
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Mucoceles of the Paranasal Sinuses
Similar to Mucoceles of the Paranasal Sinuses (20)
More from Dr. Shilpa M J
Recently uploaded
Recently uploaded (20)
Mucoceles of the Paranasal Sinuses
- 1. DR.SHILPA M J MUCOCELES OF THE PARANASAL SINUSES
- 2. A Mucocele is an epithelium-lined mucus-filled sac within one of the paranasal sinuses with expansion of the sinus cavity and remodelling of the sinus walls. Forms – secondary to obstruction of the outflow tract and an inflammatory process within the sinus. Lining epithelium - pseudostratified or low-columnar epithelium. Bony erosion - mucocele’s epithelium is often fused with dura or orbital periosteum. DEFINITION
- 3. Frontal > ethmoid > maxillary > sphenoid sinuses Frontal sinus mucoceles - more common - complex and narrow drainage pathway - easily obstructed. Mucoceles - can form in aerated structure – concha bullosa of the middle or superior turbinate. Obstruction of the nasolacrimal duct - lacrimal sac mucocele / dacryocele. SITE OF DEVELOPMENT
- 4. Following Sinus surgery - for chronic sinusitis and nasal polyposis. frontal and sphenoid mucoceles developing earlier than maxillary sinus mucoceles. Surgery of the frontal recess - circumferential injury to the frontal sinus outflow tract - subsequent stenosis – mucocele. AETIOLOGY
- 5. External fronto-ethmoidectomy/ Lynch-Howarth operation - leading cause - because of loss of lateral bony support of the frontal recess which causes herniation of the periorbital tissue into the frontal sinus outflow tract. Following endoscopic repair of skull-base fractures in children. Any benign or malignant tumour. AETIOLOGY
- 6. Two factors are essential: 1) An obstructed sinus outflow tract 2) An inflammatory process within the sinus Osteolytic cytokine-IL-1 and tumour necrosis factor are present within the epithelial lining of mucoceles. Cytokine may be the responsible for the bony erosion in expanding mucoceles. PATHOGENESIS
- 7. A visible mass - on the forehead, medial canthus or in the gingivobuccal sulcus or cheek. Ophthalmologic symptoms are more common than rhinological and neurological symptoms. The most common ophthalmologic complaints - periorbital swelling, pain and exophthalmos. Displacement of the orbital content - lead to limited ocular mobility, visual disturbance and diplopia. CLINICAL FEATURES
- 9. Optic neuropathy - 18% of patients - due to direct compression of the optic nerve in the posterior ethmoid and sphenoid sinuses. A mucocele within a concha bullosa may present with nasal obstruction and / or secondary sinusitis. Epiphora and a cystic swelling in the medial canthus suggest the presence of a dacryocele. CLINICAL FEATURES
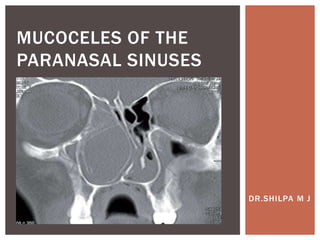
- 11. Computed tomography (CT) - homogeneous, isodense lesion within an expanded sinus with bony remodelling of the sinus walls. Contrast enhancement - pyocele. A bony defect of the lamina papyracea and / or superomedial part of the orbital rim - fronto- ethmoidal mucoceles. The globe - displaced laterally and / or inferiorly - on axial images. RADIOLOGY
- 12. CT SCAN
- 13. The sac - erosion of the posterior table of the frontal sinus and compression of the intracranial contents. Difficult to differentiate maxillary sinus mucoceles from other benign or malignant lesions. Magnetic resonance imaging (MRI) - significant bony erosion of the posterior table of the frontal sinus or the orbital lamina papyracea – delineate the mucocele from adjacent soft tissue e.g. cerebral tissue. MRI can be misleading - variability of mucocele content. RADIOLOGY
- 14. MRI
- 15. 1. Benign or malignant tumours 2. Allergic fungal sinusitis / Other fungal disease 3. Cholesterol granuloma (rare). DIFFERENTIAL DIAGNOSIS
- 16. Widely marsupialize the sac - provide permanent ventilation and sinus drainage and to relieve pressure on vital structure. Cosmetic deformities settle with time - bony remodelling takes place. Fronto-ethmoidal mucoceles Wide marsupialization by endoscopic and/or open technique. Endoscopic surgery with wide marsupialization/nasalization - the first line of treatment - simple mucoceles. SURGICAL MANAGEMENT
- 17. Modified Endoscopic Lothrop Procedure (MELP) - more complex frontal sinus mucoceles Combined approaches - required for laterally located mucoceles - thick bony septation Lynch-Howarth approach - access laterally located frontal sinus mucoceles,to assist with the drilling down of bony septations. SURGICAL MANAGEMENT
- 18. An osteoplastic frontal flap in combination with a MELP – mucocele lying far laterally in the frontal sinus. Transorbital neuroendoscopic surgery (TONES) and the superior eyelid approach – an alternative, less invasive approach. Stenting remains controversial. Stent - loose fitting to prevent circumferential pressure. SURGICAL MANAGEMENT
- 19. Maxillary sinus mucoceles A wide middle meatal antrostomy will usually suffice. A partial medial maxillectomy with preservation of the lacrimal system - to gain access to laterally located mucoceles. The Caldwell-Luc approach - in centres where endoscopic surgery is not an option. SURGICAL MANAGEMENT
- 20. Sphenoid sinus mucoceles A wide sphenoidotomy and intra-nasal marsupialization. No attempt to remove the lateral sphenoid sinus mucosa as bony erosion place the internal carotid artery or optic nerve at risk of injury. Other mucoceles Within a concha bullosa - resection of the lateral aspect of the concha bullosa. Dacryoceles - Endoscopic dacryocystorhinostomy. SURGICAL MANAGEMENT
- 21. Great care - decompressing a large,tense frontal mucocele that displaces the frontal lobe of the brain as sudden expansion of the cranial contents can disrupt the dural vessels and cause a subdural haematoma, or disrupt the dura - cerebrospinal fluid (CSF) leak. Recurrence occur decades later, long-term follow-up. COMPLICATIONS
- 22. THANK YOU