
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Peritoneum
Similar to Peritoneum (20)
Recently uploaded
Recently uploaded (20)
Peritoneum
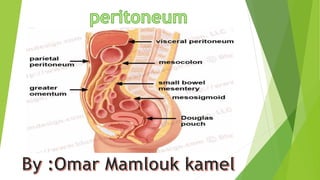
- 2. Peritoneum The peritoneum is a nearly continuous membrane that lines the peritoneal cavity and separates viscera from the abdominal wall. In men, the peritoneum is a closed system. In women, it is an “open system” interrupted in the pelvis by the fallopian tubes, which provide a final conduit for transmission of pathogens and chemicals from the genital tract to the peritoneal cavity. The cells that line the peritoneal cavity and those that form the serosa of the ovary are both of celomic epithelial origin. Thus, it is not clear whether tumors and tumor-like lesions of peritoneum and ovary (i.e., müllerian epithelial lesions) are the same entity in both locations. Many inflammatory lesions involve the peritoneum. Granulomatous peritonitis develops as a response to foreign materials such as sutures, surgical glove powder or contrast media. Exposure to intestinal contents after perforation (e.g., in Crohn disease or diverticulitis); rupture of a mature cystic teratoma (dermoid cyst) of the ovary; and, of course, tuberculosis can also cause peritoneal inflammation. Reactive mesothelial proliferation occurs with the slightest irritation.
- 5. PATHOPHYSIOLOGY: The pathogenesis of endometriosis is uncertain. Several theories, not necessarily mutually exclusive, are proposed: 1. Transplantation of endometrial fragments to ectopic sites 2. Metaplasia of the multipotential celomic peritoneum 3. Induction of undifferentiated mesenchyme in ectopic sites to form lesions after exposure to substances released from shed endometrium TRANSPLANTATION: The most widely accepted theory holds that menstrual endometrium refluxes through the fallopian tubes and implants at ectopic sites. It is known that retrograde menstruation through the fallopian tubes occurs in 90% of women. A mechanism involving lymphatic and hematogenous dissemination would explain endometriosis in lymph nodes and at distant organ sites like the lungs and kidneys. The observation that pulmonary endometriosis occurs almost exclusively in women who have had uterine surgery supports this contention. CELOMIC METAPLASIA: This theory proposes that endometriosis arises by endometrial metaplasia of peritoneal serosa or serosa-like structures. Thus, if appropriately stimulated, the pelvic peritoneum may differentiate into any type of müllerian epithelium. INDUCTION THEORY: This concept suggests that something secreted by the endometrium makes endometrial epithelium and stroma develop in ectopic sites.
- 6. PATHOLOGY: The earliest lesions of endometriosis may be yellow-red stains, reflecting breakdown of blood products. Red lesions, which also occur early in the disease, are actively growing foci of endometriosis. Operative specimens usually contain black lesions showing some degree of resolution. These 1–5-mm foci on the ovary and peritoneal surfaces are called “mulberry” nodules. With repeated cycles of hemorrhage and subsequent fibrosis, affected surfaces may scar and become grossly brown (“powder burns”). Over time, fibrous adhesions may become more pronounced and lead to complications, such as intestinal obstruction. Repeated hemorrhage in the ovaries may turn endometriotic foci into cysts up to 15 cm in diameter containing inspissated, chocolatecolored material (“chocolate cysts”). Endometriosis is characterized by ectopic normal endometrial glands and stroma. Occasionally, healed foci may contain only fibrous tissue and hemosiderinladen macrophages, which by themselves are not diagnostic. Immunohistochemical demonstration of CD-10 can be diagnostic.
- 8. CLINICAL FEATURES: Symptoms of endometriosis depend on where implants are located. Dysmenorrhea, caused by implants on uterosacral ligaments, is common. Lesions swell just before or during menstruation, producing pelvic pain. Half of women with dysmenorrhea have endometriosis. Other symptoms include dyspareunia and cyclical abdominal pain. Infertility is the primary complaint in a third of women with endometriosis . The hormonal milieu in a woman who does not achieve pregnancy encourages development of endometriosis. In turn, once endometriosis develops, it contributes to the infertile state and a vicious circle is established. Conversely, pregnancy may alleviate the disease. Conservative surgery to restore pelvic anatomy helps many women with endometriosis to become pregnant. Malignancy occurs in about 1%–2% of cases of endometriosis . Clear cell and endometrioid tumors are the most frequent forms. Adenosarcoma, although rare, is the most common sarcoma.
- 9. MESOTHELIAL TUMORS Mesothelial tumors range from benign to multicentric aggressive malignancies. Adenomatoid Tumors Are Benign Mesothelial Neoplasms, Mainly of Fallopian Tubes It is encountered in the fallopian tubes and in subserosal tissue of the uterine corpus near the fallopian tubes. It is rare elsewhere in the peritoneum. Well-Differentiated Papillary Mesotheliomas are rare in women of reproductive age. They are typically asymptomatic and usually found incidentally at operation. These tumors are solitary, small, broad-based, wart-like polypoid or nodular excrescences with a single layer of small bland cuboidal cells covering thick papillae . They often resemble serous epithelial tumors of the ovary, but the two are treated differently. Diffuse Peritoneal Malignant Mesotheliomas Are Invariably Fatal These tumors arise from peritoneal mesothelium. They are rare in women and constitute only a small proportion of all malignant mesotheliomas, most of which are pleural. They must be distinguished from serous adenocarcinomas, including those arising from the peritoneal surface itself and those metastatic from the ovary, because they are treated differently and have much different survival rates. Most patients are middle-aged or postmenopausal with nonspecific symptoms such as ascites, abdominal discomfort, digestive disturbances and weight loss. Unlike pleural tumors, asbestos exposure is uncommon in women with peritoneal mesothelioma, but up to 2 million fibers per gram wet weight have been reported in some tumors.
- 11. PATHOLOGY: Diffuse malignant mesothelioma extensively involves and thickens the peritoneum and serosa of the various abdominal and pelvic organs. It has a tubulopapillary to solid pattern. Unlike pleural mesothelioma, the sarcomatoid type is rare. The epithelial variant displays polygonal or cuboidal neoplastic cells with abundant cytoplasm. Thrombomodulin, calretinin, cytokeratin 5/6 and HBME-1 are markers of malignant mesothelioma, whereas CA-125, CEA and estrogen and progesterone receptors (ER and PR) are markers of ovarian epithelial tumors. No effective treatment is available. SEROUS TUMORS (PRIMARY AND METASTATIC) Unlike the ovary, which features a wide range of tumors, serous tumors are virtually the only type found in the peritoneum. Mucinous tumors in the peritoneum are metastases from a primary cancer of the appendix or ovary. Serous Tumors of Borderline Malignancy Resemble the Corresponding Ovarian Neoplasms Most serous borderline tumors in the peritoneum are metastases from the ovary, but some may be primary in the peritoneum. In the latter case, serous peritoneal tumors without invasion are usually benign; those that are invasive carry a worse prognosis.
- 12. Whether in the ovary or the peritoneum, borderline serous tumors are characterized by papillary processes, small clusters of cells, cell stratification, detached cellular clusters, nuclear atypia and mitotic activity in the absence of invasion. Implants appear as fine granularities or small nodules with clusters of blunt papillae or glandular structures, often having complex cellular tufts . Psammoma bodies are common and may fill the core of the papillae. Mild to severe cytologic atypia with some stratification is common but is substantially less than that seen in adenocarcinoma Serous Adenocarcinoma Occurs in Women with Normal Ovaries The frequency of serous adenocarcinoma arising de novo in the peritoneum is estimated as 10% of its counterpart in the ovary. The mean age of women with this tumor is 50–65 years. The diagnosis of a primary peritoneal tumor requires demonstration of normal ovaries. Abdominal pain and ascites are frequent presentations. Like ovarian cancer, serous adenocarcinoma primarily in the peritoneum may have a familial basis and can metastasize to distant locations. PSEUDOMYXOMA PERITONEI is the accumulation of jelly-like mucus in the pelvis or peritoneum. Previously interpreted as spread from mucinous ovarian tumors, pseudomyxoma peritonei is now understood to derive largely from mucusproducing adenocarcinomas of the appendix.
- 13. The condition may be extensive and appear as semisolid gelatin covering all abdominal structures, or there may be little more than a slightly thickened gelatinous coat over a focal area of bowel or omentum. The appendix is commonly enlarged or adherent to an omentum covered with the gelatinous material. Within the gelatin are strips of very well-differentiated, intestinal-type, mucinous epithelium. If only isolated foci are present, the epithelium may be so well differentiated that it resembles a simple mucinous adenoma. Cribriform patterns or other histologic features of malignancy, such as signet-ring cells or glands, are seen on occasion and warrant a diagnosis of adenocarcinoma. Low-grade tumors are usually treated for cure, which entails aggressive surgical debulking and intraperitoneal chemotherapy. The 5-year survival is under 50%.