
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Spina bifida
Similar to Spina bifida (20)
Recently uploaded
Recently uploaded (20)
Spina bifida
- 1. Spina bifida Presented by Shiksha verma MPT(Neuro)
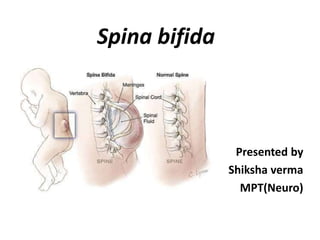
- 2. Definition • (Latin “Split Spine”) is a developmental congenital disorder caused by incomplete closing of the embryonic neural tube. • Some vertebrae overlying the spinal cord are not fully formed and remain unfused and open. • It is usually occur in lumbar or sacral region.
- 3. Incidence • It is the one of the most common birth defects, with an average worldwide incidence of one to two cases per 1000 births, but certain populations have a significantly greater risk. • Myelomeningocele is the most significant and common form and this leads to disability in most affected individuals. • This condition is more likely to appear in females; the cause for this is unknown.
- 4. Types of spina bifida
- 5. Transverse section of vertebrae
- 6. Types 1. Spina bifida occulta – – Occulta is a latin word which means “hidden”. This is the mildest form of the spina bifida. – In occulta, the outer part of some of vertebrae is not completely closed. – The splits in the vertebrae are so small that the spinal cord does not protrude. – The skin at the site of lesion may be normal or it may have some hair growing from it.
- 8. 2. Meningocele – The bony vertebrae is open, part of meninges is protruding out of the spinal canal. – Since the spinal cord is not protruding, there is often normal function.
- 9. 3. Myelomeningocele – The bony vertebrae is open, part of meninges and part or all the spinal cord is protruding out of the spinal canal. – Since the spinal cord is protruding, it is often not fully developed. – Involving nerve roots are often not developed resulting in weakness, pain and/or paralysis.
- 10. – Arnold Chiari malformation II is often is associated with myelomeningocele and occurs when the cerebellum is forced downward. – This can result in life-threatening situations because the build-up of cerebrospinal fluid can cause pressure on the brain.
- 12. Causes of spina bifida • The exact cause of spina bifida is unknown. • All the research to date has indicated both genetic and environmental influence. • The developmental process that results in spina bifida is well studied.
- 13. Pathogenesis Neural tube defect: The neural plaque that develops between the 2nd and 4th weeks in the embryologic stage is closed by curving from two edges and forms the neural tube. While the brain develops from the cranial part of the neural tube, the spinal cord develops from the caudal part. Problem that occur during the closure of the caudal part of the neural tube in this stage cause spina bifida and other spinal cord disorders. The risk of an adult with MMC having the a child with neural tube defect is 5%. Women with low level of RBCs and folate level during early pregnancy have up to a 6 times greater risk of having a child with a neural tube defect.
- 15. Clinical manifestation 1. Spina bifida occulta: spina bifida occulta are asymptomatic, the only features seen are: – Dimple in the skin or growth of hair over malformed vertebrae. – As the child grows, he may develop foot weakness or disturbances of bladder and bowel sphincter. 2. Meningocele: – External cystic defect – Weakness of leg or lack of sphincter control
- 16. 3. Myelomeningocele Primary clinical picture: A. Abnormal nerve conduction, resulting in: – Somatosensory losses – Motor paralysis, including loss of bowel and bladder control (all are below the level of lesion) – Changes in the muscle tone B. An enlarged head caused by: – Hydrocephalus – Arnold chairi malformation II C. Bowel and bladder symptoms
- 17. D. Musculoskeletal deformities – scoliosis – clubfoot E. Joint and extremity problems – joint contractures – hip subluxation – Diminished growth of non weight bearing limb F. Abnormal or damaged nerve tissue which can leads to loss of extroceptive and proprioceptive sensation Secondary features: – Skin breakdown – Obesity – Latex allergy – Osteoporosis.
- 18. Surgical treatment There is no cure for nerve damage caused by spina bifida. Surgery for spina bifida involves a variety of neurological, orthopaedic and urologic procedures. This my includes- – Closure if the defect over the spinal cord. – Spinal deformity reconstruction. – Lower-extremity deformity correction. Medical treatment- – Antibiotics are essential in preventing infection of CNS and UTI.
- 19. Physiotherapy Assessment Subjective - • Name • Age/gender • Weight • Height • Date of admission • Address • Chief complaints/ parent concern • Past medical history • Present medical history • Social and family history
- 20. Physiotherapy assessment conti.. Objective - • MMT • ROM • Sensory testing • Reflex testing • Developmental/ functional evaluations cognitive evaluations
- 21. Physiotherapy Management The therapy programs should be designed to parallel the normal achievement of gross motor milestones • Stage 1: before surgical closure of sac: – Rom – Positioning – Auditory and visual stimulation • Stage 2: after surgery during hospitalization – Positioning in prone lying and side lying – ROM taught to parents – Provide toys of various colours, textures and shapes – Therapeutic handling to encourage good head and trunk control
- 22. • Stage 3: pre ambulatory stage – Work on sitting and equilibrium reactions – Eye-hand coordination activities – Early weight bearing on lower limbs – Weight shifting in standing frame – Continue home program • Stage 4: toddler through preschool – Choose appropriate orthotic devices – Gait training – Strengthening exercises – Development in cognitive and psychological areas – Continue home programme
- 23. • Stage 5 : primary school through adolescence – Replace orthotic device as necessary – Wheel chair prescription as necessary – Teach locomotion activities – Strengthening exercise of trunk and extremities – Teach skin care – Teach-self care activities like dressing, feeding, hygiene, bowel and bladder care.
- 24. Thank you