Pioneering Precision Medicine in Bladder Cancer: Multidisciplinary Perspectives on Personalizing Patient Care
•
0 likes•12 views

Chair and Presenter Neal D. Shore, MD, FACS, Sia Daneshmand, MD, and Guru P. Sonpavde, MD, prepared useful Practice Aids pertaining to bladder cancer for this CME/MOC/AAPA activity titled “Pioneering Precision Medicine in Bladder Cancer: Multidisciplinary Perspectives on Personalizing Patient Care.” For the full presentation, downloadable Practice Aids, and complete CME/MOC/AAPA information, and to apply for credit, please visit us at https://bit.ly/40qGkJH. CME/MOC/AAPA credit will be available until December 28, 2024.

Recommended
Recommended
More Related Content
Similar to Pioneering Precision Medicine in Bladder Cancer: Multidisciplinary Perspectives on Personalizing Patient Care
Similar to Pioneering Precision Medicine in Bladder Cancer: Multidisciplinary Perspectives on Personalizing Patient Care (20)
More from PVI, PeerView Institute for Medical Education
More from PVI, PeerView Institute for Medical Education (20)
Recently uploaded
Recently uploaded (20)
Pioneering Precision Medicine in Bladder Cancer: Multidisciplinary Perspectives on Personalizing Patient Care
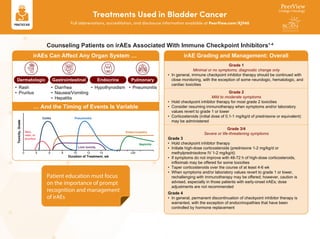
- 1. Treatments Used in Bladder Cancer Full abbreviations, accreditation, and disclosure information available at PeerView.com/XJV40 Counseling Patients on irAEs Associated With Immune Checkpoint Inhibitors1-4 Patient education must focus on the importance of prompt recognition and management of irAEs Grade 1 Minimal or no symptoms; diagnostic change only • In general, immune checkpoint inhibitor therapy should be continued with close monitoring, with the exception of some neurologic, hematologic, and cardiac toxicities Grade 2 Mild to moderate symptoms • Hold checkpoint inhibitor therapy for most grade 2 toxicities • Consider resuming immunotherapy when symptoms and/or laboratory values revert to grade 1 or lower • Corticosteroids (initial dose of 0.1-1 mg/kg/d of prednisone or equivalent) may be administered Grade 3/4 Severe or life-threatening symptoms Grade 3 • Hold checkpoint inhibitor therapy • Initiate high-dose corticosteroids (prednisone 1-2 mg/kg/d or methylprednisolone IV 1-2 mg/kg/d) • If symptoms do not improve with 48-72 h of high-dose corticosteroids, infliximab may be offered for some toxicities • Taper corticosteroids over the course of at least 4-6 wk • When symptoms and/or laboratory values revert to grade 1 or lower, rechallenging with immunotherapy may be offered; however, caution is advised, especially in those patients with early-onset irAEs; dose adjustments are not recommended Grade 4 • In general, permanent discontinuation of checkpoint inhibitor therapy is warranted, with the exception of endocrinopathies that have been controlled by hormone replacement irAE Grading and Management: Overall • Diarrhea • Nausea/Vomiting • Hepatitis Gastrointestinal • Hypothyroidism Endocrine • Rash • Pruritus Dermatologic • Pneumonitis Pulmonary irAEs Can Affect Any Organ System … … And the Timing of Events Is Variable Duration of Treatment, wk 0 4 6 8 10 12 14 >30 Toxicity, Grade Colitis Endocrinopathy Nephritis Liver toxicity Skin, rash, or pruritus Pneumonitis
- 2. Treatments Used in Bladder Cancer Full abbreviations, accreditation, and disclosure information available at PeerView.com/XJV40 Educating Patients About ADCs5-7 Enfortumab Vedotin (EV) Sacituzumab Govitecan (SG) Dosing Schedule 2 doses in a 21-d cycle Infusion Time Administered over 3 h for the first dose, with subsequent doses administered over 1-2 h Dose Rounding Administered over 30 min 3 doses in a 28-d cycle as monotherapy 2 doses in a 21-d cycle in combination with pembrolizumab Available as 20-mg and 30-mg vials, allowing flexibility with dose rounding Available as a 180-mg vial Assess patients with a thorough history and physical examination Screen for pre-existing neuropathy or diabetes mellitus Before a patient starts treatment with either EV or SG … • There is a risk of infusion-related reactions • Although rare, grade 3-4 reactions do occur – Infusion-site extravasation observed with EV; ensure adequate venous access prior to infusion • Hypersensitivity reactions, ranging from mild to anaphylaxis, have been seen within 24 h of SG administration – Premedicate with an antipyretic and H1 and H2 blockers prior to each infusion – Have medication and emergency equipment to treat such reactions ready for immediate use • Monitor patients during the infusion and for ≥30 min after completion of infusion Safety Considerations With ADCs Peripheral Neuropathy • Generally resolves/remains at grade 1 Hyperglycemia • Monitor blood glucose in patients with/at risk for diabetes or hyperglycemia Ocular Disorders • Monitor and consider prophylactic artificial tears for dry eyes and treatment with ophthalmic topical steroids after an ophthalmic examination Neutropenia • Consider growth factor support • Dose reduction/hold Diarrhea • Educate patients • Maintain hydration with electrolytes • Antidiarrheal medications/best supportive care Management Strategies for Common AEs EV SG
- 3. Treatments Used in Bladder Cancer Full abbreviations, accreditation, and disclosure information available at PeerView.com/XJV40 1. Martins F et al. Nat Rev Clin Oncol. 2019;16:563. 2. Postow MA et al. N Engl J Med. 2018;378:158-168. 3. Schneider BJ et al. J Clin Oncol. 2021;39:4073-4126. 4. NCCN Clinical Practice Guidelines in Oncology. Management of Immunotherapy-Related Toxicities. Version 3.2023. https://www.nccn.org/ professionals/physician_gls/pdf/immunotherapy.pdf. 5. Hanna KS et al. Am J Health-Syst Pharm. 2022;79:629-635. 6. Trodelvy (sacituzumab govitecan-hziy) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761115s035lbl.pdf. 7. Padcev (enfortumab vedotin) Prescribing Information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/761137s020lbl.pdf. 8. Knowles MA et al. Nat Rev Cancer. 2015;15:25-41. 9. Nimgaonkar N et al. JAMA Oncol. 2022;8:1070-1072. 10. LoriotY et al. N Engl J Med. 2019;381:338-348. 11. Siefker-Radtke AO et al. Lancet Oncol. 2022;23:248-258. FGFR Mutations Are Frequently Observed in Bladder Cancer8,9 Erdafinitib: Understanding Safety Considerations10-11 Patients ideally undergo testing upon diagnosis Options include specifically testing tumors for FGFR3 alterations (eg, RT-PCR companion assay) or more comprehensive approaches (eg, NGS panels, liquid biopsy) Both nurses and oncologists have important roles in educating patients on the importance of genomic testing Eligibility for FGFR inhibition requires testing for genomic alterations • FGFR3 inhibitors are associated with unique AEs • Oral hygiene critical; mucositis and other oral toxicities can be a concern • Monitor for skin and nail toxicities, referring to dermatology and podiatry as needed • Close monitoring and supportive care is important General Guidance on AEs Associated With FGFR3 Inhibitors • Erdafitinib also inhibits FGFR signaling in the proximal renal tubule, impairing function of the sodium-dependent phosphate co-transporter • Dietary phosphate may require restriction – Consult a nutrition professional (eg, registered dietitian, nutritionist) for individualized dietary planning – Consider adding a non–calcium- containing phosphate binder (eg, sevelamer carbonate) • Recommended ophthalmologic examinations – Monthly for first 4 mo; every 3 mo thereafter – At any time for visual symptoms • For any occurrence of central serous retinopathy (CSR)/retinal pigment epithelial detachment (RPED): – Withhold erdafitinib; discontinue permanently if symptoms do not resolve in 4 wk – Discontinue permanently for grade 4 CSR/RPED Bladder lumen Lamina propria Inner muscle Outer muscle Tis Ta T1 T2a T2b T3 T4 Tumor invades adjacent tissues and organs Tumor invades perivesical tissue Tumor invades deep muscle Tumor invades superficial muscle Tumor invades subepithelial connective tissue Noninvasive papillary carcinoma Carcinoma in situ Urothelium Non-Muscle Invasive Muscle Invasive Metastatic >60% ~30% ~30% ~20% Hyperphosphatemia Ocular Toxicities
- 4. Expanding Role of Therapeutic Approaches in Bladder Cancer Full abbreviations, accreditation, and disclosure information available at PeerView.com/XJV40 Neoadjuvant immunotherapy is administered before surgery and can reduce the size of the primary tumor as well as eliminate residual cancer cells left after surgery Rationale • Lower disease burden and intact immune system • T-cell response generated against in situ primary tumor with diverse antigen load • Fast endpoints to assess response • Allows for translational research: biologic and immunologic correlative studies Rationale • Immunologic pathways are disrupted by surgical stress • No risk for delaying surgery with adjuvant versus neoadjuvant approach • Prior chemotherapy or other systemic/local therapies may help augment immune responses Adjuvant immunotherapy is administered after surgery and leads to an increase in activated T cells that can eliminate residual cancer cells in the tumor bed Comparison of Neoadjuvant and Adjuvant Treatment Approaches1 Immunotherapy T cells T-cell activation Resection surgery Solid tumor Resection surgery Immunotherapy T-cell activation and additional immunotherapy Tumor cells Artery Healthy cells Immunotherapy
- 5. Expanding Role of Therapeutic Approaches in Bladder Cancer Full abbreviations, accreditation, and disclosure information available at PeerView.com/XJV40 Select Clinical Trials for NMIBC3 Pembrolizumab FDA approved for the treatment of patients with BCG-unresponsive, high-risk NMIBC with carcinoma in situ with or without papillary tumors who are ineligible for or have elected not to undergo cystectomy based on the KEYNOTE-057 trial2 Clinical Trials Testing TAR-200 • Phase 2 SunRISe-1: TAR-200 in BCG-unresponsive • Phase 2 SunRISe-3: TAR-200 in BCG-naive • Phase 1 TAR-210: FGFR alterations Intravesical drug delivery system that enables a sustained release of gemcitabine (TAR-200) or erdafitinib (TAR-210) into the bladder, increasing the dwell time of the local drug concentration TAR-200/TAR-210 Clinical Trials Testing BCG + IO • Phase 3 POTOMAC: BCG + durvalumab • Phase 3 KEYNOTE-676: BCG + pembrolizumab Key Eligibility Criteria • High-risk NMIBC • No prior BCG therapy BCG induction/maintenance + CPI BCG induction only + CPI BCG induction + maintenance R
- 6. Expanding Role of Therapeutic Approaches in Bladder Cancer Full abbreviations, accreditation, and disclosure information available at PeerView.com/XJV40 1. Versluis JKM et al. Nat Med. 2020;26:475-484. 2. Balar AV et al. Lancet Oncol. 2021;22:919-930. 3. clinicaltrials.gov. Approaches for MIBC3 Nivolumab FDA approved for the adjuvant treatment of patients with MIBC who are at high risk of recurrence after undergoing radical resection based on the CheckMate -274 trial Cisplatin-Eligible Trials • Phase 3 ENERGIZE: gem/cis ± nivolumab (fully accrued N = 861) • Phase 3 NIAGARA: gem/cis ± durvalumab (fully accrued N = 1,063) • Phase 3 KEYNOTE-866: gem/cis + pembrolizumab (fully accrued N = 907) • Phase 3 KEYNOTE-B15/EV-304: pembrolizumab + EV Cisplatin-Ineligable Trials • Phase 3 KEYNOTE-905/EV-303: pembrolizumab + EV • Phase 3 VOLGA: durvalumab + tremelimumab + EV • Phase 2 SunRISe-4: TAR-200 + cetrelimab R Cisplatin Ineligible Neoadjuvant Phase 1:1:1 IO IO + novel agent Radical cystectomy and pelvic lymph node dissection Adjuvant Phase IO IO + novel agent Observation R Cisplatin Eligible Radical cystectomy and pelvic lymph node dissection Neoadjuvant Phase Adjuvant Phase IO + chemo or IO + novel agent Placebo + chemo IO or IO + novel agent Placebo 1:1 First-Line: • Phase 2 BAYOU: durvalumab ± olaparib in platinum-ineligible patients • Phase 3 NILE: durvalumab + chemo ± tremelimumab vs chemo • Phase 3 CheckMate -901: nivolumab + gem/cis vs gem/cis • Phase 3 EV-302/KEYNOTE A-39: enfortumab vedotin + pembrolizumab vs chemo Second-Line: • Phase 2 DS8201-A-U105: T-DXd + nivolumab • Phase 2 DESTINY PanTumor02: T-DXd in HER2+ mUC • Phase 2 NORSE: erdafitinib + cetrelimab vs erdafitinib • Phase 3 THOR: erdafitinib vs chemo vs pembrolizumab in patients with selected FGFR mutations • Phase 3 TROPiCS-04: sacituzumab govitecan vs chemo Approaches for Unresectable or mUC3
- 7. Patient Resources for Healthcare Professionals1 Full abbreviations, accreditation, and disclosure information available at PeerView.com/XJV40 1. https://bcan.org. The Bladder Cancer Advocacy Network (BCAN) is a national advocacy organization that is committed to advancing bladder cancer research and supporting those impacted by the disease. BCAN provides free online and printed educational resources designed to help patients, caregivers, and the medical community learn about bladder cancer and treatment options. • Printed materials • Patient videos • Webinars • Podcasts • Treatment matrix • Clinical trials dashboard • Bladder cancer support line: 833-ASK-4-BCA Get Yours Today!