
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Healing Of Extraction Wound.pdf
Similar to Healing Of Extraction Wound.pdf (20)
More from NASERALHAQ
More from NASERALHAQ (16)
Recently uploaded
Recently uploaded (20)
Healing Of Extraction Wound.pdf
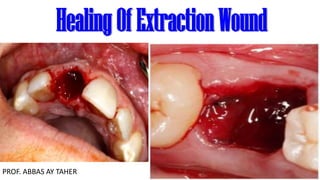
- 1. HealingOf ExtractionWound PROF. ABBAS AY TAHER
- 2. The healing of an extraction socket is a specialized example of healing by second intention. After tooth extraction, the wound goes through several stages of healing. Here are the typical stages of post-extraction wound healing: Hemostasis: Immediately after the tooth extraction, a blood clot forms in the socket. The blood clot helps control bleeding and serves as a foundation for the healing process. Inflammation: In the first few days following the extraction, inflammation occurs. The area around the socket may appear swollen, and you may experience some pain or discomfort. The body's immune response is triggered, sending white blood cells to the area to fight off infection and initiate the healing process.
- 3. Granulation tissue formation: Within a week or so, granulation tissue begins to develop at the base of the socket. This tissue contains new blood vessels and connective tissue, which is crucial for the subsequent stages of healing. Epithelialization: The granulation tissue is gradually replaced by epithelial cells, which grow over the socket from the surrounding tissue. This process helps to cover the wound and protect it from external factors. Wound contraction: Over time, the wound contracts as the surrounding tissue pulls together, reducing the size of the socket. This helps to close the wound and fill the gap left by the extracted tooth. Remodeling: In the final stage of healing, the newly formed tissue undergoes remodeling. The socket continues to fill in with new bone, gradually restoring the area where the tooth was removed.
- 4. Timing of the healing process: By 1st week The clot forms a temporary scaffold upon which inflammatory cells migrate. Epithelium at the wound periphery grows over the surface of the organizing clot. Osteoclasts accumulate along the alveolar bone crest setting the stage for active crestal resorption. Angiogenesis proceeds in the remnants of the periodontal ligaments. By 2nd Week The clot continues to get organized through fibroplasia and new blood vessels that begin to penetratetowards the center of the clot. Trabeculae of osteoid slowly extend into the clot from the alveolus, and osteoclastic resorption of the cortical margin of the alveolar socket is more distinct. By 3rd Week The extraction socket is filled with granulation tissue and poorly calcified bone forms at the wound perimeter. The surface of the wound is completely re-epithelialized with minimal or no scar formation. Active bone remodeling by deposition and resorption continues for several more weeks. Radiographic evidence of bone formation does not become apparent until the sixth to eighth weeks following tooth extraction. Due to the ongoing process of bone remodeling the final healing product of the extraction site may not be discernible on radiographs after 4 to 6 months.
- 5. It's important to note that individual healing times can vary depending on factors such as the complexity of the extraction, the overall health of the individual, and adherence to post-operative care instructions. Factors affecting the post extraction healing : Several factors can influence the healing process after tooth extraction. Here are some of the key factors that can affect post-extraction wound healing: Surgical technique: The technique used during the extraction procedure can impact healing. Atraumatic extraction techniques that minimize trauma to surrounding tissues tend to promote faster and smoother healing. Oral hygiene: Maintaining good oral hygiene is crucial for proper healing. Failure to keep the extraction site clean can increase the risk of infection and delay healing. Following your dentist's instructions for post-operative care, including proper brushing and rinsing techniques, is important.
- 6. Medications and medical conditions: Certain medications, such as anticoagulants or anti-inflammatory drugs, can affect the healing process. Medical conditions like bleeding disorders or compromised immune systems can interfere with proper healing. Tooth location and complexity: The location and complexity of the extracted tooth can influence healing. Wisdom teeth extractions or surgical extractions that involve more extensive bone removal may require additional healing time compared to simple extractions. Post-operative care: Following post-operative instructions given by the dentist or oral surgeon is essential for optimal healing. This includes avoiding certain activities like vigorous rinsing, drinking through a straw, or consuming hard or chewy foods that can disrupt the healing process.
- 7. Patient's overall health: General health plays a significant role in the healing process. Conditions such as diabetes, immune disorders, and nutritional deficiencies can impede healing. Certain medications, such as immunosuppressants or anticoagulants, may also affect the healing process. Smoking: Smoking has a negative impact on wound healing, including after tooth extraction. Smoking decreases blood flow to the tissues, reduces oxygen supply, and impairs the immune response, all of which can slow down healing and increase the risk of complications. Infection and inflammation: Infections at the extraction site can hinder healing. Pre-existing infections or inadequate post-operative care can contribute to inflammation and delay the healing process. Proper oral hygiene, antibiotic use (if prescribed), and following post-operative instructions help minimize the risk of infection.
- 8. Post-extraction socket preservation: Socket preservation is a technique defined as alveolar ridge preservation within the bone envelope remaining after tooth extraction with the purpose of reducing bone resorption in order to perform a correct implant-supported prosthesis, or proper fitted dentures or fix prostheses Here are some commonly used methods of post- extraction socket preservation: Ridge preservation with bone grafting: This involves placing a bone graft material into the socket after the tooth extraction. The graft material can be synthetic or derived from the patient's own bone or from a donor source. This method helps to maintain the volume and contours of the alveolar ridge.
- 9. Guided bone regeneration (GBR): GBR involves using a barrier membrane to cover the socket and promote bone regeneration. The membrane prevents soft tissue ingrowth while allowing the bone to grow into the socket. A bone graft material may also be used in conjunction with the membrane. Socket seal: After the tooth extraction, the socket is covered with a resorbable or non-resorbable membrane or collagen plug to create a seal. This helps to protect the socket from bacterial invasion and promotes blood clot formation, which is crucial for proper healing. Platelet-rich fibrin (PRF): PRF is a technique that involves collecting and processing the patient's own blood to obtain a concentrated solution of platelets and growth factors. This solution is then placed in the socket after extraction to enhance healing and promote bone regeneration.
- 10. Problems of Residual ridge resorption
- 11. Alveolar bone is defined as the bony portion of the maxilla and the mandible in which roots of the teeth are held by fibers of periodontal ligament Residual alveolar ridge ( is that portion of the alveolar ridge and its soft tissue covering which remains following the removal or loss of teeth. We don’t come across the ideal ridge in complete denture patients. 7 out of 10 completely edentulous patients have resorbed mandibular ridge. So you need to understand the residual ridge resorption.
- 12. ◼ The residual ridge resorption (RRR)is a life-long process. ◼ The rate of reduction in size of the residual ridge is maximum in the first 3-6 months and then gradually tapers off. Coupled process between: 1. Bone deposition by osteoblasts 2. Bone resorption by osteoclasts 5-7% of bone mass recycled weekly All spongy bone replaced every 3-4 years. All compact bone replaced every 10 years. To prevent mineral salts from crystallizing; protect against brittle bones and fractures
- 13. The rate of RRR varies, from one individual to another; at different phases of life and even at different sites in the same person. The clinical significance of such remodeling is that the functionality of removable prostheses, which rely greatly on the quantity and architecture of the residual ridge, may be adversely affected. Based on Bone Height (Mandible only) ◼ Type I : Residual bone height of 21 mm or greater measured at the least vertical height of the mandible. ◼ Type II : Residual bone height of 16 - 20 mm measured at least vertical height of the mandible. ◼ Type III : Residual alveolar bone height of 11 - 15 mm measured at the least vertical height of the mandible. ◼ Type IV : Residual vertical bone height of 10 mm or less measured at the least vertical height of the mandible.
- 14. Consequences of Residual Ridge Resorption: The following consequences provide a serious problem to clinicians on how to provide adequate support, stability, and retention of the denture. 1. Apparent loss of sulcus width and depth 2. Displacement of the muscle attachment closer to the crest of the residual ridge. 3. Loss of vertical dimension of occlusion. 4. Reduction of lower face height. 5. Anterior rotation of the mandible. 6. Increase in relative prognathism. 7. Changes in inter-alveolar ridge relationship. 8. Morphological changes such as sharp, spiny, uneven residual ridges. 9. Location of the mental foramina close to the crest of the mandibular residual ridge. 10. Resorption of the mandibular canal wall and exposure of the mandibular nerve.
- 15. RRR occurs worldwide in Males and females ,Young and old, Sickness and health, With or without dentures, Unrelated to primary reason for the extraction of teeth ( caries & pdl disease ) Studies also suggest incresed knife edge tendency in mandibular residual ridge in women compared to men. RRR is accelerated in the first 6 months with more loss in mandible than maxilla. According to Boucher, ➢ During the first year after tooth extraction, the reduction in residual ridge height in the midsagittal plane is 2-3 mm for maxilla 4-5 mm for mandible ➢ Annual rate of reduction in height 0.1-0.2 mm for mandible 4 times less in the maxilla
- 16. The direction of bone resorption: Maxilla resorbs upward and inward to become progressively smaller because of the direction and inclination of the roots of the teeth and the alveolar process. The opposite is true of the mandible, which inclines outward and becomes progressively wider according to its edentulous age. This progressive change of the edentulous mandible and maxilla makes many patients appear prognathic RRR is generally more in mandible than in maxilla and but the reverse may also occur…. So one must treat the “PARTICULAR PATIENT, NOT THE AVERAGE PATIENT
- 17. Atwood classified residual ridge resorption into: Order 1: pre-extraction Order 2: post-extraction Order 3: high, well-rounded Order 4: knife-edged Order 5: low, well rounded Order 6: depressed There is a reduction in the size of the residual ridge. Residual ridge resorption is a localized loss of bone structure. To categorize the most common residual ridge configurations, Atwood has described the six orders of residual ridge resorption. But there may be porosities and imperfections in the crestal areas of residual ridges of both maxilla and mandible, no matter at what stage of configuration they are. Residual ridge resorption does not stop with the residual ridge. This ridge resorption can continue till only a thin cortical plate is left on the inferior border of the mandible, and in maxilla, it continues till there is no alveolar process left. Lateral cephalometric radiographs provide an accurate method for determining RRR.
- 18. ◼ Acc. to Atwood…..RRR is a multifactorial biomechanical disease caused by a combination of :Anatomic factors ,Mechanical factors ,and Metabolic factors 1-Anatomic factors It is postulated that RRR varies with the quantity and quality of the bone of residual ridges.. i.e. the more bone there is, the more RRR will ultimately be. 2.Metabolic factors RRR varies directly with certain systemic or localized bone resorptive factors and inversely with certain bone formation factors. RRR Bone resorption factors Bone formation factors Residual ridge resorption (RRR)is directly proportional to bone resorption factors/bone formation factors. Bone formation factors are local and syustemic Local bone-resorbing factors like endotoxins, osteoclast activating factor (OAF), prostaglandins, human gingival bone- resorption stimulating factor, heparin and trauma lead to residual ridge resorption. Bone forming factors are circulating estrogen, thyroxine, growth hormone, androgens, calcium, phosphorus, vitamin D, protein and fluoride.
- 19. ◼ Force is the main factor in Residual ridge resorption. Residual ridge resorption is directly proportional to force. ◼ Bone that is used by regular and physical activity will tend to strengthen within certain limits, then the bone that is in “disuse atrophy”, while others postulated that due to denture wearing It is caused due to an “abuse” bone resorption. ◼ While considering force, one must also consider: Amount of force, Frequency of force Duration of force, Direction of force ,Force per unit area ◼ Perhaps there is truth in both hypotheses. ◼ The fact is that with or without dentures some patients have little or no RRR and some have severe RRR. ◼ Mechanical factors ◼ Also, force applied to the bone is affected inversely by the damping effect of the underlying tissue. The damping effect is energy absorption in the mucoperiosteum.
- 20. Treatment and prevention Treatment of RRR is ideally by preventing it. 1-Prevention of loss of natural teeth 2-Change in design of the denture 3-Impression procedures 4-Minimal pressure impression technique. 5-Selective pressure impression technique: places stress on those areas that best resist functional forces 6-Adequate relief of non-stress bearing areas eg. Crest of the mandibular ridge. 7-The broad area of coverage helps in reducing the force /unit area (Snow Shoe Effect) 8-Avoidance of inclined planes to minimize dislodgment of dentures and shear forces. 9-Centralization of occlusal contacts to increase stability and maximize compressive forces. 10-Provision of adequate tongue room to improve stability of denture in speech and mastication. 11-Adequate interocclusal distance during jaw rest to decrease the frequency and duration of tooth contact. 12-Occlusal table should be narrow 13-Diet counseling for prosthodontic patients is necessary to correct imbalances in nutrient intake.
- 21. 14-Denture patients with excessive RRR report lower calcium intake and poorer calcium phosphorus ratio, along with less vitamin D.
- 22. Excessive RRR leads to loss of sulcus width and depth with a displacement of muscle attachment more to the crest of the residual ridge, osseous reconstruction surgeries, removal of high frenal attachments, augmentation procedures, vestibuloplasties etc may be required to correct these conditions.
- 23. Immediate dentures: Some authors claim that extraction followed by immediate dentures reduces the ridge resorption but this has still to be proved. Overdenture: tooth or implant supported 1.The denture bearing mucosa of the residual ridges are spared abuse. 2.Maintenance of the alveolar bone 3.Sensory feedback 4.Minimal load thresholds 5.Tactile sensitivity discrimination 6.Masticatory performance 7.Reduction of Psychological trauma
- 24. Thank you