2. Lip cancer is a malignant tumor from the elements of the integumentary epithelium
of the red border of the lips. Cancer is rare on the upper lip. This is due to the
anatomical and physiological characteristics of the lips (insufficient lubrication
with fat) and unequal susceptibility to carcinogenic factors. The danger lies in the
fact that over time, cancer of the mucous membrane of the lip metastasizes to the
bones of the lower jaw. In addition, damaged cells are transported with the lymph
to the lymph nodes, which causes the appearance of new malignant foci.
Depending on the type of tumor growth, papillary and warty, as well as ulcerative
and ulcerative-infiltrative forms of lip cancer are distinguished. In 95% of cases,
keratinizing squamous cell carcinoma develops; in 5% of cases - squamous cell non
-keratinizing cancer of the lip mucosa, characterized by a more malignant course
(infiltrative growth and early metastasis to regional lymph nodes).
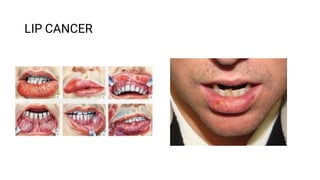
3. Lower lip cancer. Of all parts of the oral cavity, the tumor most often
affects the border of the lower lip. A fissure, ulcer, or wart-like swelling
forms on it. The disease is usually diagnosed in people over the age of 60.
Cancer of the upper lip. Malignant tumors of the upper lip occur less
frequently than the lower lip. However, neoplasms are more aggressive,
cancer of the upper lip spreads quickly, and has a high risk of metastasis.
This is due to the fact that the tumor is located close to the nasal cavity,
where the blood supply system is developed.
In general, in terms of its manifestations, cancer of the upper lip does not
differ from cancer of the lower lip in either symptomatology or methods of
treatment.
4. DIAGNOSTICS
In LISOD, the diagnosis of lip cancer is based on examination data both with the
naked eye and with the use of stomatoscopy (cheiloscopy). These methods make it
possible to detect the nature and depth of the ulcer, to see the infiltration roller around
the ulcerative form of cancer, to determine the state of the surrounding mucous
membrane, on the basis of which the focus of the neoplasm arose. The use of staining
with a 1% aqueous solution of toluidine blue allows you to see areas suspicious of
malignancy (areas of precancerous formations remain unstained, and cancer cells
record a blue color). Palpation of the lip through its entire thickness allows you to
determine the true size of the tumor. If lip cancer is suspected, a cytological
examination of smears-prints from a tumor ulcer is carried out, and punctate of
regional lymph nodes is also examined.
LISOD specialists will definitely clarify the patient's profession and the presence of
contacts with harmful substances.
5. The following examinations are carried out:
examination and digital examination of the lip, buccal-gingival pocket, mucous
membrane of the alveolar processes of the jaws;
palpation of the submandibular region and neck on both sides;
Ultrasound of the lips, neck, abdominal organs (according to indications);
radiography of the lower jaw, orthopantomography (according to indications);
smears-prints for cytological examination (with ulceration) or biopsy of the affected
area;
cytological puncture of the lymph nodes of the neck with their enlargement;
differential diagnosis with tuberculosis and syphilis.
When the diagnosis of lip cancer is confirmed, an x-ray examination of the chest organs,
general clinical and laboratory examinations (ECG, blood tests, urine tests, etc.) are
performed
PET-CT examination is prescribed for:
-evaluating the response to treatment;
-detecting a relapse of the disease during the observation period;
-determining the stage of the disease.
6. TREATMENT
When treating a disease, LISOD specialists take into account many
different factors, from the age of the patient to the type and characteristics
of the spread of the tumor. Regardless of the chosen technique, the effect is
on the lesion focus or tumor and areas of regional metastasis.
With I and II degrees of lip cancer, treatment is carried out by the
following methods:
radiation, which includes external radiation therapy;
surgical, implying radical action and used only when it is impossible to use
radiation treatment.
7. Prophylactic surgery at stages I and II is carried out exclusively in cases
where it is not possible to control the dynamics of the development of the
disease, there are unfavorable forecasts about its spread. At stage III and in
the absence of metastases, treatment is carried out using a combined effect
on the focus of infection and the adjacent areas. With a wide spread of the
disease and in the presence of single metastases in the lymph nodes (stage
IV), combined treatment of lip cancer is performed, followed by surgery,
plastic surgery and surgical correction of the lips. In stage IVC, palliative
chemoradiation therapy is indicated.
Cancer of the lip, which was treated in the early stages, is cured in 97-
100% of cases. At stage III, the disease can be cured in 67-80% of cases.
On IV and repeated relapses - in 55%.
8. SYMPTOMS
Signs of the disease are expressed in lip discaretosis, papillomas, erosive forms of lichen
and cheilitis. For reference: in most cases, discateriasis looks like sores and cracks on
the inside of the lips. In almost all patients, lip cancer is preceded by various
background processes and precancerous conditions of the lip mucosa. Depending on the
resulting pathological changes in the red border, precancerous diseases are distinguished
with a high frequency of malignancy (in 15-30% - obligate) and with a low frequency of
malignancy (in 6-10% - optional), as well as background processes.
Obligate precancer: verrucous precancer, limited hyperkeratosis, Manganotti cheilitis.
Optional precancers: verrucous leukoplakia, keratoacanthoma, cutaneous horn,
keratinized papilloma, erosive-ulcerative and hyperkeratotic forms of lupus
erythematosus and lichen planus erythematosus, postradiation cheilitis.
Background processes: flat leukoplakia, chronic ulcers and lip cracks, atmospheric and
actinic cheilitis.
Treatment of cheilitis, lupus erythematosus and lichen planus is medication with
mandatory microscopic control in the absence of effect. Treatment of other pathological
changes is carried out by cryogenic, surgical, laser exposure and the method of
photodynamic therapy.
9. Cancer of the lip, the symptoms of which are quite vivid and varied, causes many health
problems. To prevent this, the person should pay attention to any bleeding sores. They
are usually crusty and resemble herpes in appearance, but, unlike it, do not heal after a
certain period of time. Some patients have no ulcers. Instead, a small compaction
appears, which grows over time and also becomes covered with a crust. On the red
border of the lower lip, to the side of the midline, a formation or area protruding above
the surface appears. In the center of the formation, an erosion or ulcer is formed with a
granular surface and a roller-like edge. The formation is distinguished by a dense
consistency and gradually increases in size, acquires an irregular shape. The boundaries
of education are unclear. Often, the tumor grows against the background of leukoplakia,
papilloma or cracks, bleeds. Particular attention is paid to the sequence of the
appearance of changes in the lip area. Exophytic lip cancer more often arises from
papilloma or warty form of productive diffuse dyskeratosis. With exophytic growth, a
tumor of dense consistency is often covered with flat scales. Endophytic growth is
characterized by an ulcer with uneven dense edges, often appears against the
background of destructive dyskeratosis, quickly infiltrates the soft tissues of the lip and
is prone to metastasis.
10. Distinguishing neoplasms from common herpes is quite simple. If the appearance of
swelling or sores is accompanied by itching, discomfort when eating, and profuse
salivation, then most likely it is lip cancer. Symptoms of the disease should be a signal
to see a doctor immediately. Remember that lip cancer, the treatment of which was
started on time, is removed from the body without consequences in 90% of cases.
The clinical picture of the disease depends on the stage at which the cancer is and how
far it has spread. A non-healing fissure, which is a precursor to major problems,
develops over time, takes the form of an ulcer and begins to bleed on contact. At the
same time, the patient develops an infiltrate, which also tends to spread. As a result, the
person's lip swells and becomes less mobile. Once again, we note that all signs of lip
cancer are grounds for contacting a specialized medical institution. Otherwise, the
tumor will begin to metastasize to the bone of the lower jaw and the collecting lymph
nodes.
11. RISK FACTORS
Lip cancer is more common in rural people, especially in the southern regions. Quite
often, this tumor occurs in persons by occupation associated with exposure to
atmospheric phenomena: insolation, sudden changes in temperature and humidity,
weathering.
Smoking (especially pipes), alcohol, poor oral hygiene, viral infections play a
significant role. All these factors disrupt the processes of keratinization. Also, the
causes of the onset of the disease can be chronic trauma to the lips with carious teeth
and improperly made prostheses, microburns;
In almost all patients, lip cancer is preceded by various background processes and
precancerous conditions of the lip mucosa.
12. Let's single out the etiological factors causing lip cancer:
long-term exposure to unfavorable meteorological factors (solar radiation, wind, sharp
fluctuations in air temperature, ionizing effects);
exposure to carcinogenic substances;
bad habits: smoking, alcohol, chewing various mixtures (us, betel nut);
injuries of the red border of the lips:
mechanical - carious teeth, sharp edges of teeth, tartar, improperly made dentures, biting
the lip, pressure from a pipe or mouthpiece, cigarettes or cigarettes;
chemical - carcinogens of tobacco, compounds of arsenic, mercury and bismuth,
anthracite, liquid tar, distillation products of oil in persons of the relevant professions;
thermal - burns with hot food, cigarettes;
viral infections (shingles - Herpes zoster);
inflammatory and fungal diseases of the red border of the lips;
diseases of the gastrointestinal tract, liver.
deficiency of beta-carotene, vitamins A, E, C.
13. PREVENTION
Primary. We recommend protecting your face from direct sunlight (wearing a wide-
brimmed hat), quitting smoking cigarettes and pipes, changing working conditions,
observing oral hygiene, and not drinking strong alcoholic beverages. Required annual
dispensary examinations of persons prone to lip dyskeratosis, cheilitis.
Secondary. Have your teeth treated regularly by your dentist. Carry out treatment for
dyskeratosis and cheilitis, including surgery (conservative therapy is usually
ineffective). It is necessary to actively detect and treat precancerous diseases in
agricultural workers, sailors and in enterprises associated with hazardous industries.