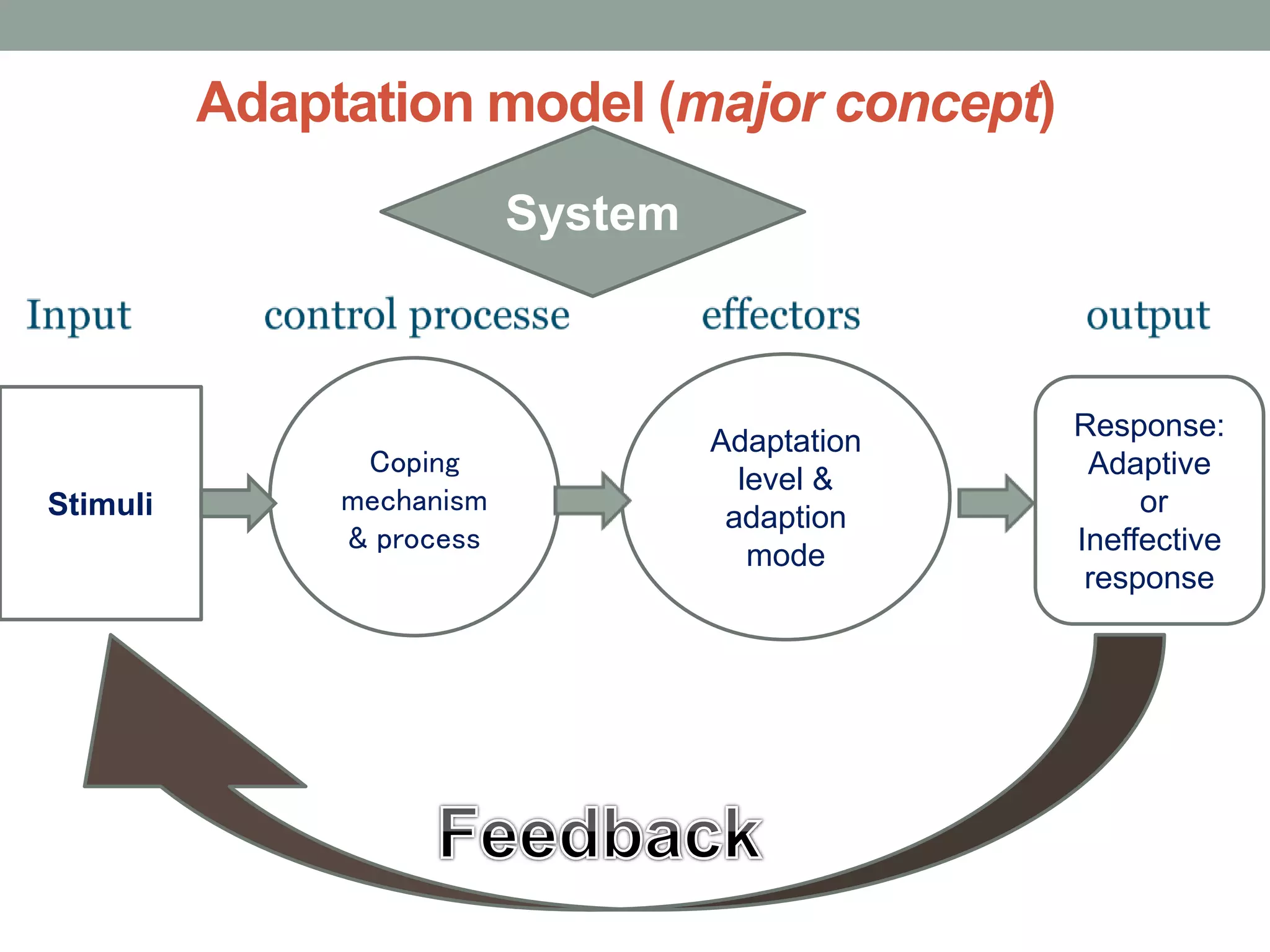
The document provides an overview of the Roy Adaptation Model (RAM) developed by Sister Callista Roy. It outlines Roy's background and credentials, the theoretical sources and concepts of RAM, including stimuli, coping mechanisms, adaptation levels, and response. RAM views the person as an adaptive system interacting with the environment. Nursing aims to promote positive adaptation. The model can guide nursing practice, education, and research by assessing and promoting a person's adaptation. Some critiques of RAM include its complexity and theoretical jargon.