5. MASTICATION :
• Rhythmic opposition and separation of jaws with
the
involvement of teeth ,lips ,cheeks and tongue for
chewing of food in order to prepare it for
swallowing and digestion.
• Main purpose of mastication is to reduce the
size of food particles to a size that is convenient
for swallowing (bolus formation) with the help
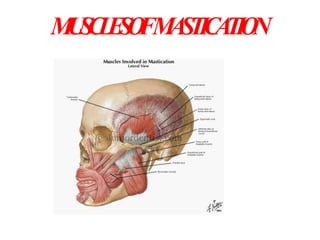
6. MUSCLE OF MASTICATION
• The muscles which are required for mastication
are known as the muscles of mastication, These
muscles help mainly in the movement of the
mandible and not the maxilla as maxilla is an
integral part of the skull and the mandible being
the only movable bone in the skull.
• There are many muscles which help in the
process of mastication but the main muscles
which take part in the process are
8. SECONDARY MUSCLES OF
MASTICATION
• Suprahyo
id
• Digastric
• Stylohyoid
• Mylohyoid
• Geniohyoi
d
• Infrahyoid
muscles
• Sternohyoid
• Thyrohyoid
• Omohyoid
9. THESE MUSCLES ATTACHED TO
MANDIBLE ARE PRIMARILY
RESPONSIBLE FOR :
• ELEVATING
• DEPRESSING
• LATERAL MOVEMENT
• RETRUDING
10. • They are funtionally classified
as:
Jaw elevator
1. Masseter
2. Medial pterigoid
3. Temporalis
Jaw depresser
1. Lateral pterigoid
2. Digastric
3. Geniohyoid
11.
12. LATERAL VIEW OFA FOUR WEEK EMBRYO SHOWING
MUSCLES DERIVED FROM BRANCHIALARCHES
13. COMMEN CHARATERSTIC OF
ALL MUSCLE OF
MASTICATION
All are inserted to the
mandible.
All are innervated by the mandibular
division of the trigeminal nerve.
All are concerned for biting and
chewing. FUNCTIONS
To move the mandible.
To secure then stabilize the mandibular
positions.
To determine the direction of
mandibular movements .
14. Masseter
• The masseter is a thick, somewhat
quadrilateral muscle, consisting of two
parts, superficial and deep. The fibers of
the two portions are continuous at their
insertion. The masseter muscle is
sometimes the target of plastic jaw
reduction surgery.
15.
16.
17.
18. • MIDDLE LAYER
• Origin -anterior 2/3 of the deep
surface and posterior 1/3 of the
lower border of the zygomatic arch,
• Insertion - middle part of ramus.
• DEEP LAYER:
• Origin -deep surface of the
zygomatic arch,
• Insertion - upper part of the
ramus and into the coronoid
process.
19.
20.
21. Origin : zygomatic arch and maxilla
Insertion : coronoid process,
ramus of mandible
Artery Supply :masseteric artery
Nerve supply : mandibular nerve (V3)
Actions : elevation (as in closing of the
mouth) and protraction of mandible
22. ACTIONS OF MASSETER
Actions:
• Elevates the mandible to close
the mouth and to occlude the
teeth in mastication.
• Its activity in the resting
position is minimal.
• It has a small effect in side-to-
side movement, protraction and
retraction.
23.
24.
25. Palpation
• The patient is asked to clench their teeth
and, using both hands, the practitioner
palpates the masseter muscles on both
sides extraorally, making sure that the
patient continues to clenchduring the
procedure.
• Palpate the origin of the
masseter bilaterally along the
zygomatic arch
and continue to palpate down the body of
the mandible where the masseter is
28. Clinical Importance of
Masseter Muscle of
Mastication:
• Masseter muscle can be palpated both intraorally
and extraorally
• The masseter muscle is sometimes the target of
plastic jaw reduction surgery.
• The muscle that commonly undergoes Hypertrophy in
Bruxism is Masseter
• Because of the Multipennate arrangement of fibers
masseter is a very powerful muscle
30. Temporalis
The temporal muscle, also known as the
temporalis, is one of the muscles of mastication. It
covers much of the temporal bone.
Structure :
It arises from the temporal fossa and the deep part of
temporal fascia. It passes medial to the zygomatic
arch and inserts onto the coronoid process of the
mandible.
The temporal muscle is covered by the temporal
fascia, also known as the temporal aponeurosis.
The muscle is accessible on the temples, and can
be seen and felt contracting while the jaw is
clenching and unclenching.
31.
32.
33.
34.
35.
36.
37. Origin and Insertion: From the Parietal bone
of the skull and is inserted on the coronoid
process of the mandible.
Arterial supply: The Deep Temporal
artery supplies the large muscle.
Nerve Supply: Trigeminal nerve( this nerve
has been associated with being the cause
of Headache and migrane.
Embryology :The temporalis is derived from
the first pharyngeal arch in development.
38. Function
s:
• Elevation of the mandible
• Retraction of the mandible.
• Crushing of food between the molars.
• Posterior fibers draw the mandible
backwards
after it has been protruded.
• It is also a contributor to side to side
grinding movement.
39. ACTIONS OF
TEMPORALIS
• Elevates the mandible, this
movement requires both the upward
pull of anterior fibers and backward
pull of the posterior fibers.
• Posterior fibers draw the mandible
backwards after it has been
protruded.
• It is also a contributory to side to
side grinding movement.
46. LATERAL PTERYGOID
ATTACHMENTS
It is a short thick muscle with two parts
or head
• UPPER head arise from infratemporal
surface and infratemporal crest of
greater wing of sphenoid bone
• LOWER head arise from lateral surface
of lateral pterygoid plate.
• Its fibers pass backwards and laterally
to be inserted into a depression
(pterygoid fovea)on the front of the
neck of the mandible and into the
articular capsule and disc of the
temporomandibular articulation.
47.
48.
49.
50. BLOOD SUPPLY
Pterygoid branch of
2nd part of maxillary
artery
NERVE SUPPLY
Nerve to lateral
pterigoid branch
anterior division of
trigiminal nerve
51. ACTIONS OF LATERAL
PTERYGOID
• Assists in opening the mouth with suprahyoid muscles.
• Right lateral pterygoid and right medial pterygoid turns the
chin to left side as a part of grinding movement.
• When the medial and lateral pterygoids of two sides act
together they protrude the mandible so that the lower incisors
project in front of the other.
• The upper (superior) head being involved in chewing
52. The combinded efforts of the
Digastrics and Lateral Pterygoids
provide for natural jaw opening.
58. Medial Pterygoid
muscle:
• It is a thick muscle of mastication.
Origin and Insertion :
• It Arises lateral pterygoid plate, and
from the maxillary tuberosity.
• Insertion is seen on the Medial
angle of the Mandible
59.
60. NERVE SUPPLY
• Branch of the main
trunk of the
mandibular nerve.
BLOOD SUPPLY
• Pterygoid branch of
2nd part of maxillary
artery
66. • gently palpate them on the medial aspect of the
jaw,
• simultaneously from both inside and outside the
mouth
67. Clinical Importance of Medial
Pterygoid Muscle:
• Medial Pterygoid muscle can
be palpated only intraorally
• Most commonly involved in
MPDS
• Trismus following inferior
alveolar nerve block is mostly
due to involvement of medial
pterygoid muscle
68. The 4 primary muscles of mastication are in turn supported
or supplemented by few secondary muscles known as
SUPRAHYOID GROUP of muscles they are
• DIGASTRIC
• MYLOHYOID
• GENIOHYOID
69. DIAGASTRIC MUSCLE
• Two bellies united by tendon
• The muscle has secondary role in mastication as a
depressor muscle adding to the action of lateral
pterygoid muscle when mouth is to be opened against
resistance.
70. MYLOHYOID MUSLE
• Flat triangular
• The secondary role of this muscle is evident as a
depressor seen in action when mouth is to be opened
against resistance.
• It elevates the floor of mouth to help in deglutition.
71.
72. GENIOHYOID
• Short and narrow musle lies above
mylohyoid
• When the hyoid bone is fixed, it
depresses the mandible
74. IMPORTANT FACTS ABOUT
MASTICATION
• There are about 15 chews in a series from the time of food
entry until swallowing
• Average jaw opening during chewing is between 16-20mm
• Average lateral displacement on chewing is between 3 and
5mm
• Men chew faster and have a shorter occlusal phase than
women, it also depends on the type of food
76. TETANUS(LOCK JAW)
• Caused by exotoxins of gram positive bacillus Clostridium
tetani.
• Disease of the nervous system characterized by intense
activity of motor neuron and resulting in severe muscle
spasm
CLINICAL FEATURES
• Pain and stiffness in the jaws and neck muscles ,with
muscle rigidity producing trismus and dysphagia
77. TREATMENT
• All patients should receive antimicrobial drugs
• Active and passive immunization.
• Surgical wound care
• Anticonvulsant if indicated
78. BRUXISM
Bruxism : Jaw clenching, with or without forcible excursivemovements,
where the intensity of the clenching dictates the severity (or lackof)
grinding .
Clenching- It can occur as a brief rhythmic strong contractions of the jaw
muscles during eccentric lateral jaw movements, or in maximum
intercuspation,
Causes
1) Associated with stressfulevents
2)Non stress related or hereditary
79. • Bruxismmay lead to
-tooth wear
-fracture of the teeth or restoratrion
-uncosmetic muscle hypertrophy
• Treatment
-coronoplasty
-maxillary stabalization appliance
80.
81. MYOFACIAL PAIN
DYSFUNCTION SYNDROME
• Pain
• Muscle tenderness
• Clicking in the joint
• Limitation in the mouth opening
TREATMENT
• Physiotherapy and Myotherapeutic exercises
• Transcutaneous Electronic Nerve Stimulation
• Muscle relaxants
• surgery
82.
83.
84. REFERENCES
• B.D.Chaurasias, Human anatomy
• Shafer,Hine,Textbook of oral
pathology
• Human anatomy A K Dutta
• Grays Anatomy
• Journal Refernces