Tuberculous infection of the central nervous system (CNS) can occur via hematogenous spread or direct extension from a local infection. It most commonly manifests as tuberculous meningitis or tuberculomas. Tuberculous meningitis involves thick exudate in the subarachnoid space and can lead to hydrocephalus or ischemic infarcts. Tuberculomas appear as ring-enhancing lesions on imaging. Pott's disease is spinal tuberculosis that causes vertebral body collapse and kyphosis. Management involves antituberculous medications for at least 6-9 months.
Top Rated Hyderabad Call Girls Erragadda ⟟ 9332606886 ⟟ Call Me For Genuine ...
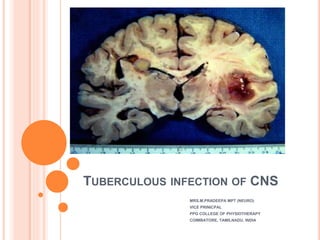
Tuberculous infection of CNS
1. TUBERCULOUS INFECTION OF CNS
MRS.M.PRADEEPA MPT (NEURO)
VICE PRINICPAL
PPG COLLEGE OF PHYSIOTHERAPY
COIMBATORE, TAMILNADU, INDIA
2. INTRODUCTION
Tuberculosis of the central nervous system (CNS)
is a highly devastating form of tuberculosis
Tuberculosis is an infection caused by one of two
Mycobacteria – Mycobacterium tuberculosis and
Mycobacterium bovis.
The disease involves the nervous system in 10% of
patients.
Can result from either haematogenous spread from
distant systemic infection (e.g. pulmonary
tuberculosis) or direct extension from local infection
(e.g. tuberculous otomastoiditis).
3. EPIDEMIOLOGY
Tuberculosis remains a leading cause of morbidity and
mortality in the developing world.
It may account for 1/6th of the 3 million of global
mortality.
CNS involvement is thought to occur in 2-5% of patients
with tuberculosis and up to 15% of those with AIDS-
related tuberculosis 6,7.
Although CNS involvement by tuberculosis is seen in all
age groups, there is a predilection for younger patients,
with 60-70% of cases occurring in patients younger than
20 years of age.
In endemic regions, tuberculomas account for as many
as 50% of all intracranial masses
Male predominance
4. RISK FACTORS
Children
HIV-infected patients
Malnutrition
Recent measles in children
Alcoholism
Malignancies
Use of immunosuppressive agents in adults
6. PATHOGENESIS OF TUBERCULOSIS
The acquisition of M. tuberculosis infection occurs through the
inhalation of droplet nuclei containing the bacilli, eventually
leading to deposition in the lung alveoli.
In the alveoli, the bacilli interact with alveolar macrophages
through a multitude of different receptors.
Numerous cytokines and chemokines are released, the
activation of a type 1 T-helper cell-mediated immune response
occurs, and, ultimately, a granuloma is formed.
Prior to the actual containment of the infection, bacilli are
filtered into draining lymph nodes, and there exists a low-level
bacteremia in which M. tuberculosis disseminates to distant
sites in the body (haematogenous seeding)
In case of CNS involvement the characteristic lesions known
as Rich’s foci tuberculous subpial or subependymal foci about
1 mm in diameter are formed
7. PATHOGENESIS
CNS TB is a three step process
1. Hematogenous seeding of meninges during
bacteremia of primary TB
2. Quiescent phase: may last from few weeks to
many years.
3. Mycobacteria in Richs foci multiply and with
immune or traumatic stimulus rupture or grow and
clinical manifestations occur.
8. PATHOGENESIS
For CNS tuberculosis, the disease begins with the
development of small tuberculous foci (Rich foci) in
the brain, spinal cord, or meninges.
The location of these foci and the capacity to
control them ultimately determine which form of
CNS tuberculosis occurs.
CNS tuberculosis manifests itself primarily as
tuberculous meningitis (TBM) and less commonly
as tubercular encephalitis, intracranial tuberculoma,
or a tuberculous brain abscess
9.
10. TUBERCULOUS MENINGITIS
This is the commonest manifestation of tuberculous
infection of the nervous system.
In children, it usually results from bacteraemia
following the initial phase of primary pulmonary
tuberculosis.
In adults, it may occur many years after the primary
infection.
Tuberculous meningitis may manifest in two forms:
1. Leptomeningitis: common
2. Pachymeningitis: rare
11. EPIDEMIOLOGY
Tuberculous meningitis, although seen in all age
groups, has a peak incidence in childhood
(particularly 0-4 years of age) in high prevalence
areas.
In low prevalence areas, it is more frequently
encountered in adolescents and adults.
12. LEPTOMENINGITIS
Common and presents with thick tuberculous exudate within
the subarachnoid space, particularly pronounced at the base
of the brain especially in the interpeduncular fossa, anterior to
the pons and around the cerebellum and may also extend into
the Sylvian fissures.
In contrast to bacterial meningitis, extension over the surfaces
of the cerebral hemispheres is relatively uncommon.
Eventually, mass-like regions of caseous necrosis can form
within this exudate, representing extra-axial tuberculomas.
CSF flow is disrupted, and obstructive hydrocephalus is
common.
An additional complication is arteritis that may result in
ischemic infarcts, which are seen in approximately a third of
cases, especially in children
13. PATCHYMENINGITIS
Tuberculous pachymeningitis is a rare form of CNS
tuberculosis characterized by a chronic tuberculous
infection leading to a dura mater involvement.
Common sites of involvement are cavernous sinuses,
floor of middle cranial fossa and tentorium.
Characterized by thick plaque-like regions of
pachymeningeal enhancement.
This term should be reserved for cases where it is an
isolated abnormality, and not confused with the
sometimes dramatic thickening of dura adjacent to
a tuberculoma.
14.
15. CLINICAL FEATURES OF TB MENINGITIS
The clinical features of tuberculous meningitis
(TBM) result from:
Infection.
Exudation – which may obstruct the basal cisterns
and result in hydrocephalus.
Vasculitis – secondary to inflammation around
vessels, resulting in infarction of brain and spinal
cord.
The basal meninges are generally most severely
affected.
16. The majority of patients are adults; childhood TBM
is now rare.
Non-specific prodromal symptoms develop over 2–
8 weeks.
Staging is useful for predicting outcome.
Stage I Early Stage II intermediate Stage III advanced
Fever (in 80%) Confusion Coma
Lethargy Cranial nerve paresis
Meningism
Vasculitis -
hemi/quadriparesis,
ataxia, dysarthria
17. Seizures may occur at the onset. Involuntary
movements (chorea, myoclonus) occur in 10%.
Atypically the illness may develop slowly over
months presenting with dementia or rapidly like
pyogenic (bacterial) meningitis.
Occasionally cerebral features prevail rather than
signs of meningitis.
Untreated, the illness may progress from phase 1 to
death over a 3-week period.
Arachnoiditis inflammatory exudate may result in
hydrocephalus/dementia/blindness
18. INVESTIGATION OF TB MENINGITIS
General: Anaemia, leucocytosis. Hyponatraemia (if inappropriate
ADH secretion occurs).
Cerebrospinal fluid
Cell count, differential count, cytology (50–4000/mm3 –
predominantly lymphocytes)
Glucose, with a simultaneous blood sugar (<50% blood glucose)
Protein (>1g/l)
Acid-fast stain, Gram stain, appropriate bacteriologic culture and
sensitivity, India ink (all causes of lymphocytic meningitis)
Cryptococcal antigen, herpes antigen (other causes of
lymphocytic meningitis)
Culture for M. tuberculosis (50–80% positive)
Polymerase chain reaction (PCR) to detect Mycobacterium DNA
– specificity and sensitivity 100% and 70%.
19. Tuberculin skin test: Positive in 50% of cases.
(Negative if recent steroids or acquired primary
infection.)
Chest x-ray:
Hilar lymphadenopathy, infiltrate, cavitations,
effusion, scar.
CT scan and MRI
Hydrocephalus, basal meningeal thickening,
infarcts, oedema, tuberculomas and obliteration of
the subarachnoid space.
22. MANAGEMENT
Normal regime:
2 months
1. Isoniazid (300 mg daily)
2. Rifampicin (600 mg daily)
3. Pyrazinamide (15–30 mg/kg daily)
Then for 6 months
1. Isoniazid and Rifampicin
Drug resistance suspected due to previous
antituberculous therapy - Add a fourth drug –
streptomycin (1 g daily) or ethambutal (25 mg/kg
daily).
23. Intrathecal therapy: Streptomycin 50 mg may be
given daily or more frequently in seriously ill
patients. When obstructive hydrocephalus occurs,
combined intraventricular (through the shunt
reservoir or drainage catheter) and lumbar
intrathecal treatment injections may be
administered.
Steroid therapy: Adjunctive steroids reduce
neurological sequelae, hearing loss and mortality
in patients with TBM without HIV.
24. TUBERCULOMA
Intracranial tuberculous granulomas, also known
as CNS tuberculomas, are common in endemic
areas and may occur either in isolation or along
with tuberculous meningitis
Tuberculomata may occur in cerebral hemispheres,
cerebellum or brain stem with or without
tuberculous meningitis, and may produce a space-
occupying effect.
Lesions may be single or multiple.
25. PATHOGENESIS OF TUBERCULOMAS
A tuberculoma is distinct from a tuberculous
abscess in that it demonstrates evidence of
granulomatous reaction and caseous necrosis
histologically.
Tuberculomas have a solid granulomatous core
made up of epitheloid cells and macrophages
containing mycobacteria and some may undergo
liquefaction.
26. CLINICAL FEATURES
The clinical presentation of CNS tuberculoma is
usually more subtle than that of TB meningitis.
Tuberculomas accompany TB meningitis in 10% of
patients
Lesions may occur in the brain, spinal cord,
subarachnoid, subdural, or epidural space
Include headache, seizures, focal neurologic
deficits, and papilledema
27. INVESTIGATION OF TUBERCULOMAS
TB organisms may not necessarily be identified in
tuberculomas, whereas they are necessary to make
the diagnosis of tuberculous abscess.
CT
Tuberculomas may appear as a round or lobulated
nodule with moderate to marked edema.
MRI
Isointense to grey matter, usually appears as ring-
enhancement
31. POTT’S DISEASE
This was first described by Percivall Pott. He noted this
as a painful kyphotic deformity of the spine associated
with paraplegia.
Tuberculous spondylitis, also known as Pott disease,
refers to vertebral body osteomyelitis and intervertebral
diskitis from tuberculosis (TB).
The spine is the most frequent location
of musculoskeletal tuberculosis, and commonly related
symptoms are back pain and lower limb
weakness/paraplegia.
This arises in the lower thoracic region, can extend over
several segments and may spread through the
intervertebral foramen into pleura, peritoneum or psoas
muscle (psoas abscess).
Chronic epidural infection follows tuberculous
osteomyelitis of the vertebral bodies.
32. EPIDEMIOLOGY
In developing countries, spinal TB is mostly a
disease of childhood or adolescence.
1/5th of TB population is in India.
3% are suffering from skeletal TB, 50% of these
suffer from spinal lesion and almost 50% are from
pediatric group.
An estimated 2 million or more patients have active
spinal tuberculosis.
The incidence is now increasing, probably due to
the development of antibiotic resistance
33.
34. PATHOLOGY
The spine is involved due to hematogenous spread via
the venous plexus of Batson.
There is usually a slow collapse of one or usually more
vertebral bodies, which spreads underneath the
longitudinal ligaments.
This results in an acute kyphotic or "gibbus" deformity.
This angulation, coupled with epidural granulation tissue
and bony fragments, can lead to cord compression.
Unlike pyogenic infections, the discs can be preserved
and it more commonly involves the thoracic spine.
In late-stage spinal TB, large paraspinal abscesses
without severe pain or frank pus are common, leading to
the expression "cold abscess".
35. TYPES OF POTT’S DISEASE
Paradiscal: This is the commonest type. In this, the
contagious areas two adjacent vertebrae along with
the intervening disc are affected.
Central: Body of single vertebrae affected leading
to early collapse of the weakened vertebrae. The
nearby disc maybe normal. The collapse may be a
‘wedging’ or ‘concertina’ collapse.
Anterior: Infection is localised to anterior part of
vertebral body. Infection spreads up and down
under the anterior longitudinal ligament.
Posterior: Posterior complex vertebrae i.e., the
pedicle, lamina, spinous process and transverse
process is affected.
36.
37. CLINICAL FEATURES
The classic systemic features of weight loss, night
fever and cachexia are often absent.
Pain occurs over the affected area and is made
worse by weight bearing.
Symptoms and signs of cord compression occur in
approximately 20% of cases.
The onset may be gradual as pus, caseous material
or granulation tissue accumulate, or sudden as
vertebral bodies collapse and a kyphosis develops.
38. STAGES ACCORDING TO CLINICAL
PRESENTATION
ACTIVE STAGE:
BACK PAIN
1. Diffuse “radicular pain”, commonest presenting complaint.
2. Presents in the arm (cervical root), girdle (dorsal root), abdomen
(dorso-lumbar root), groin (lumbar root), sciatic (lumbo-sacral root)
STIFFNESS
1. Very early symptom.
2. Protective mechanism of the body.
COLD ABSCESS
1. Patient may present with a swelling ‘cold abscess’ or problems
secondary to its compression effects on nearby vicera.
PARAPLEGIA (IF NEGLECTED IN EARLY STAGES)
DEFORMITY
CONSTITUIONAL SYMPTOMS
Fever, Weight loss, Night sweats
39. HEALED STAGE:
No systemic features but deformity persists.
Radiological evidence of bone healing
Patient may present with cold abscess or due
to its compression effects
1. Retropharyngeal abscess — Dysphagia
,dyspnea, hoarseness of voice
2. Mediastinal abscess—Dysphagia
3. Psoas abscess— Flexion deformity of hip
44. MANAGEMENT
A needle biopsy is often sufficient
Long-term anti-tuberculous therapy is commenced.
If signs of cord compression develop,
decompression is necessary.
Anterior Transthoracic Decompression with strut
graft fusion is sometimes performed. This permits
clearance of pus and caseous debris without
retracting the spinal cord.
Posterolateral approach (costotransversectomy):
One or more ribs are resected medially, along with
the transverse processes.
45. TUBERCULOUS MENINGOMYELITIS
Tuberculous meningomyelitis is a relatively rare but
serious type of nervous system tuberculosis.
This disorder is now more frequent in AIDS
patients.
This disease is caused by invasion of the spinal
cord or the spinal meninges which may result from
downward spread of intracranial infection or direct
spread from epidural infection.
Occasionally arises from rupture of local metastatic
focus; resultant infection is confined to the spinal
level.
Tuberculosis Infection of the leptomeninges results
in an exudate that encases the spinal cord and
nerve roots.
46. CLINICAL FEATURES
It can be Ascending myelitis, Root involvement,
Descending myelitis
Results in
Back pain
Root pain, paraesthesia
Weakness mainly lower limb
Pyramidal and segmental.
Sensory loss.
Sphincter disturbance
47. INVESTIGATION
Imaging may be normal while CSF shows high
protein, lymphocytes and rarely acid fast bacilli.