tail > head/uncinate • Well-defined, unilocular/ • Macrolacunae • Peripheral rim of calcification • CEA >192; String Sign; Cytology • High malignant potential
- 11. Serous cystadenoma • 13-23% • 6th decade • 4:6 M:F • Head/uncinate = body/tail • Well-defined • Small cysts separated by delicate septa • Central stellate scar with sunburst pattern of calcification • CEA<5; Amylase-low • Low malignancy potential
- 13. MD-IPMN • 21-33% • 7th decade • 6:4 M:F • Head/uncinate > body/tail • Distended pancreatic duct • Polypoid intraductal lesion • Patulous ampulla with mucin extrusion • CEA>192; String Sign • High malignancy potential 60 year old male presented with pain abdomen s/o Acute pancreatitis.
- 14. BD-IPMN
- 15. SPEN • 2% • 3rd decade • 1:9 M:F • Body/tail > head/uncinate • Well-defined • Heterogeneous-appearing mass with solid and cystic areas • High malignancy potential
- 16. Cystic PNET • 4-7% • 6th decade • 5:5 M:F • Body/tail > Head/uncinate • Well-defined • Heterogeneous-appearing mass • with solid and cystic areas • Hypervascular cyst rim
- 18. EUS- Mural Nodule vs Mucus Plug • Mucus – hypoechoic & smooth, hyperechoic rim • Nodules - iso- or hyperechoic without hyperechoic rim or smooth edge • Rotating patient & try move lesion with FNA needle can help to differentiate mucus vs nodule. • CH-EUS enhancement in nodule, not if mucus. • The sensitivity and specificity of EUS (75% and 83%) were superior to CT (24% and 100%) for nodules, and surpasses diagnostic yield of MRI
- 19. Current Diagnostic Approach • History • Initially- Non-invasive imaging-CT/MRI • EUS – Fluid analysis- Biomarkers, cytology. – Biopsy – Molecular analysis
- 20. Radiology • Combining MDCT and MRI, the accuracy of predicting malignancy of a PCL increased from 61% (CT) to 81% • Accuracy for identifying the specific type of PCN is between 40% - 95% for MRI/MRCP and between 40% and 81% for CT • MRI/MRCP is preferable – Better to evaluate septa, nodules, – Main duct, branch duct involvement, communication with MPD and – Cyst contents/debris; 79%-82% accurate in identifying mucinous cysts. • 18-FDG PET/CT had sensitivity of 57–94%, specificity of 65– 97% and accuracy of 94% in benign vs malignant cysts. European evidence-based guidelines on pancreatic cystic neoplasms; Gut. 2018 May; 67(5): 789–804. 10.1136/gutjnl-2018- 316027 Kadiyala V, Lee LS. Endosonography 24in the diagnosis and management of pancreatic cysts. World J Gastrointest Endosc 2015; 7(3): 213-223 [PMID: 25789091 DOI: 10.4253/wjge.v7.i3.213]
- 21. EUS scores over Radiology • EUS is recommended as an adjunct to other imaging modalities (GRADE 2C) • EUS with or without cyst fluid aspirate analysis more sensitive (76%) than CT or MRI (48% and 34%) differentiating neoplastic vs non- neoplastic cysts. Khashab MA et al. Should we do EUS/FNA on patients with pancreatic cysts? The incremental diagnostic yield of EUS over CT/MRI for prediction of cystic neoplasms. Pancreas. 2013;42:717- 721.
- 22. Glucose level(<50mg%) in PCF is better than CEA(94 vs 85%) for preoperative diagnosis of mucinous cysts. McCarty T.R., Garg R., Rustagi T. Pancreatic cyst fluid glucose in differentiating mucinous from nonmucinous pancreatic cysts: A systematic review and meta-analysis. Gastrointest. Endosc. 2021
- 23. EUS-FNA • EUS-FNA should only be performed if change in management expected(GRADE 2C). • No - if diagnosis is established by imaging, or where clear indication for surgery (GRADE 2C). • Relative contraindications-distance of >10 mm • EUS-FNA for PCN is safe procedure with relatively low risk (3.4%) of complications.
- 24. Antibiotic before FNA of PCL? • One retrospective study of 253 patients found antibiotic prophylaxis had no effect on risk of infection (7% vs 9.3%), although conclusive evidence is lacking. • Current practice is single shot antibiotic treatment prior to EUS-FNA of a cystic lesion.
- 25. Newer tools • Contrast EUS – Mural Nodules, – Assess vascularity in cyst & septa – Sonazoid>Sonovue -EUS-FNA of pancreatic cysts sensitivity 54% for mucinous versus non-mucinous cysts, - 44% - 78% when more passes from solid component. - 84.2% sensitivity when CH-EUS-FNA from fluid analysis & mural nodules.
- 26. Other tools • Moray Forceps – cyst tissue acquisition yield 90% – 83.7–88.6% sensitivity and 81.8–94.7% specificity for mucinous PCN – adverse events was 8.6–9.9% • Confocal Laser endocytoscopy(nCLE) • Molecular analysis(NGS): 4mutations: – KRAS, GNAS, VHL and one other (PIK3CA, TP53, SMAD4, PTEN, CDKN2A) • Artificial Intelligence – Imaging – EUS – Fluid analysis
- 29. EUS guided Therapy for PCLs • ?Alternative to surgery in poor / reluctant surgical candidates and low-risk in cases where malignant potential is uncertain. • Ethanol lavage • Paclitaxel stabilizes microtubule polymer to inhibit its disassembly & induce apoptosis. • RFA • Cryotherapy • Benign with no malignant features, 2-4 cm, uni/oligolocular, and no connection with MPD. • Post procedure pain, Pancreatitis, intracyst bleed, infection, Peritonitis. • EUS-guided therapies for IPMNs should not be performed outside trials.
- 31. Current Guidelines on PCLs
- 33. Summary • Increasing prevalence of PCLs recently. • Accurate diagnosis & risk stratifying paramount. • Multimodal diagnosis, EUS complementary. • EUS scores higher with FNA, Biopsy. • Fluid biomarkers and Molecular testing key • Newer tools promising. • F/U- No-surveillance, Surveillance or Surgery. • Therapeutic role of EUS in PCLs needs evidence.
- 34. Thank You