
Recommended
More Related Content
Similar to Thorax prt. 1.pdf
Similar to Thorax prt. 1.pdf (20)
Recently uploaded
Recently uploaded (20)
Thorax prt. 1.pdf
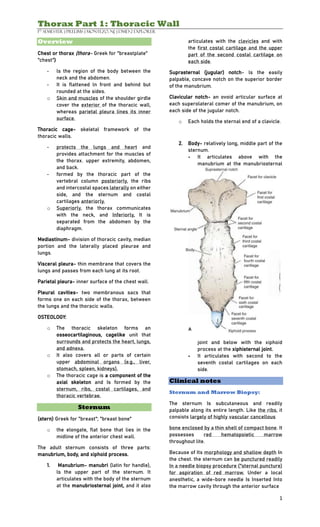
- 1. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 1 Overview Chest or thorax (thora- Greek for "breastplate" "chest") - ls the region of the body between the neck and the abdomen. - It is flattened ln front and behind but rounded at the sides. o Skin and muscles of the shoulder girdle cover the exterior of the thoracic wall, whereas parietal pleura lines its inner surface. Thoracic cage- skeletal framework of the thoracic walls. - protects the lungs and heart and provides attachment for the muscles of the thorax. upper extremity, abdomen, and back. - formed by the thoracic part of the vertebral column posteriorly, the ribs and intercostal spaces laterally on either side, and the sternum and costal cartilages anteriorly. o Superiorly, the thorax communicates with the neck, and Inferiorly, It is separated from the abdomen by the diaphragm. Mediastinum- division of thoracic cavity, median portion and the laterally placed pleurae and lungs. Visceral pleura- thin membrane that covers the lungs and passes from each lung at its root. Parietal pleura- inner surface of the chest wall. Pleural cavities- two membranous sacs that forms one on each side of the thorax, between the lungs and the thoracic walls. OSTEOLOGY: o The thoracic skeleton forms an osseocartilaginous, cagelike unit that surrounds and protects the heart, lungs, and adnexa. o It also covers all or parts of certain upper abdominal organs (e.g., liver, stomach, spleen, kidneys). o The thoracic cage is a component of the axial skeleton and Is formed by the sternum, ribs, costal cartilages, and thoracic vertebrae. Sternum (stern) Greek for "breast"; "breast bone" o the elongate, flat bone that lies in the midline of the anterior chest wall. The adult sternum consists of three parts: manubrium, body, and xiphoid process. 1. Manubrium- manubri (latin for handle), ls the upper part of the sternum. It articulates with the body of the sternum at the manubriosternal joint, and it also articulates with the clavicles and with the first costal cartilage and the upper part of the second costal cartilage on each side. Suprasternal (jugular) notch- ls the easily palpable, concave notch on the superior border of the manubrium. Clavicular notch- an ovoid articular surface at each superolateral comer of the manubrium, on each side of the jugular notch. o Each holds the sternal end of a clavicle. 2. Body- relatively long, middle part of the sternum. - It articulates above with the manubrium at the manubriosternal joint and below with the xiphoid process at the xiphisternal joint. - It articulates with second to the seventh costal cartilages on each side. Clinical notes Sternum and Marrow Biopsy: The sternum Is subcutaneous and readily palpable along its entire length. Like the ribs, it consists largely of highly vascular cancellous bone enclosed by a thin shell of compact bone. It possesses red hematopoietic marrow throughout lite. Because of Its morphology and shallow depth In the chest. the sternum can be punctured readily In a needle biopsy procedure ("sternal puncture) for aspiration of red marrow. Under a local anesthetic, a wide-bore needle Is Inserted Into the marrow cavity through the anterior surface
- 2. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 2 of the bone. The sternum may also be split In surgery to allow the surgeon to gain easy access to the heart, great vessels, and thymus. Embryology Notes Sternum development: The adult sternum consists of three parts: manubrium, body, and xiphoid process. Prenatally, lt consists of six main parts. The first and last parts remain distinguishable as the manubrium and xiphoid process, respectively. The middle four parts (sternebrae) fuse to form the body. The three main parts were named after the resemblance of the sternum to the short sword favored by Roman troops and gladiators- thus, the manubrium (handle), the body (in older terminology = gladiolus = small sword), and the xiphoid process (sword point). Ribs (cost- is Latin for "ribs), elongate, flattened, arched bones that form a large part of the thoracic wall. - consist largely of highly vascular cancellous bone enclosed by a thin shell of compact bone. True ribs (pairs 1-7)- are connected directly to the sternum via individual costal cartilages. False ribs (pairs 8 to 10)- are connected the sternum via Individual costal cartilages that join together and attach collectively to the seventh costal cartilages. Floating ribs (pairs 11 to 12) - do not attach to the sternum. TYPICAL RIBS: - a long, twisted, flat bone having rounded, smooth superior border and a sharp, thin inferior border. - The anterior end of each rib is attached to the corresponding costal cartilage. Sternum, ribs, and costal cartilages forming the thoracic: skeleton. Lateral view of the thorax showing the relationship of the surface markings to the vertebral levels. 3. xiphoid process- (xiph- Is Greek for "sword) ls the small, "pointed" (at its inferior end), most inferior part of the sternum. - a thin plate of cartilage that becomes ossified at its proximal end during adult life. - ls highly variable in size, shape, and degree of ossification. - No ribs or costal cartilages attach to it. However, the seventh costal cartilage may have a shared attachment with the xiphoid process and the body. -The xiphistemal joint lies opposite the body of the ninth thoracic vertebra. -The inferior end of the xiphoid provides attachment for the linea alba of the abdominal wall. Sternal angle (angle of louis)- articulation of the manubrium with the body forms. - can be recognized by the presence of a transverse ridge on the anterior aspect of the sternum. - an important landmark for thoracic anatomy because it marks (1) the manubriosternal joint (a symphyseal joint), (2) the attachment points of the second costal cartilages (thus, these attach to both manubrium and body), (3) a horizontal line that typically projects posteriorly onto the T4 intervertebral disc, and (4) the plane of separation between the superior and inferior mediastina.
- 3. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 3 Head- the posterior (vertebral) end of the rib and has two facets for articulation with the numerically corresponding vertebral body and that of the vertebra immediately above. Neck- the flattened, slightly constricted portion situated between the head and the tubercle. Tubercle- prominence on the outer posterior surface of the rib at the junction of the neck with the body. It has a facet for articulation with the transverse process of the numerically corresponding vertebra. Body (shaft)- long, thin, flattened, and twisted (on its long axis) part that extends from the tubercle to the anterior (sternal) end. Costal groove- elongate depression along the inferior aspect of the internal surface of the shaft of the rib. This holds the intercostal vessels and nerve. Angle- the point (usually slightly distal to the tubercle) at which the body of the rib bends sharply and turns from a lateral to a more anteriorly directed orientation. Anterior (sternal) end- flat and has a depression for the costal cartilage. FIRST RIB: Important because of its close relationship to the lower nerves of the brachial plexus and the main vessels to the arm, namely, the subclavian artery and vein COSTAL CARTILAGES: - bars of cartilage connecting the upper seven ribs to the lateral edge of the sternum and the 8th, 9th, and 10th ribs to the cartilage immediately above. - The cartilages of the 11th and 12th ribs end In the abdominal musculature - Contribute to the elasticity and mobility of the thoracic walls. - In old age, the costal cartilages tend to lose some of their flexibility as the result of superficial calcification. Vertebrae Costal facets (facet latin for little face)- are small articular surfaces at approximately the posterolateral aspect of the body, at the junction of the body and the pedicle. o Typical thoracic vertebrae (2 to 8) have two on each side. One is located superiorly (superior costal facet). One is located inferiorly (Inferior costal facet). - sites where the heads of the ribs articulate with the body. Fifth right rib, as seen from the posterior aspect.
- 4. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 4 o Adjacent typical thoracic vertebrae (2 to 8) share the articulations of ribs. - head of an individual rib articulates with both the superior costal facet of the numerically corresponding vertebral body and the Inferior costal facet of the vertebra immediately above. Demifacet (demi- French for half)- carries half of rib articulation. o The Tl vertebra has a full costal facet (instead of a superior demifacet) for the head of the first rib, plus an inferior demifacet for the superior half of the head of the second rib. o The Tl 1 and T12 vertebrae each have full costal facets (located mainly on the pedicles) instead of demifacets because the heads of ribs 11 and 12 articulate only with their own Individual vertebrae. Transverse costal facets- small articular surfaces on the transverse processes. - sites where the tubercle of each rib articulates with the transverse process. - not present on the T11 and T12 vertebrae because ribs 11and12 do not articulate with the transverse processes. Clinical Notes Cervical rib: The importance of a cervical rib is that it may cause pressure on the lower trunk of the brachial plexus, causing pain down the medial side of the forearm and hand and wasting of the small muscles of the hand. It can also exert pressure on the overlying subclavian artery and Interfere with the circulation of the upper limb. Rib excision: - Perform by surgeons to gain entrance to the thoracic cavity. A longitudinal incision ls made through the periosteum on the outer surface of the rib, and a segment of the rib ls removed. A second longitudinal incision Is then made through the bed of the rib, which is the inner covering of the periosteum. After the operation, the rib regenerates from the osteogenetic layer of the periosteum. Thoracic cage distortion: The shape of the thorax can be distorted by congenital anomalies of the vertebral column or by the ribs. Destructive disease of the vertebral column that produces lateral flexion or scoliosis results in marked distortion of the thoracic cage. Traumatic injury to thorax: Common as a result of automobile accidents. Sternum fracture: The sternum ls a resilient structure that ls held ln position by relatively pliable costal cartilages and bendable ribs. For these reasons, fracture of the sternum Is not common; however, it does occur in high-speed motor vehicle accidents. Remember that the heart lies posterior to the sternum and may be severely contused by the sternum on Impact. Rib fractures: Common chest injuries. In children, the ribs are highly elastic, and fractures in this age group are
- 5. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 5 therefore rare. Unfortunately, the pliable chest wall In the young can be easily compressed so that the underlying lungs and heart may be Injured. With Increasing age, the rib cage becomes more rigid, owing to the deposit of calcium in the costal cartilages, and the ribs become brittle. The ribs then tend to break at their weakest part, their angles. Ribs 5 through 10 are the most commonly fractured ribs. The clavicle and pectoral muscles protect the first four ribs anteriorly and the scapula and its associated muscles do so posteriorly. The 11th and 12th ribs float and move with the force of impact. Flail chest: a section of the chest wall is disconnected from the rest of the thoracic wall. If the fractures occur on either side of the sternum, the sternum may be flail. In either case, the stability of the chest wall ls lost, and the flail segment ls sucked in during lnspiration and driven out during expiration, producing paradoxical and Ineffective respiratory movements. Sternal Joints Manubriosternal joint- a cartilaginous joint between the manubrium and the body of the sternum. - A small amount of angular movement is possible here during respiration. Xiphisternal joint- a cartilaginous joint between the xiphoid process and the body of the sternum. – The xiphoid process usually fuses with the body of the sternum during middle age Joints of Heads and Ribs o The first rib and the 3 lowest ribs have a single synovial joint with their corresponding vertebral body. o second to ninth ribs, the head articulates by means of a synovial joint with the corresponding vertebral body and that of the vertebra above it. A strong intra- articular ligament connects the head to the intervertebral disc. Joints of Tubercles of Ribs o The tubercle of a rib articulates by means of a synovial joint with the transverse process of the corresponding vertebra. This joint is absent on the 11th and 12th ribs. Joints of Ribs and Costal Cartilages o These joints are cartilaginous joints. No movement ls possible here. Joints of Costal Cartilages with Sternum o The first costal cartilages articulate with the manubrium by cartilaginous joints that do not permit movement. o The second to seventh costal cartilages articulate with the lateral border of the sternum by synovial joints. o the 6th, 7th, 8th, 9th, and 10th costal cartilages articulate with one another along their borders by small synovial joints. o The cartilages of the 11th and 12th ribs do not articulate with the sternum and are embedded ln the abdominal musculature. Rib and Costal Cartilage Movements o The first ribs and their costal cartilages are fixed to the manubrium and are immobile. o The raising and lowering of the ribs during respiration are accompanied by movements in both the joints of the head and the tubercle, permitting the neck of each rib to rotate around its own axis. Thoracic Aperture superior thoracic aperture (thoracic outlet) - A narrow opening of the root of the neck - Called outlet because important vessels and nerves emerge from the thorax here to enter the neck and upper limbs. o The body of the first thoracic vertebra forms the posterior boundary of the thoracic outlet o the medial edges of the first ribs and their costal cartilages mark the lateral boundaries. o superior margin of the manubrium sterni forms the anterior border. o The outlet Is obliquely directed, facing upward and forward, and conveys the esophagus, trachea, and several vessels and nerves. Inferior Thoracic Aperture- Large opening of the abdomen where the thoracic cavity communicates. o The body of the 12th thoracic vertebra forms the posterior boundary of this opening. o curving costal margin marks its lateral boundaries o the xiphisternal joint forms the anterior border.
- 6. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 6 o The diaphragm closes the inferior aperture. SUPREPLEURAL MEMBRANE: The thoracic outlet transmits structures that pass between the thorax and the neck (esophagus, trachea, blood vessels, etc.) and for the most part lie close to the midline. Suprapleural membrane- dense facial layer which closes the thoracic outlet on either side of these structures. o tent-shaped fibrous sheet attaches laterally to the medial border of the first rib and costal cartilage; medially to the fascia investing the structures passing from the thorax into the neck; and, at its apex, to the tip of the transverse process of the seventh cervical vertebra. o It protects the underlying cervical pleura and resists the changes in intrathoracic pressure occurring during respiratory movements. ENDOTHORACIC FASCIA: o a thin layer of loose connective tissue that separates the parietal pleura from the thoracic wall. o The suprapleural membrane is a thickening of this fascia. Clinical Notes Thoracic outlet syndrome: o Obstruction of the thoracic outlet may compress these neurovascular structures in this area. o Symptoms are caused by pressure on the lower trunk of the plexus, causing pain down the medial side of the forearm and hand and wasting of the small muscles of the hand. Pressure on the blood vessels may compromise the circulation of the upper limb. Intercostal Spaces o Gaps between adjacent ribs. A needle passing through the entire depth of an intercostal space must penetrate seven structural layers. In superficial to deep sequence, the layers are the ff: 1. Skin 2. Superficial fascia 3. Deep fascia 4. Intercostal muscles 5. Endothoracic fascia 6. Extrapleural fatty layer 7. Parietal pleura o serratus anterior, may cover the intercostal muscle layer. o The three intercostal musles all act as muscles of respiration o The innermost intercostal muscle is lined internally by the endothoracic fascia, which is lined internally by a highly variable extrapleural fatty layer and then the parietal pleura. Intercoastal Muscles Three intercostal muscles fill the lntercostal spaces: external lntercostal, Internal lntercostal, and Innermost intercostal. 1. External intercostal muscle- the most superficial of the three muscle layers. o Its fibers are directed downward and forward from the inferior border of the rib above to the superior border of the rib below. o The muscle extends forward to the costal cartilage where it is replaced by an aponeurosis, the anterior (external) lntercostal membrane. 2. Internal intercostal muscle- forms the intermediate layer. o Its fibers are directed downward and backward from the subcostal groove ofthe rib above to the upper border of the rib below. o The muscle extends backward from the sternum in front to the angles of the ribs behind, where the muscle is replaced by an aponeurosis, the posterior (Internal) lntercostal membrane. 3. Innermost intercostal muscle- forms the deepest layer and corresponds to the transversus abdominis muscle In the anterior abdominal wall.
- 7. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 7 o It is an incomplete muscle layer and crosses more than one intercostal space. o It is related. internally to the endothoracic fascia and parietal pleura and externally to the intercostal nerves and vessels. Divided into three portions: 1. Transversus thoracis- anterior 2. Innermost intercostal- lateral 3. Subcostalis- posterior ACTION: o primary function of the intercostal muscles during respiration appears to be to stabilize the position of the ribs to maintain the intercostal spaces. o Their actions in elevation (external intercostals) and depression (internal lntercostals) of the ribs are most likely to occur during forced respiration. NERVE SUPPLY: o The corresponding lntercostal nerves supply the intercostal muscles. The lntercostal nerves and blood vessels (the neurovascular bundle), as in the abdominal wall, run between the middle and innermost layers of muscles. ARRANGEMENT: Intercostal vein - Intercostal artery - Intercostal nerve o
- 8. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 8 o o o o o o o o o o o o o o o Diaphragm o thin muscular and tendinous septum that separates the chest cavity above from the abdominal cavity below. o Most important muscle in respiration. o It ls dome shaped and consists of a peripheral muscular part, which arises from the margins of the thorax, and a centrally placed tendon. The origin of the diaphragm can be divided into three parts: 1. Sternal part- arising from the posterior surface of the xiphoid process. 2. Costal part- arising from the deep surfaces of the lower six ribs and their costal cartilages. 3. Vertebral part- arising by vertical columns (crura) and from the arcuate ligaments. Right crus- arises from the sides of the bodies of the first three lumbar vertebrae and the intervertebral discs. Left crus- arises from the sides of the bodies of the first two lumbar vertebrae and the intervertebral disc. o Lateral to the crura, the diaphragm arises from the medial and lateral arcuate ligaments. Medial arcuate ligament- extends from the side of the body of the second lumbar vertebra to the tip of the transverse process of the first lumbar vertebra. Lateral arcuate ligament- extends from the tip of the transverse process of the first lumbar vertebra to the lower border of the 12th rib. Median arcuate ligament- crosses over the anterior surface of the aorta, connects the medial borders of the two crura. Central tendon- where diaphragm is inserted, shaped like three leaves. o The superior surface of the tendon is partially fused with the inferior surface of the fibrous pericardium. o Some of the muscle fibers of the right crus pass up to the left and surround the esophageal orifice In a slinglike loop. Diaphragm Shape - As seen in the front, the diaphragm curves up into right and left domes ( cupulae ). o the right dome reaches as high as the upper border of the fifth rib, and the left dome may reach the lower border of the fifth rib. o The right dome lies at a higher level because of the large size of the right lobe of the liver. o The domes support the right and left lungs, whereas the central tendon supports the heart. Nerve Supply of Diaphragm o Motor nerve supply comes from the right and left phrenic nerves (C3, 4, 5). o Each phrenic nerve supplies approximately half of the diaphragm. Thus, functionally, the diaphragm operates as two hemidiaphragms. o For sensory nerve supply, phrenic nerves supply the parietal pleura and peritoneum covering the central surfaces of the diaphragm. Diaphragmatic action o On contraction, the diaphragm pulls down its central tendon and increases the vertical diameter of the thorax. Diaphragmatic function 1. Muscle of Inspiration- on contraction, the diaphragm pulls its central tendon down and increases the vertical diameter of the thorax. The diaphragm is the most important muscle used in inspiration. 2. Muscle of abdominal straining- the contraction of the diaphragm assists the contraction of the muscles of the anterolateral abdominal wall in raising the intra-abdominal pressure for micturition, defecation, and parturition. o Taking a deep breath and closing the glottis of the larynx further aids this mechanism. o The diaphragm is unable to rise because of the air trapped in the respiratory tract. Now and again, air is allowed to escape, producing a grunting sound. 3. Weight-lifting muscle- taking a deep breath, the diaphragm assists the muscles of the anterolateral abdominal wall in raising the intra-abdominal pressure to such an extent that it helps
- 9. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 9 support the vertebral column and prevent flexion. o adequate sphincteric control of the bladder and anal canal is important under these circumstances. 4. Thoracoabdominal Pump- the descent of the diaphragm decreases the intrathoracic pressure and at the same time increases the intra-abdominal pressure. o this pressure change compresses the blood in the inferior vena cava and forces it upward into the right atrium of the heart. o Lymph within the abdominal lymph vessels is also compressed, and the negative intrathoracic pressure aids its passage upward within the thoracic duct. o The presence of valves within the thoracic duct prevents backflow. Diaphragm openings The diaphragm has three main openings: 1. Aortic opening- lies anterior to the body of the 12th thoracic vertebra and between the crura. o It transmits the aorta, the thoracic duct, and the azygos vein. o the aortic opening is not a true opening within the diaphragm. Rather, it is a gap behind the posterior margin of the diaphragm. 2. Esophageal opening- lies at the level of the 10th thoracic vertebra In a sling of muscle fibers derived from the right crus. - It transmits the esophagus, the right and left vagus nerves, the esophageal branches of the left gastric vessels, and the lymphatics from the lower third of the esophagus. 3. Caval opening- lies at the level of the eighth thoracic vertebra, in the central tendon. It transmits the inferior vena cava and terminal branches of the right phrenic nerve. In addition to these openings, the sympathetic splanchnic nerves pierce the crura, the sympathetic trunks pass posterior to the medial arcuate ligament on each side, and the superior epigastric vessels pass between the sternal and costal origins of the diaphragm on each side. Clinical Notes Hiccup: The involuntary spasmodic contraction of the diaphragm, accompanied by the approximation of the vocal folds and closure of the glottis of the larynx. o Common condition that occurs after eating or drinking as a result of gastric irritation of the vagus nerve endings. o may be a symptom of disease such as o pleurisy, peritonitis, pericarditis, or uremia Diaphragm Paralysis: A single dome of the diaphragm (a hemidiaphragm) may be paralyzed by crushing or sectioning of the phrenic nerve in the neck. o This may be necessary in the treatment of certain forms of lung tuberculosis, when the physician wishes to rest the lower lobe of the lung on one side. o Accessory phrenic nerve- the fifth cervical spinal nerve joins the phrenic nerve late as a branch from the nerve to the subclavius muscle. o Recognizing that a paralyzed hemidiaphragm assumes a hyperelevated posture rather than a depressed (flattened) posture is important. Penetrating Injuries to Diaphragm: Penetrating Injuries to the diaphragm can result from stab or bullet wounds to the chest or abdomen. Any penetrating wound to the chest below the level of the nipples should be suspected of causing damage to the diaphragm until proved otherwise. Embryology Notes Diaphragm Development: The diaphragm is formed from the ff: 1. Septum transversum- forms the muscle and central tendon. o Is a mass of mesoderm that ls formed In the neck by the fusion of the myotomes of the third, fourth, and filth cervical segments. o With the descent of the heart from the neck to the thorax, the septum is pushed caudally, pulling its nerve supply with it. Thus, cervical nerves C3 to 5 form the phrenic nerve, which supplies the diaphragm. 2. 2 pleuroperitoneal membranes- largely responsible for the peripheral areas of the diaphragmatic pleura and peritoneum that cover its upper and lower surfaces. o grow medially from the body wall on each side until they fuse with the septum
- 10. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 10 transversum anterior to the esophagus and with the dorsal mesentery posterior to the esophagus. 3. Dorsal mesentery of the esophagus- which the crura develop. o The motor nerve supply to the entire muscle of the diaphragm is the phrenic nerve. o The central pleura on the upper surface of the diaphragm and the peritoneum on the lower surface are also formed from the septum transversum, which explains their sensory Innervation from the phrenic nerve Congenital herniae- occur as the result of incomplete fusion of the septum transversum, the dorsal mesentery, and the pleuroperitoneal membranes from the body wall. The herniae occur in the ff sites: 1. The pleuroperitoneal canal (more common on the left side; caused by failure of fusion of the septum transversum with the pleuroperitoneal membrane). 2. The opening between the xiphoid and costal origins of the diaphragm. 3. The esophageal hiatus. Acquired herniae- occur in esophageal opening ln the diaphragm. These herniae may be either sliding (hiatal) or paraesophageal. asd dd Levatores Costarum - Comprises 12 pairs. - Each is triangular in shape and Inserts Into the rib below its origin. - They elevate the ribs, but their role in respiration ls questionable. They may serve as proprioceptive devices. Serratus Posterior Muscles The serratus posterior superior and serratus posterior Inferior are thin, flat muscles that comprise the Intermediate layer of muscles of the back. o The superior muscle passes downward and laterally and inserts into the upper ribs. o The inferior muscle passes upward and laterally. and inserts into the lower ribs. o Both are supplied by adjacent intercostal nerves. o Both have been describe as respiratory muscles because of their alignments, with the superior muscle denoted as acting In inspiration to elevate the ribs and the Inferior muscle acting In expiration to depress the ribs. Nerves Intercostal Nerves- supply the entire thoracic wall. These nerves are the anterior rami of the first 11 thoracic spinal nerves. Subcostal Nerve- the anterior ramus of the 12th thoracic nerve lies in the abdomen and runs forward in the abdominal wall. o Each intercostal nerve enters an intercostal space between the parietal pleura and the posterior intercostal membrane. o The first six nerves are distributed within their intercostal spaces. o The seventh to ninth intercostal nerves leave the anterior ends of their intercostal spaces by passing deep to the costal cartilages, to enter the anterior abdominal wall. o The 10th and 11th nerves pass directly into the abdominal wall.
- 11. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 11 Branches Rami Communicantes- connect the intercostal nerve to a ganglion of the sympathetic trunk. - The gray and white rami are adjacent to one another. Collateral Branch- runs forward inferiorly to the main nerve on the upper border of the rib below. Lateral cutaneous Branch- reaches the skin on the side of the chest. It divides into an anterior and a posterior branch. Anterior cutaneous branch- terminal portion of the main trunk. reaches the skin near the midline. It divides into a medial and a lateral branch. Muscular Branches- run to the intercostal muscles. Pleural sensory branches- go to the parietal pleura. Peritoneal sensory branches- (7th to 11th intercostal nerves only) run to the parietal peritoneum. First intercostal nerve- joins the brachial plexus by a large branch that ls equivalent to the lateral cutaneous branch of typical intercostal nerves. o The remainder of the first intercostal nerve is small, and an anterior cutaneous branch does not exist. Second intercostal nerve- joins the medial cutaneous nerve of the arm by a large branch named the lntercostobrachial nerve. - which is equivalent to the lateral cutaneous branch of other nerves. o The second intercostal nerve supplies the skin of the armpit and the upper medial side of the arm. In coronary artery disease, pain is referred long this nerve to the medial side of the arm. o The 7th to 11th intercostal nerves supply skin and the parietal peritoneum covering the outer and inner surfaces of the abdominal wall, respectively, plus the anterolateral abdominal wall muscles (which include the external oblique, internal oblique, transversus abdominis, and rectus abdominis muscles). Vasculature The subclavian artery, axillary artery, and thoracic aorta supply the thoracic walls. o The subclavian artery provides blood through Its Superior intercostal and Internal thoracic branches. o The axillary artery supplies via its Superior thoracic and lateral thoracic branches. o The thoracic aorta gives off posterior intercostal and subcostal branches. Internal Thoracic Artery - supplies the anterior wall of the body from the clavicle to the umbilicus. - It is a branch of the first part of the subclavian artery in the neck. - It descends vertically on the pleura behind the costal cartilages, a fingerbreadth lateral to the sternum, and ends ln the sixth intercostal space by dividing into the superior epigastric and musculophrenic arteries. Branches 1. Two anterior intercostal arteries- supply the upper six intercostal spaces. 2. Perforating arteries- accompany the terminal branches of the corresponding intercostal nerves. 3. Pericardiacophrenic artery - accompanies the phrenic nerve and supplies the pericardium. 4. Mediastinal arteries- supply the contents of the anterior mediastinum. 5. Superior epigastric artery- enters the rectus sheath of the anterior abdominal
- 12. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 12 wall and supplies the rectus muscle as far as the umbilicus. 6. Musculophrenic artery- runs around the costal margin of the diaphragm and supplies the lower Intercostal spaces and the diaphragm. Clinical Notes Skin Innervation of chest wall and referred pain o The supraclavicular nerves (C3 and 4) provide the cutaneous innervation of the anterior chest wall above the level of the sternal angle. Below this level, the anterior and lateral cutaneous branches of the intercostal nerves supply oblique bands of skin in regular sequence. o An intercostal nerve not only supplies areas of skin but also supplies the ribs, costal cartilages, intercostal muscles, and parietal pleura lining the intercostal space. o 7th to 11th intercostal nerves leave the thoracic wall and enter the anterior abdominal wall to supply dermatomes on the anterior abdominal wall, muscles of the anterior abdominal wall, and parietal peritoneum. Herpes Zoster (shingles) - a relatively common condition caused by the reactivation of the latent varicella-zoster virus In a patient who has previously had chickenpox. - The lesion is seen as an inflammation and degeneration of the sensory neurons in a cranial or spinal nerve with the formation of vesicles and Inflammation of the skin. Pneumothorax- can occur if the e needlepoint misses the subcostal groove and penetrates too deeply through the parietal pleura. Hemorrhage- caused by the puncture of the intercostal blood vessels. This is a common complication, so aspiration should always be performed before Injecting the anesthetic. A small hematoma may result. Internal thoracic vein - accompanies the internal thoracic artery and drains into the brachiocephalic vein on each side. Intercostal arteries and veins Each intercostal space contains a large single posterior intercostal artery and two small anterior intercostal arteries. o Posterior intercostal arteries of the first two spaces are branches from the superior intercostal artery, a branch of the costocervical trunk of the subclavian artery. The posterior intercostal arteries of the lower nine spaces are branches of the descending thoracic aorta. o Anterior intercostal arteries of the first six spaces are branches of the Internal thoracic artery, which arises from the first part of the subclavian artery. The anterior intercostal arteries of the lower spaces are branches of the musculophrenic artery, one of the terminal branches of the internal thoracic artery. o The corresponding posterior lntercostal veins drain posteriorly into the azygos or hemiazygos veins. o The anterior lntercostal vein drain anteriorly into the internal thoracic and musculophrenic veins. Clinical Notes Internal thoracic artery in coronary artery disease treatment o In patients with occlusive coronary disease caused by atherosclerosis, the diseased arterial segment can be bypassed by inserting a graft. The graft most commonly used is the great saphenous vein of the leg Arterial Anastomoses o The anterior intercostal arteries (branches of the subclavian artery via the internal thoracic and musculophrenic arteries) and the lower nine posterior intercostal arteries (branches of the thoracic aorta) typically anastomose with one another at approximately the costochondral junctions.
- 13. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 13 o These Important connections create collateral circulatory routes that potentially allow blood flow to bypass obstructions in the thoracic aorta or the proximal part of the subclavian artery. o These anastomoses are notably prominent in circumventing the constriction present In postductal coarctation of the aorta. Thoracic wall lymph drainage o The lymph drainage of the skin of the anterior chest wall passes to the anterior axillary lymph nodes; that from the posterior chest wall passes to the posterior axillary nodes. o The lymph drainage of the intercostal spaces passes forward to the Internal thoracic nodes, situated along the Internal thoracic artery, and posteriorly to the posterior intercostal nodes and the para-aortic node In the posterior mediastinum o o o o o o o o o o o o o o o o o o o o Needle thoracostomy - is creating and maintaining an opening into the thoracic cavity by using a needle. - necessary in patients with tension pneumothorax (air in the pleural cavity under pressure) or to drain fluid (blood or pus) away from the pleural cavity to allow the lung to reexpand. Tube Thoracostomy - The preferred insertion site for a tube thoracostomy is the fourth or fifth intercostal space at the anterior axillary line. - The tube Is Introduced through a small Incision. Thoracotomy - making an incision through the thoracic wall into the pleural space. - This may be a lifesaving procedure in patients with penetrating chest wounds with uncontrolled intrathoracic hemorrhage. Anatomic and physiologic Thoracic changes with aging Certain anatomic and physiologic changes take place in the thorax with advancing years: o The rib cage becomes more rigid and loses its elasticity as the result of calcification and even ossification of the costal cartilages. This also alters their usual radiographic appearance. o The stooped posture (kyphosis), so often seen in the old because of degeneration of the intervertebral discs and/ or bodies, decreases the chest capacity. o Disuse atrophy of the thoracic and abdominal muscles can result In poor respiratory movements. o Degeneration of the elastic tissue In the lungs and bronchi results In impairment of the movement of expiration.
- 14. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 14 Surface Anatomy Anterior Chest wall Suprasternal notch- the superior margin of the manubrium sterni and is easily felt between the prominent medial ends of the clavicles in the midline. - It Iies opposite the lower border of the body of the second thoracic vertebra. Sternal angle (angle of louis)- angle made between the manubrium and the body of the sternum. - It Iies opposite the intervertebral disc between the fourth and fifth thoracic vertebrae. Xiphisternal Joints- the joint between the xiphoid process of the sternum and the body of the sternum. - Lies opposite the body of the ninth thoracic vertebra Subcostal angle- situated at the inferior end of the sternum, between the sternal attachments of the seventh costal cartilages. Costal margin- the lower boundary of the thorax and is formed by the cartilages of the 7th, 8th, 9th, and 10th ribs and the ends of the 11th and 12th cartilages. - The lowest part of the costal margin is formed by the 10th rib and lies at the level of the third lumbar vertebra. Clavicle- subcutaneous throughout Its entire length and can be easily palpated. It articulates at Its lateral extremity with the acromion process of the scapula. Ribs o The first rib lies deep to the clavicle and cannot be palpated. o The 12th rib can be used to identify a particular rib by counting from below.
- 15. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 15 Diaphragm o The central tendon of the diaphragm lies directly behind the xiphlstemal joint. o In the midrespiratory position, the summit of the right dome of the diaphragm arches upward as far as the upper border of the fifth rib In the midclavicular line, but the left dome only reaches as far as the lower border of the fifth rib. Nipple o In the male, the nipple usually lies in the fourth intercostal space about 4 in. (10 cm) from the midline. o In the female, its position is not constant. However, the T4 dermatome always crosses the nipple in both sexes regardless of the form of the breast. Apex base of the heart o The lower portion of the left ventricle forms the apex of the heart. o The apex of the heart being thrust forward against the thoracic wall as the heart contracts causes the apex beat. (The heart Is thrust forward with each ventricular contraction because of the ejection of blood from the left ventricle Into the aorta; the force of the blood in the aorta tends to cause the curved aorta to straighten slightly, thus pushing the heart forward.) o The apex beat can usually be felt by placing the Oat of the hand on the chest wall over the heart. o The apex beat is normally found In the fifth left intercostal space, 3.5 In. (9 cm) from the midline. Axillary folds Anterior axillary fold-forms the lower border of the pectoralis major muscle. Posterior axillary fold- forms the tendon of the latissimus dorsi muscle as It passes around the lower border of the teres major muscle. Posterior chest wall Spinous processes of the thoracic vertebrae can be palpated In the posterior midline. o The first spinous process to be felt is that of the seventh cervical vertebrae (vertebra prominens). - The overlapping spines of the thoracic vertebrae are below this level. Ligamentum nuchae- a large ligament. Covers the spines of the Cl to 6 vertebrae. It should be noted that the tip of a spinous process of a thoracic vertebra lies posterior to the body of the next vertebra below. Scapula (shoulder blade)- flat and triangular in shape and is located on the upper part of the posterior surface of the thorax. o Superior angle lies opposite the spine of the second thoracic vertebra. o Spine of the scapula is subcutaneous, and the root of the spine lies on a level with the spine of the third thoracic vertebra. o Inferior angles lies on a level with the spine of the seventh thoracic vertebra. Clinical notes As medical personnel, you will be examining the chest to detect evidence of disease. Your examination consists of Inspection, palpation, percussion, and auscultation. 1. Inspection shows the configuration of the chest. the range of respiratory movement, and any inequalities on the two sides.
- 16. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 16 2. Palpitation enables the clinician to confirm the Impressions gained by Inspection, especially of the respiratory movements of the chest wall. - Abnormal protuberances or recession of part of the chest wall ls noted. - Abnormal pulsations are felt and tender areas detected. 3. Percussions is a sharp tapping of the chest wall with the fingers. This produces vibrations that extend through the tissues of the thorax. 4. Auscultation enables the clinician to listen to the breath sounds as air enters and leaves the respiratory passages. - If the alveoli or bronchi are diseased and filled with fluid, the nature of the breath sounds will be altered. - The rate and rhythm of the heart can be confirmed by auscultation, and the various sounds produced by the heart and its valves during the different phases of the cardiac cycle can be heard. - Detecting friction sounds produced by the rubbing together of diseased layers of pleura or pericardium may be possible. Orientation lines • Midsternal line- lies in the median plane over the sternum. • Midclavicular line- runs vertically downward from the midpoint of the clavicle. • Anterior axillary line- runs vertically downward from the anterior axillary fold. • Posterior axillary line- runs vertically downward from the posterior axillary fold. • Midaxillary line-runs vertically downward from a point situated midway between the anterior and posterior axillary folds. • Scapular line- runs vertically downward on the posterior wall of the thorax, passing through the Inferior angle of the scapula (arms at the sides) Trachea - Extends from the lower border of the cricoid cartilage (opposite the body of the sixth cervical vertebra) In the neck to the level of the sternal angle In the thorax. - It commences In the midline and ends just to the right of the midline by dividing into the right and the left principal bronchi. - At the root of the neck, it may be palpated in the midline in the suprasternal notch. Lungs Apex of the lungs projects into the neck. - It can be mapped out on the anterior surface of the body by drawing a curved line, convex upward, from the sternoclavicular joint to a point 1 in. (2.5 cm) above the junction of the medial and intermediate thirds of the clavicle. Anterior border of the right lung begins behind the sternoclavicular joint and runs downward, almost reaching the midline behind the sternal angle. It then continues downward until it reaches the xiphisternal joint. Anterior border of the left lung has similar course, but at the level of the fourth costal cartilage, It deviates laterally and extends for a variable distance beyond the lateral margin of the sternum to form the cardiac notch. - The heart displacing the lung to the left produces this notch. - The anterior border then turns sharply downward to the level of the xiphisternal joint. Lower border of the lung in midinspiration follows a curving line, which crosses the sixth rib in the midclavicular line and the eighth rib in the midaxillary line, and reaches the 10th rib adjacent to the vertebral column posteriorly. - inferior border of the lung changes during inspiration and expiration.
- 17. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 17 Posterior border of the lung extends downward from the spinous process of the seventh cervical vertebra to the level of the 10th thoracic vertebra and lies about 1.5 In. (4 cm) from the midline. Oblique fissure of the lung can be indicated on the surface by a line drawn from the root of the spine of the scapula obliquely downward, laterally and anteriorly, following the course of the sixth rib to the sixth costochondral junction. Horizontal fissure- an additional fissure in the right lung only. - This fissure may be represented by a line drawn horizontally along the fourth costal cartilage to meet the oblique fissure in the midaxillary line. Pleura The boundaries of the pleural sac can be marked out as lines on the surface of the body. Lines of pleural reflection- the lines, which indicate the limits of the parietal pleura where it lies close to the body surface. Cervical pleura bulges upward into the neck and has a surface marking identical to that of the apex of the lung. - A curved line may be drawn, convex upward, from the sternoclavicular joint to a point 1 in. (2.S cm) above the Junction of the medial and intermediate thirds of the clavicle. Anterior border of the right pleura runs down behind the sternoclavicular joint, almost reaching the midline behind the sternal angle. It then continues downward until It reaches the xiphisternal joint. Anterior border of the left pleura has a similar course, but at the level of the fourth costal cartilage. it deviates laterally and extends to the lateral margin of the sternum to form the cardiac notch. (Note that the pleural cardiac notch is not as large as the cardiac notch of the lung.) It then turns sharply downward to the xiphisternal joint. Lower border of the pleura on both sides follows a curved line, which crosses the eighth rib In the midclavicular line and the 10th rib In the midaxillary line, and reaches the 12th rib adjacent to the vertebral column-that Is, at the lateral border of the erector spinae muscle Costodiaphragmatic recess- distance between two borders. Clinical notes Cervical dome of the pleura and the apex of the lungs extend up into the neck so that at their highest point, they Iie about 1 in. (2.5 cm) above the clavicle. Consequently, they are vulnerable to stab wounds ln the root of the neck or to damage by an anesthetist's needle during nerve block of the lower trunk: of the brachial plexus. Heart - both have apex and four borders. Apex- formed by the left ventricle, corresponds to the apex beat and is found in the fifth left intercostal space 3.5 in. (9 cm) from the midline. Superior border- formed by the roots of the great blood vessels, extends from a point on the second left costal cartilage (remember the sternal angle) 0.5 in. (1.3 cm) from the edge of the sternum to a point on the third right costal cartilage 0.5 in. (1.3 cm) from the edge of the sternum. Right border- formed by the right atrium, extends from a point on the third right costal cartilage 0.5 in. (I.3 cm) from the edge of the sternum downward to a point on the sixth right costal cartilage 0.5 in. (1.3 cm) from the edge of the sternum. Left border- formed by the left ventricle, extends from a point on the second left costal cartilage 0.5 in. (1.3 cm) from the edge of the sternum to the apex beat of the heart.
- 18. Thorax Part 1: Thoracic Wall 1st Semester | Prelims | Montezo, NJ. | DMD-2 Explorer 18 lnferior border- formed by the right ventricle and the apical part of the left ventricle, extends from the sixth right costal cartilage 0.5 in. (1.3 cm) from the sternum to the apex beat. Thoracic blood vessels o Arch of the aorta and the roots of the brachiocephalic and left common carotid arteries lie behind the manubrium sterni. o The superior vena cava and the terminal parts of the right and left brachiocephalic veins also lie behind the manubrium sterni. o Internal thoracic vessels run vertically downward, posterior to the costal cartilages, 0.5 in. (I.3 cm) lateral to the edge of the sternum o lntercostal vessel and nerve (“vein, artery, nerve"-VAN-is the order from above downward) are situated immediately below their corresponding ribs Mamillary Gland - lies in the superficial fascia covering the anterior chest wall. o It is rudimentary in children and in men. It enlarges and assumes its hemispherical shape in females after puberty.