This study evaluated the inappropriate usage of medications that increase fall risk in older patients using an interdisciplinary communication tool. Nurses assessed fall risk using the Morse Fall Scale and identified high-risk medications. Pharmacists identified potential therapeutic interventions. Physicians assessed patient gait. Of the patients analyzed, 55% met criteria for potential fall risk and 69% of these patients had high Morse Fall Scale scores. A total of 50 high-risk medications and 16 potential interventions were identified. Most healthcare professionals believed increased interdisciplinary communication about falls is needed. The communication tool may help flag high-risk patients and identify interventions to reduce fall risk.
Dr Jeremy Veillard: High Use in the Health Sector in Canada, 30 June 2014
Poster Presentation
1. Results
Methods
• Survey sent to nurses, pharmacists, and physicians to assess their
personal beliefs about the value of interdisciplinary communica9on
with regards to fall risk
• Interdisciplinary form created to iden9fy pa9ents at risk
• Form divided into three sec9ons to be filled out by nurses,
pharmacists, and physicians:
• Nurses: calculated pa9ent’s fall risk using the Morse Fall
Scale and listed high risk medica9ons
• Pharmacists: iden9fied therapeu9c interven9ons
• Physicians: assessed pa9ent gait
Background
• Accidental falls occur at a rate of 30-40% per year in community
dwelling adults over the age of 651
• Risk factors associated with falls include:2
• History of postural instability or history of falls
• Use of ≥ 3 medica9ons implicated in causing falls
• Side effects which predispose geriatric pa9ents to falls include:3
• Orthosta3c hypotension: an9hypertensives
(e.g. diure9cs)
• Seda3on: opioids and psychotropic drugs
• Confusion: an9cholinergics
Iden9fying Inappropriate Medica9on Usage in Geriatric Fall Risk Pa9ents
via an Interdisciplinary Communica9on Tool
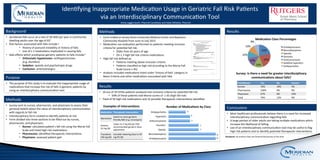
Results
• 16 out of 29 (55%) pa9ents analyzed met inclusion criteria for poten9al fall risk
• 69% of these pa9ents had Morse scores of ≥ 45 (high fall risk)
• Total of 50 high risk medica9ons and 16 possible therapeu9c interven9ons iden9fied
11
11
7
7
5
5
4
An9depressants
Benzodiazepines
Opiods
Diure9cs
An9convulsants
Hypno9cs
An9psycho9cs
Number of Medica3ons by Class
Purpose
• The purpose of this study is to evaluate the inappropriate usage of
medica9ons that increase the risk of falls in geriatric pa9ents by
using an interdisciplinary communica9on tool.
Prac33oner Yes No Unsure
Nurses 76% 19% 5%
Pharmacists 100% 0% 0%
Physicians 67% 0% 33%
Total 79% 12% 9%
Methods
• Form trialed at Jersey Shore University Medical Center and Bayshore
Community Hospital from June to July 2015
• Medica9on use evalua9on performed on pa9ents mee9ng inclusion
criteria for poten9al fall risk:
• Older than 65 years of age
• On ≥ 3 high fall risk criteria medica9ons
• High fall risk defined as:
• Pa9ents mee9ng above inclusion criteria
• Pa9ents classified as high risk according to the Morse Fall
Scale (score ≥ 45)
• Analysis included medica9ons listed under ‘history of falls’ category in
Beers Criteria and other medica9ons associated with falls
Conclusions
• Most healthcare professionals believe there is a need for increased
interdisciplinary communica9on regarding falls
• A large por9on of older adults are taking mul9ple medica9ons which
increase the likelihood of falling
• Use of an interdisciplinary communica9on tool may be useful to flag
high risk pa9ents and to iden9fy poten9al therapeu9c interven9ons
22%
22%
14%
14%
10%
10%
8%
Medica3on Class Percentages
An9depressants
Benzodiazepines
Opioids
Diure9cs
An9convulsants
Seda9ve hypno9cs
An9psycho9cs
Smita Jaggernauth, PharmD Candidate and Ka9e Militello, PharmD
Survey: Is there a need for greater interdisciplinary
communica3ons about falls?
Medica3on Therapeu3c Interven3on
Alprazolam
Switch to more geriatric
friendly BZD (e.g. lorazepam)
Ambien
10 mg QD
Lower to 5 mg QD per FDA
recommended geriatric dose
adjustment
Trazodone
100 mg QD
Consider lowering dose to 50
mg PO QD
Examples of Interven3ons
Disclosure: No authors have any financial disclosures at this 9me