
Recommended
Recommended
More Related Content
Similar to (NR326 Mental Health NursingRUA Scholarly
Similar to (NR326 Mental Health NursingRUA Scholarly (15)
More from VannaJoy20
More from VannaJoy20 (20)
Recently uploaded
Recently uploaded (20)
(NR326 Mental Health NursingRUA Scholarly
- 1. ( NR326 Mental Health Nursing RUA: Scholarly Article Review Guidelines )Purpose The student will review, summarize, and critique a scholarly article related to a mental health topic. Course outcomes: This assignment enables the student to meet the following course outcomes. (CO 4) Utilize critical thinking skills in clinical decision- making and implementation of the nursing process for psychiatric/mental health clients. (PO 4) (CO 5) Utilize available resources to meet self-identified goals for personal, professional, and educational development appropriate to the mental health setting. (PO 5) (CO 7) Examine moral, ethical, legal, and professional standards and principles as a basis for clinical decision-making. (PO 6) (CO 9) Utilize research findings as a basis for the development of a group leadership experience. (PO 8)
- 2. Due date: Your faculty member will inform you when this assignment is due. The Late Assignment Policy applies to this assignment. Total points possible: 100 pointsPreparing the assignment 1) Follow these guidelines when completing this assignment. Speak with your faculty member if you have questions. a. Select a scholarly nursing or research article, published within the last five years, related to mental health nursing. The content of the article must relate to evidence-based practice. · You may need to evaluate several articles to find one that is appropriate. b. Ensure that no other member of your clinical group chooses the same article, then submit your choice for faculty approval. c. The submitted assignment should be 2-3 pages in length, excluding the title and reference pages. 2) Include the following sections (detailed criteria listed below and in the Grading Rubric must match exactly). a. Introduction (10 points/10%) · Establishes purpose of the paper · Captures attention of the reader b. Article Summary (30 points/30%) · Statistics to support significance of the topic to mental health care · Key points of the article · Key evidence presented · Examples of how the evidence can be incorporated into your nursing practice c. Article Critique (30 points/30%) · Present strengths of the article · Present weaknesses of the article · Discuss if you would/would not recommend this article to a colleague d. Conclusion (15 points/15%) · Provides analysis or synthesis of information within the body of the text · Supported by ides presented in the body of the paper
- 3. · Is clearly written e. Article Selection and Approval (5 points/5%) · Current (published in last 5 years) · Relevant to mental health care · Not used by another student within the clinical group · Submitted and approved as directed by instructor f. APA format and Writing Mechanics (10 points/10%) NR326 Mental Health Nursing RUA: Scholarly Article Review Guidelines NR326 Mental Health Nursing RUA: Scholarly Article Review Guidelines NR326_RUA_Scholarly_Article_Review_V4b_FINAL_MAY21 1 · Correct use of standard English grammar and sentence structure · No spelling or typographical errors · Document includes title and reference pages · Citations in the text and reference page For writing assistance (APA, formatting, or grammar) visit the APA Citation and Writing page in the online library. Please note that your instructor may provide you with additional assessments in any form to determine that you fully understand the concepts learned in the review module. Grading Rubric Criteria are met when the student’s application of knowledge demonstrates achievement of the outcomes for this assignment. Assignment Section and Required Criteria (Points possible/% of total points available)
- 4. Highest Level of Performance High Level of Performance Satisfactory Level of Performance Unsatisfactory Level of Performance Section not present in paper Introduction (10 points/10%) 10 points 8 points 0 points Required criteria 1. Establishes purpose of the paper 2. Captures attention of the reader Includes 2 requirements for section. Includes 1 requirement for section. No requirements for this section presented. Article Summary (30 points/30%) 30 points 25 points 24 points 11 points 0 points Required criteria 1. Statistics to support significance of the topic to mental health care 2. Key points of the article 3. Key evidence presented 4. Examples of how the evidence can be incorporated into your nursing practice Includes 4 requirements for section. Includes 3 requirements for section. Includes 2 requirements for section. Includes 1 requirement for section. No requirements for this section presented. Article Critique
- 5. (30 points/30%) 30 points 25 points 11 points 0 points Required criteria 1. Present strengths of the article 2. Present weaknesses of the article 3. Discuss if you would/would not recommend this article to a colleague Includes 3 requirements for section. Includes 2 requirements for section. Includes 1 requirement for section. No requirements for this section presented. Conclusion (15 points/15%) 15 points 11 points 6 points 0 points 1. Provides analysis or synthesis of information within the body of the text 2. Supported by ides presented in the body of the paper 3. Is clearly written Includes 3 requirements for section. Includes 2 requirements for section. Includes 1 requirement for section. No requirements for this section presented. Article Selection and Approval (5 points/5%) 5 points 4 points 3 points 2 points 0 points 1. Current (published in last 5 years)
- 6. 2. Relevant to mental health care Includes 4 Includes 3 Includes 2 Includes 1 No requirements for ( NR326 Mental Health Nursing RUA: Scholarly Article Review Guidelines ) NR326_RUA_Scholarly_Article_Review_V4b_FINAL_MAY21 1 3. Not used by another student within the clinical group 4. Submitted and approved as directed by instructor requirements for section. requirements for section. requirements for section. requirement for section. this section presented. APA Format and Writing Mechanics (10 points/10%)
- 7. 10 points 8 points 7 points 4 points 0 points 1. Correct use of standard English grammar and sentence structure 2. No spelling or typographical errors 3. Document includes title and reference pages 4. Citations in the text and reference page Includes 4 requirements for section. Includes 3 requirements for section. Includes 2 requirements for section. Includes 1 requirement for section. No requirements for this section presented. Total Points Possible = 100 points 119© NAPICU 2016 Journal of Psychiatric Intensive Care Journal of Psychiatric Intensive Care, 12 (2): 119–127 doi:10.20299/jpi.2016.009 Received 15 July 2015 | Accepted 28 January 2016 © NAPICU 2016 REVIEW ARTICLE The use of a token economy for behaviour and symptom management
- 8. in adult psychiatric inpatients: a critical review of the literature Krista Glowacki, Grace Warner, Cathy White School of Occupational Therapy, Dalhousie University, Canada Correspondence to: Krista Glowacki, School of Occupational Therapy, Forrest Building, PO Box 15000 Halifax, Nova Scotia, B3H 4R2, Canada; [email protected] Background: A token economy is a behavioural modification and reward based intervention in which tokens are given for predefined terms. This review aims to answer the question: What is the effectiveness of the use of a token economy for the reduction of negative behaviours and symptoms in adult psychiatric inpatients? Method: A systematic review of studies using a token economy for adults with mental illness, within an inpatient setting was undertaken for the period 1999–2013. References cited in relevant literature were also examined. Results: The Oxford CEBM Levels of evidence was used to determine quality. Grade A and B recommended studies were included in the review. A total of seven studies were included in the analysis. All of the studies showed the effectiveness of a token economy for reducing negative
- 9. behaviours and symptoms in the short-term. Conclusions: The use of a token economy, on the basis of reward and encouragement, should be considered within inpatient psychiatric settings. The literature shows the effectiveness on behavioural changes in reduction of violence and aggression. The literature on negative symptom reduction is scarce and cannot be generalised. There is no evidence to support the transfer outside of an inpatient/secure setting. Key words: token economy; psychiatric inpatient; symptom manage- ment; behaviour management Financial support: This research received no specific grant from any funding agency, commercial or not-for-profit sectors. Declaration of interest: None. 120 © NAPICU 2016 GLOWACKI ET AL. Introduction With the shift toward community-based mental health care, inpatient psychiatry units are seeing an increase in acuity of the patients who come through their doors (Bow - ers, 2005). Common reasons for admission include danger to self or others, severe mental disorder such as psychosis, and extreme behaviours such as agitation, mania,
- 10. unpredictability, confusion, disorientation, emotional lability, distress/tears, acting out and delusions (Bowers, 2005). Patients may exhibit negative symptoms such as slow and superficial responses, social withdrawal, and lack of energy (Hopko et al. 2003; Gholipour et al. 2012), or negative behaviours, including agitation and aggres- sion particularly toward staff members (Lepage et al. 2003; Park & Lee, 2012). Thus, the creation of a safe and secure environment becomes paramount. As Bowers (2005) discussed, ongoing risk assessment and monitoring and observation of the patients are routine aspects of the care, which may lead to the need to employ skills in negotiation, persuasion, coaxing, distraction and de-escalation. When patients do escalate, disrupting the milieu and placing themselves and/or others at risk, be- haviour management strategies such as exerting physical control, restraints and coercive use of medications may be employed to mediate the behaviour. One approach to behaviour modification that has received limited recent attention in the literature is the use of a token economy. Background A token economy, developed for use within inpatient psychiatry settings, is a behaviour modification interven- tion that can be used to shape behaviours including acquir- ing new skills, reducing undesired behaviours, increasing treatment compliance, and improving overall manage- ment of patients on psychiatry units (LePage et al. 2003; McMonagle & Sultana, 2000). This intervention is based on operant conditioning. Patients can earn ‘tokens’ which have no innate value, and can exchange them for some- thing that does have value to them, such as goods, services or privileges in the facility when they exhibit a desired behaviour (Seegert, 2003; McMonagle & Sultana, 2000).
- 11. The first principle of the token economy is the law of cause and effect based on the idea that reinforcement is the most effective means in changing behaviour. The second princi - ple is the law of contiguity association, in that two events will be associated with one another if they happen together (Dickerson et al. 2005; McMonagle & Sultana, 2000). In the original economy, both reward and punishment tech- niques could be implemented (Kreyenbuhl et al. 2010). Punishment is now viewed as inappropriate within a healthcare setting, causing the decline of this intervention. Punishment is considered a negative consequence, includ- ing the removal of tokens. There are common mis- conceptions about all token economies, including the belief that the intervention is abusive, it does not foster individual treatment, and does not generalise. These mis- conceptions prevail among health care practitioners and further contribute to its lack of use (LePage et al. 2003). A token economy can facilitate improvement in behav- iour and function. It is an economically friendly intervention, and can be beneficial in facilities with lim- ited resources (LePage, 1999; Seegert, 2003; Coelho et al. 2008; Comaty et al. 2001; McMonagle & Sultana, 2000; Kreyenbuhl et al. 2010). It is relatively simple in its overall conceptualisation for those involved, and is beneficial for reducing challenging or disruptive behaviours (LePage, 1999; Coelho et al. 2008). Token economies can be used to increase functioning and to foster recovery, a key focus of today’s mental health care (Hassell, 2009). A systematic review of the use of token economies was published in 2000, analysing literature up to 1999 (McMonagle & Sultana, 2000). McMonagle & Sultana (2000) concluded by recommending the token economy as a cost-effective alternative to psychosocial interven-
- 12. tions in institutions with financial struggles. The article also recommends further in-depth research in a controlled setting using randomised trials to further explore effec- tiveness. This systematic review of the literature examines current research (1999–2013) on the use of a current token economy in adult inpatient psychiatric settings. The ques- tion guiding the review is: What is the effectiveness of the use of a token economy for the reduction of negative behaviours and symptoms in adult psychiatric inpatients? Method Inclusion criteria Types of studies. Peer reviewed articles including: randomised controlled trials, prospective cohort studies, retrospective cohort studies and pre–post design. Types of participants. Adults ages 18 and older admitted to a psychiatric facility as an inpatient in a forensic, acute, or rehabilitation unit, with a mental health disorder as identified in the Diagnostic Statistical Manual of Mental Disorder, 5th Edition (DSMV). Types of interventions. Intervention included a token economy in which tokens or vouchers are given as rewards for behaviour specified prior to entering the programme/ economy. Rewards may be given for positive behaviour or abstinence of negative behaviour. The goal is to achieve behavioural change by means of use of non-monetary and non-consumable tokens, which can be exchanged for a variety of goods, privileges or services in the facility. 121© NAPICU 2016
- 13. A TOKEN ECONOMY Types of outcome measures. To determine if the therapy is effective, there must be a reduction in one of the two identified outcomes after the implementation of the inter - vention. The identified outcomes are negative behaviours or negative symptoms. Negative behaviours include: vio- lence, aggression, and drug abuse. Negative symptoms include: flat affect, lack of pleasure in life, lack of partici - pation, lack of ability to begin and sustain activities, and lack of socialisation and interaction with others. Out- comes can be measured by observation data, frequency data, incident reports, patient charts, group participation numbers/percentages and number of positive urine sam- ples. Statistical information was extracted from each study inclusive of average test scores and standard deviation, statistical significance and effect size in changes or differ - ences. Search strategy Electronic searches were undertaken, limiting results to the English language and publication in the period 1999– 2013 (due to the McMonagle & Sultana (2000) review including research prior to 1999). The databases CINAHL, EMBASE, OTseeker, PubMed, PsycInfo and Google Scholar were used. The search terms used in CINAHL (EBSCOhost) were: (1) “token economy” OR (tokens OR vouchers) and psychiatric OR (mental* N2 (health OR ill* OR disorder*)) and inpatient* OR hospital* OR ward* OR unit OR patient* OR forensic*; (2) “token economy” OR tokens OR vouchers and psychiatric OR mental* NEAR/2 (health OR ill* OR disorder*) and inpatient* OR hospital* OR ward* OR unit OR patient* OR forensic* and
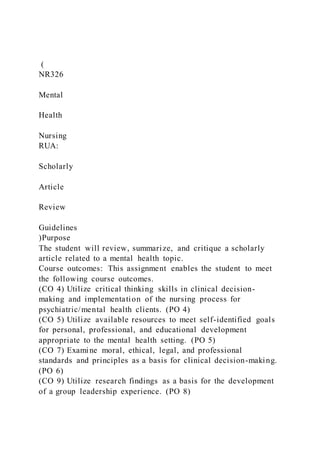
- 14. behavi* OR violen* OR aggressi* OR negative; (3) “To- ken economy” and adult; (4) “Token economy” and psychiatric OR (mental* N2 (health OR ill* OR disor- der*)); (5) Voucher-based and mental health. Other similar search terms were used in the other databases. An exami- nation of references cited in relevant literature was also undertaken. Exclusion criteria Research done before 1999, participants under the age of 18, outpatient settings, and diagnoses not in the DSMV were excluded. Specific study types not included were: systematic reviews, open forum blogs, hospital unit re- views and descriptive articles of intervention without a measureable outcome (see Fig. 1). Data extraction & quality review Articles were identified through electronic searches and abstracts were reviewed. Those that did not meet the inclusion criteria were then excluded. Of the abstract reviews, 20 articles were identified and the full manuscripts Identified through searching database: n = 342 Identified through
- 15. examination of references: n = 3 Excluded after abstract review: n = 325 Full-text articles assessed for eligibility: n = 20 Included after manuscript review: n = 7 Excluded after manuscript review: n = 13 Reasons: Population not inpatients: n = 4 Study design: n = 7 Outcome measured not negative behaviour change: n = 1 Full text not accessible: n = 1 Fig. 1. Articles included and excluded.
- 16. 122 © NAPICU 2016 GLOWACKI ET AL. of the papers were read and assessed for quality and eligibility. The Oxford Centre for Evidence-Based Medi- cine Levels of Evidence was used to determine quality, and only grade A and B studies were included in the review (OCEBM, 2009). Grade A studies are considered the highest quality and grade B studies are the second highest quality. After the full manuscript reviews, 13 were ex- cluded, leaving 7 studies to be included in the systematic review. Figure 1 indicates reasons why studies were ex- cluded. Results Data were extracted from seven studies and compared to determine the effectiveness of a token economy (Table 1). Each study included a rewards and incentive based token economy for adults within an inpatient psychiatry setting. Of the seven studies, three were randomised controlled trials, one was a prospective cohort, two were pre–post designs and one was a retrospective cohort. All of these studies were categorised using the OCEBM (2009) to determine study quality. The studies classified as grade A of the OCEBM (2009) were the three randomised controlled trials (Hopko et al. 2003; Gholipour et al. 2012; Park & Lee, 2012). Randomisation methods were difficult to assess as entire inpatient units were used. Two of the studies looked only at male units and were done outside of North America
- 17. (Gholipour et al. 2012; Park & Lee, 2012), and in one, all males on the unit were diagnosed with schizophrenia (Gholipour et al. 2012). Thus, cultural and gender differ- ences should be considered and the results be used with caution to generalise to North American culture and prac- tice, and to mixed units. Two of the studies had small sample sizes (Hopko et al. 2003; Gholipour et al. 2012). The next grade of studies, level B of the OCEBM (2009), were pre–post designs and prospective cohorts (LePage, 1999; Comaty et al. 2001; LePage et al. 2003). Two of the studies only analysed one unit of a hospital, limiting the generalisation, and there was no control group as all patients in the unit participated in the token economy (LePage, 1999; LePage et al. 2003). Lastly, a retrospective study, also grade B of the OCEBM (2009) was used (Hassell, 2009). This included an analysis of medical records and no power analysis was used to determine if sample size was adequate. In the same study various healthcare profession- als implemented the token economy and no information was given on inter-relater reliability or training. It should also be noted that in all of the studies the intervention was combined with individualised pharmacological treatment. The effect of interventions on outcomes The effectiveness of the intervention being analysed will be reported as a narrative synthesis. This part will be separated into two sections. The first will describe the effectiveness of the intervention on negative behaviours, and the second will describe the effectiveness on negative symptoms. Behaviour. Behavioural change was an outcome meas- ured in five of the studies (LePage, 1999; Comaty et al. 2001; LePage et al. 2003; Hassell, 2009; Park & Lee,
- 18. 2012). These studies included violent and aggressive be- haviour in a physical or non-physical manner that could harm or threaten other individuals or themselves, mainly reported as ‘incidents’. All of the studies’ findings support the efficacy of the token economy for reducing negative behaviours and unit incidents related to these behaviours on inpatient psychiatric units. It should be noted that one study did not have a control, so improvements in behav- iour and function cannot be attributed to the token economy alone (Hassell, 2009). Further, one study and its results provides data to support the positive long-term impact a token economy can have on the safety and function of an acute care unit (LePage et al. 2003). Negative symptoms. The effect of the intervention on negative symptoms was examined in two studies (Hopko et al. 2003; Gholipour et al. 2012). The findings from both studies support the efficacy of the token economy for negative symptom reduction in an inpatient setting. How- ever, the study by Hopko et al. (2003) only included inpatients diagnosed with depression, and the study by Gholipour et al. (2012) only included males with schizo- phrenia. See Table 1 for a summary of the outcomes, results, and the statistical data from each study. Discussion This systematic review supports the efficacy of a token economy for reducing negative behaviours in adults with mental health illness in an inpatient psychiatry setting. All five of the studies analysing behavioural change showed statistical significance in the reduction of negative behav- iours. While the literature reviewed on the efficacy of the economy for reducing negative symptoms supported the use of the intervention, the number of studies was limited, providing insufficient evidence to support its use. Further,
- 19. the symptom reduction studies only targeted one diagno- sis, not representative of most psychiatric inpatient units. The research on symptom reduction alone is scarce, and this outcome measure needs to be explored further. All of the studies looked at the effects within an inpatient setting, and the regime of hospital units is important to con- sider. This includes structure, schedules, expectations and staff. None of the studies were able to look at the direct effects on behaviour or symptoms outside of an inpatient setting, so this is an important caution if considering use of 123© NAPICU 2016 A TOKEN ECONOMY Ta b le 1 . D a ta e xt ra ct e d
- 115. u e d 124 © NAPICU 2016 GLOWACKI ET AL. Ta b le 1 . C o n tin u e d C o m a ty e t
- 214. 125© NAPICU 2016 A TOKEN ECONOMY R e s u lt s T h e n o n -c o m p le te rs T h e t o ke
- 309. vi n g ; B A T D : b e h a vi o u ra l a ct iv a tio n tr e a tm e
- 310. n t f o r d e p re ss io n ; B D : b e h a vi o u ra l d is o rd e r;
- 311. D D : d u a l d ia g n o si s M D D : m a jo r d e p re ss iv e d
- 315. : s h o rt -t e rm t o ke n e co n o m y 126 © NAPICU 2016 GLOWACKI ET AL. this intervention in a community setting. Comaty et al. (2001) looked at a three-year follow-up after discharge and re-hospitalisation rates, but the data was not conclu- sive; thus the authors were unable to say whether a longer stay in the community was a result of the token economy itself.
- 316. Using a token economy may be a means of reducing violence and aggression on inpatient units. Improved safety in inpatient units for staff and patients may allow healthcare practitioners to focus their attention on treatment and rehabilitation, and less on control of the unit. Behavioural focus could be less on the reduction of negative behav- iours, and more on the promotion of positive behaviour for rehabilitation and recovery. Further, reduction in negative symptoms may also increase participation and collabora- tion of patients toward rehabilitation goals. Healthcare practitioners should be cautious in using a token economy. The token economies used in the studies of this paper varied in rewards, desired behaviour and structure. In saying this, the general concept of each economy was the same, earning tokens for positive behav- iour towards rehabilitation that can be accumulated for pre-determined rewards. The economy has potential for abuse if implemented improperly, so programmes should limit punishment and response costs for behaviour. This is inclusive of the removal of tokens for negative behaviour. Based on a recovery-oriented, patient-centred approach, the following recommendations derive from the literature: 1. Participants in the programme should be given the option of enrolling at admission, and participation should stay voluntary throughout (LePage et al. 2003; Park & Lee, 2012). 2. Staff and patients involved in the token economy should collaborate to pre-determine rewards (Chiou et al. 2006; Dunn et al. 2008; Park & Lee, 2012). Rewards should also be individualised (Park & Lee, 2012). 3. Thorough staff training should be done to ensure
- 317. consistency in programme implementation (LePage 1999; LePage et al. 2003). 4. The token/voucher should be given immediately, thereby verifying positive behaviour (Chiou, et al. 2006; LePage et al. 2003). 5. The economy should be used in congruence with individualised treatment programmes (LePage, 1999; Gholipour et al. 2012; Park & Lee, 2012). It is important to identify the limitations to this literature review. A small number of studies were analysed, as there are limited recent research studies on this interven- tion. The quality is also limited by the fact that only three studies were randomised controlled trials. Further, this was a brief review of the literature available. The research was only analysed by one person, and only English studies were used. Areas for future research have been identified from this review. The first is using a date after hospital discharge to focus on psychosocial outcomes of participants and their functioning in society outside of an institutional environ- ment. Usually hospitalisation is temporary, and it is important to find a transferable intervention for commu- nity care and living. Further, multiple units in one hospital, or comparison of multiple hospital studies could be done with comparison of control and experimental groups. Research should also be done on symptom reduction for a wider range of diagnoses within a hospital or inpatient unit. Research could also be done on the comparison of different types of rewards within the economies. Conclusions
- 318. The findings of this literature review support the efficacy of a token economy for reducing negative behaviours in an inpatient psychiatric setting. This intervention should be considered by healthcare professionals working in an inpatient setting for reduction of negative behaviours, or increased safety of the units. When implementing a token economy, the recommendations made on adapting the economy based on a recovery-oriented patient-centred practice should also be considered. Few studies were done on the efficacy of the economy for reducing negative symptoms, but all that were done determined that the token economy was effective in symptom reduction. The use of a token economy for symptom reduction should be used with caution until further research is done on the topic. Since the overall number of research studies was lim- ited, the findings identify the need for further research on this intervention and its effects on reducing negative be- haviours and symptoms. While more research is needed, the current findings should encourage healthcare practi- tioners to consider the use of a rewards-based token economy as a treatment intervention in an inpatient psy- chiatry setting. Acknowledgements School of Occupational Therapy at Dalhousie University. The Waterford Hospital in St. John’s Newfoundland, where the research first started based on a clinical need. References Bowers, L. (2005) Reasons for admission and their implications for the nature of acute inpatient psychiatric nursing. Journal of
- 319. Psychiatric & Mental Health Nursing, 12(2): 231–236. doi: 10.1111/j.1365-2850.2004.00825.x Chiou, J., Chou, M., Hsu, M. and Lin., M. (2006) Significant experiences of token therapy from the perspective of psychotic patients. Journal of Nursing Research, 14(4): 315–322. http://www.ingentaconnect.com/content/external- references?article=1351-0126()12:2L.231[aid=10836575] http://www.ingentaconnect.com/content/external- references?article=1351-0126()12:2L.231[aid=10836575] http://dx.doi.org/10.1111/j.1365-2850.2004.00825.x http://dx.doi.org/10.1111/j.1365-2850.2004.00825.x 127© NAPICU 2016 A TOKEN ECONOMY Coelho, C.M., Palha, A.P., Gonçalves, D.C. and Pachana, N. (2008) Rehabilitation programs for elderly women inpatients with schizo- phrenia. Journal of Women & Aging, 20(3/4): 283–295. Comaty, J.E., Stasio, M. and Advokat, C. (2001) Analysis of out- come variables of a token economy system in a state psychiatric hospital: a program evaluation. Research in Developmental Disabilities, 22(3): 233–253. Dickerson, F.B., Tenhula, W.N., and Green-Paden, L.D. (2005) The token economy for schizophrenia: review of the literature and recommendations for future research. Schizophrenia Research, 75(2–3): 405–416.
- 320. Dunn, K., Sigmon, S., Thomas, C., Heil, S. and Higgins, S. (2008) Voucher-based contingent reinforcement of smoking abstinence among methadone-maintained patients: a pilot study. Journal of Applied Behavior Analysis, 41: 527–538. Gholipour, A.A., Abolghasemi, S.H., Gholinia, K.K and Taheri, S. (2012) Token reinforcement therapeutic approach is more effec- tive than exercise for controlling negative symptoms of schizophrenic patients: a randomized controlled trial. Interna- tional Journal of Preventive Medicine, 3(7): 466–470. Hassell, J.T. (2009) An evolution of the points incentive program: a token economy program for veterans hospitalized on an inpa- tient treatment unit. PhD Thesis, Alliant International University, Los Angeles. Dissertation Abstracts International, 71. Hopko, D.R., Lejuez, C.W., LePage, J.P., Hopko, S.D. and McNeil, D.W. (2003) A brief behavioral activation treatment for depres - sion: a randomized pilot trial within an inpatient psychiatric hospital. Behavior Modification, 27(4): 458–469. Kreyenbuhl, J., Buchanan, R.W., Dickerson, F.B. and Dixon, L.B. (2010) The schizophrenia Patient Outcomes Research Team (PORT): updated treatment recommendations 2009. Schizo- phrenia Bulletin, 36(1): 94–103. LePage, J. (1999) The impact of a token economy on injuries and
- 321. negative events on an acute psychiatric unit. Psychiatric Serv- ices, 50(7): 941–944. Lepage, J., Delben, K., Pollard, S., McGhee, M., VanHorn, L., Murphy, J., Lewis, P., Aboraya, A. and Mogge, N. (2003) Reduc- ing assaults on an acute psychiatric unit using a token economy: a 2 year follow-up. Behavioral Interventions, 18: 179–190. McMonagle, T. and Sultana, A. (2000) Token economy for schizo- phrenia. Cochrane Database of Systematic Reviews, 2000(3): CD001473. OCEBM Levels of Evidence Working Group (2009) The Oxford Levels of Evidence. Oxford Centre for Evidence-Based Medi- cine, Levels of Evidence Working Group. Park, J.S. and Lee, K. (2012) Modification of severe violent and aggressive behavior among psychiatric inpatients through the use of a short-term token economy. Journal of Korean Academy of Nursing, 42(7): 1062–1069. Seegert, C.R. (2003) Token economies and incentive programs: behavioral improvement in mental health inmates housed in state prisons. The Behavior Therapist, 26(1): 208, 210–211. http://www.ingentaconnect.com/content/external- references?article=1075-2730()50:7L.941[aid=10836580] http://www.ingentaconnect.com/content/external- references?article=1075-2730()50:7L.941[aid=10836580] Reproduced with permission of copyright owner. Further reproduction prohibited without permission.