
Recommended
More Related Content
Similar to Pulmonary unit
Similar to Pulmonary unit (20)
More from UVAS
More from UVAS (20)
Recently uploaded
Recently uploaded (20)
Pulmonary unit
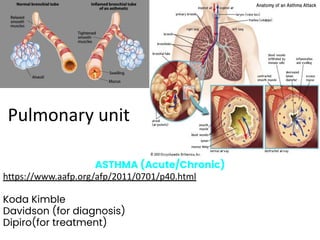
- 1. Pulmonary unit ASTHMA (Acute/Chronic) https://www.aafp.org/afp/2011/0701/p40.html Koda Kimble Davidson (for diagnosis) Dipiro(for treatment)
- 2. Introduction Chronic inflammatory disorder of the airways. – Wheezing, breathlessness, chest tightness, and cough. – Particularly at night & in the early morning. – Airflow obstruction is often reversible. ■ Co-existing symptoms of Fever,LOA, LOW,Ankle swelling,Palpitations. • Aspirin can cause asthma through the production of cysteinyl leukotrienes. • Cells that play a role are: – Mast cells. – Eosinophils, – T lymphocytes. – Neutrophils. – Epithelial cells. 1997 NIH guidelines
- 3. Etiology Childhood-onset asthma Associated with atopy. Genetic predisposition for the development of immunoglobulin E (IgE)-mediated response to common aeroallergens. positive family history of asthma and allergy to tree and grass pollen, house dust mites, household pets, and molds. Adult-onset asthma Many adults with asthma have a negative family history and negative skin tests. Patients may have nasal polyps, aspirin sensitivity, and sinusitis. Exposure to factors (e.g.,wood dusts, chemicals) at the workplace. factors include viral infections,diet, exposure to tobacco smoke, and environmental pollutants.
- 6. Pathophysiology Inflammatory cells and mediators. Mast cells, eosinophils, T lymphocytes, neutrophils,epithelial Cells. Bronchial epithelium in asthmatics is fragile, with various abnormalities including destruction of ciliated cells. After exposure to an asthma-precipitating factor (e.g., aeroallergen), inflammatory mediators are released from bronchial mast cells, macrophages, T lymphocytes, and epithelial cells. These mediators causes activation of other inflammatory cells, most notably eosinophils. Eosinophils cause airway injury, including epithelial damage, mucus hypersecretion, and increased reactivity of smooth muscle Cytokines (e.g., interleukin [IL]-4 and IL-5) TH2 lymphocytes release cytokines. at least 27 cytokines may have a role in the pathophysiology of asthma. Exhaled nitric oxide (NO), biomarker of airway inflammation. Bronchial NO has been found to be elevated during periods of exacerbations. decreased with administration of inhaled steroids but not β2-agonists. Airway remodeling refers to structural changes, including an alteration in the amount and composition of the extracellular matrix leading to airflow obstruction. long-term airway inflammation in asthma may result in airway remodeling
- 8. Hyper-reactivity defined as an exaggerated response of bronchial smooth muscles to trigger stimuli Examples of these stimuli include inhaled allergens, respiratory viral infection, cold, dry air, smoke, other pollutants. Endogenous Stimuli includes poorly controlled rhinitis, sinusitis, and gastroesophageal reflux disease. Premenstrual asthma has been reported, but the exact hormonal mechanism is not known. Characterized by periods of remissions and exacerbations. Inflammation appears to be the primary process in the pathogenesis of bronchial hyperreactivity Symptoms of Asthma Clinical presentation. intermittent episodes of expiratory wheezing, coughing, and dyspnea. chest tightness or a chronic cough that is not associated with wheezing. Symptoms may be precipitated by: ● Exercise. ● Cold weather. ● Allergen exposure (e.g. pets, occupational). ● Viral respiratory tract infections. ● Drugs (β-blockers, aspirin and NSAIDs).
- 9. Breathlessness ■ Most common symptom. ■ Severity? ■ Walk how far? ■ Climb stairs how many flights? ■ Effect on his job, social activity? ■ Timing of breathlessness? Cough ■ Duration ■ When ■ Persistent or intermittent ■ Pain? ■ Dry or wet
- 10. Classifications of Severity of an Asthma Exacerbation DEGREE OF SEVERITY SYMPTOMS AND SIGNS INITIAL PEF (OR FEV1 ) CLINICAL COURSE Mild Dyspnea only with activity PEF ≥ 70 percent Usually treated at home. Prompt relief with inhaled short-acting beta2 agonist Possible short course of oral systemic corticosteroids. Moderate Dyspnea interferes with or limits usual activity PEF 40 to 69 percent Usually requires office or emergency department visit. Relief from frequent inhaled short-acting beta2 agonist Oral systemic corticosteroids; some symptoms last for one to two days after treatment begins Severe Dyspnea at rest; interferes with conversation PEF < 40 percent Usually requires emergency department visit and likely hospitalization. Partial relief from frequent inhaled short-acting beta2 agonist Oral systemic corticosteroids; some symptoms last for more than three days after treatment begins Adjunctive therapies are helpful life threatening Too dyspneic to speak; perspiration PEF < 25 percent Requires emergency department visit/hospitalization; possible intensive care unit. Minimal or no relief from frequent inhaled short-acting beta2 agonist & Intravenous corticosteroids
- 11. Physical examinations ■ General appearance ■ Cyanosis ■ Finger clubbing ■ Head and neck ■ Chest inspection ■ Chest palpation
- 12. Full systemic enquiry ■ Past medical history ■ Family history ■ Social history ■ Current medications ■ Allergies
- 13. Diagnosis and Monitoring History Detailed history of symptoms of wheezing, chest tightness, shortness of breath, and coughing. Episodes may worsen seasonally. History of nocturnal symptoms with awakening in the early morning is a critical component to assess. History of symptoms after exposure to other common triggers (e.g., cats, perfume, second-hand tobacco smoke). A positive family history, presence of rhinitis or atopic dermatitis also are significant. Skin testing Useful in identifying triggering allergens. Pulmonary Function Tests SPIROMETRY: Performed when clinically stable. Lung volumes often are measured to obtain information about the size of the patient’s lungs.. lung volumes depend on age, race, gender, height,weight. can affect the volume of air that can be inhaled and exhaled. Tidal volume: volume of air inspired or expired during normal breathing. Vital capacity (VC): volume of air blown off after maximal inspiration to full expiration. Patients with obstructive lung disease have a decreased VC. Residual volume (RV):volume of air left in the lung after maximal expiration. Patients with obstructive lung disease have increased RV. Functional residual capacity (FRC):volume of air left after a normal expiration. Patients with obstructive lung disease have a normal TLC. Total lung capacity (TLC): VC plus the RV.
- 14. Spirometer Used to evaluate the performance of the patient’s lungs, thorax, and respiratory muscles in moving air into and out of the lungs. FEV. Measured by having the patient exhale into the spirometer as forcefully and as possible after maximal inspiration. The resulting volume curve is plotted against time so that expiratory flow can be estimated. FEV1 Gas exchanged in one second by a forced expiration. The FEV1 usually is expressed as a percentage of the total volume of air exhaled and is reported as the FEV1 to FVC ratio. Healthy persons generally can exhale at least 75% to 80% of their VC in 1 second. PEAK EXPIRATORY FLOW Maximal flow that can be produced during the forced expiration. A healthy, average sized young adult male typically has a PEF of 550 to 700 L/minute. Blood Gas Measurements ABGs (i.e., PaO2, PaCO2, and pH). ABG measurements also are dependent on the patient’s cardiovascular Status. Another measure oxygen saturation is the ratio between the actual amount of oxygen bound to hemoglobin and the potential amount of oxygen that could be bound to hemoglobin at a given pressure.
- 16. Guidelines • National Institutes of Health, National Heart, Lung, and Blood Institute. National Asthma Education and Prevention Program. Full Report of the Expert Panel: Guidelines for the Diagnosis and Management of Asthma (EPR-http://www.nhlbi.nih.gov/guidelines/asthma. • British guideline on the management of asthma
- 17. Immediate assessment of acute severe asthma Acute severe asthma PEF 33–50% predicted (< 200 L/min) Inability to complete sentences in 1 breath Heart rate ≥ 110/min Respiratory rate ≥ 25/min Life-threatening features PEF < 33% predicted (< 100 L/min) SpO2 < 92% or PaO2 < 8 kPa (60 mmHg) Normal or raised PaCO2 Silent chest/feeble respiratory effort Cyanosis Hypotension Exhaustion Confusion Coma Bradycardia or arrhythmias Near-fatal asthma ↑PaCO2 and/or requiring mechanical ventilation with raised inflation pressures
- 19. Sample Questionsa for the Diagnosis and Initial Assessment of Asthma
- 20. Obstructive versus Restrictive Airway Disease restrictive disease obstructive disease limits airflow during inspiration, results from a loss of elasticity (e.g., fibrosis, pneumonia) or physical deformities of the chest (e.g., kyphoscoliosis). limit lung expansion. limits airflow during expiration. Narrow air passages, create air turbulence, and increase resistance to airflow. Expiratory flow is depressed.
- 21. Goals of Therapy Reduce Impairment Prevent chronic/troublesome symptoms. maintain “normal” pulmonary function. require infrequent use of SABA. meet patients’ and families’ expectations of and satisfaction. Reduce Risk: Prevent recurrent exacerbations of asthma. minimize the need for ED visits/hospitalizations. Prevent progressive loss of lung function. Provide optimal pharmacotherapy with minimal or no adverse effects. Long-Term Management Measures of asthma assessment and monitoring. Education for a partnership in asthma care. Control of environmental factors/comorbid conditions that affect asthma. Medications.
- 22. TREATMENT/Aerosol • The drug is either in solution or a suspended micronized powder. • Inhalation of SABA provides rapid bronchodilation. • Inhaled corticosteroids (ICSs) enhance lung activity. • Specific agents (cromolyn, formoterol, salmeterol,ipratropium bromide) are only effective by inhalation. Device Determinants of Delivery Jet nebulizers nebulizers can deliver 2% to 15% of the actuated dose Ultrasonic nebulizers metereddose inhalers (MDIs) MDIs can deliver 15% to 50% of the actuated dose. dry powder inhalers (DPIs) DPIs can deliver 10% to 30%of the actuated dose. TABLE 15-4 Factors Determining Lung Deposition of Aerosols(DIPIRO)S. Instructions for inhaler use: http://www.nhlbi.nih.gov/guidelines/archives/epr-2/index.htm.
- 23. Drugs Used in Acute Asthma β2- Agonists SABA Page (912-913 Dipiro) SABA..most effective . 1st choice…management of ASA. Frequent administration every 20 min or continuous neb. continuous neb recommended for patients having an unsatisfactory response. Dose for children often is listed on a weight basis. Adults have fixed maximal doses. clinical trials.. equal/greater efficacy/greater safety of aerosolized β2- agonists . Systemic adverse effects…systemic β2-agonist therapy. Children younger than 2 yrs…significant responses from neb albuterol. mechanical ventilator circuits (infants, children, and adults in respiratory failure). Continuous vs intermittent (hourly) neb albuterol. Cortico- steroids (Page 913 Dipiro) Systemic corticosteroids indicated in all patients with AA. Therapy continued until hospital discharge. Tapering the IV cs dose for outpatient therapy. 3- to 10-day courses of oral prednisone…..effective. High-dose.. higher side effects IV therapy..no advantage over oral administration. patients achieve normal FEV1 within 48 hours. maintaining IV cs for 10-14 days may be unnecessarily. Multiple daily dosing of systemic corticosteroids VS OD.
- 24. Anticholinergics Page 914 Dipiro. Inhaled ipratropium bromide. multiple-dose.. Initial therapy reduces hospitalization rate. ipratropium bromide in the eyes may produce pupillary dilation. Use tight mask or mouthpiece Ipratropium bromide poorly absorbed and produces minimal/no systemic effects. administering ipratropium bromide by nebulizer…Care should be taken. Ipratropium bromide is not a vasodilator unlike β2-agonists. Alternative Therapies Page 914 Dipiro Aminophylline: increase the risk of ADR ED use of aminophylline.. not been Recommended. does not enhance improvement in lung function. Magnesium sulfate: potent bronchodilator. relaxation of smooth muscle. CNS depression. IV magnesium sulfate use in ED is controversial. Helium given as a mixture of helium and O2 (heliox) can lower resistance to gas flow. increase ventilation. Others inhalational anesthetics. volatile anesthetics…not recommended Ketamine…. recommended
- 25. Drug Class Information/Acute Asthma SABA TABLE 15-8 Page 917 Dipiro Effective bronchodilators. as-needed treatment of intermittent episodes of bronchospasm. produces smooth muscle relaxation, mast cell membrane stabilization, and skeletal muscle stimulation. Enhances insulin secretion,decrease in serum K concentration. β1-receptor stimulation produces excessive cardiac stimulation(cardiac arrhythmias). Catecholamines have a shorter duration of action. Aerosol administration of the SABA provides more rapid response. intensity and duration of response are dose dependent. Chronic administration of β2-agonists leads to downregulation. Systemic Cortico- steroids Table 15-9 Page 918 Dipiro Most effective anti-inflammatories. 1 to 2 weeks -----1 to 2 mg/kg/day of prednisone. reduces mucus production and airway edema. 4 to 12 hours may be required before any clinical response is noted. Chronic use of corticosteroids does not induce corticosteroid Dependence. Effects and side effects are dose and duration dependent. short bursts (≤10 days)…corticosteroid side effects occur.
- 26. Anticholinergics do not have an FDA-labeled indication for asthma. competitive inhibitors of muscarinic receptors. they reverse cholinergic-mediated bronchoconstriction. Ipratropium bromide, Tiotropium bromide,, not as effective as β2-agonists. intensity and duration of action are dose dependent. Ipratropium bromide is only indicated as adjunctive therapy in acute severe asthma EVALUATION OF THERAPEUTIC OUTCOMES(Figures 15-6 and 15-7 Page 922 Dipiro) Frequency of monitoring depends on the severity of the exacerbation. Lung function(spirometric or peak flow measurements-5 to 10 minutes after each Treatment) O2 saturations Patients not achieving an initial response should be monitored every 0.5 to 1 hour. decision to admit to the hospital should be made within 4 to 6 hours of entry to the ED. duration of hospitalization following admission is 2 to 3 days.
- 27. TREATMENT/Acute Severe Asthma primary goal…. prevention of life-threatening asthma,Correction of significant hypoxemia,Rapid reversal of airflow obstruction,Reduction of the likelihood of relapse. Development of a written asthma action plan in case of a further exacerbation. Goals are best achieved by early initiation of treatment and close monitoring of objective measures. Physical examination should be obtained while initial therapy is being provided. Predictor of outcome Improvement in FEV1 at 30 minutes following inhaled β2-agonists. O2 supplementation To maintain O2 saturations above 90% (0.90) (or >95% [0.95] in pregnant women and those who have coexistent heart disease. Pharmacologic Treatment short-acting inhaled β2-agonists (SABA) depending on the severity, systemic corticosteroids, inhaled ipratropium, and O2. (Figs. 15-6 and 15-7). Risk factors history of previous severe asthma exacerbations. Comorbidities. use of more than two canisters per month of short-acting inhaled β2-agonists. current intake of oral corticosteroids. TABLE 15-6 Dosages of Drugs of Acute Severe Exacerbations of Asthma in the Emergency Department or Hospital (Dipiro)
- 28. Home Management/ Acute Asthma
- 30. Cont/Acute Asthma Investigation Complete blood count(if fever or purulent sputum),Modest leukocytosis common in asthma. Chest radiography not recommended for routine assessment. Serum electrolytes (potassium, magnesium, and phosphate)should be monitored if high-dose continuous inhaled or systemic β2-agonists are to be used/in patients who take diuretics regularly/in patients with cardiovascular disease. can produce transient decreases in potassium, magnesium, and phosphate. excessive elevations of glucose and lactic acid may result from combination of high-dose β2-agonists & systemic corticosteroids. Response to Therapy. Should be significant improvement within the first 30 to 60 minutes of therapy. In Hospitalized patients 20% improvement is seen within the first 2 hours. Hypoxemia is correctable by low-flow O2. reversal of lung function may take 12 to 24 hours. complete restoration takes up to 3 to 7 days. Counseling points Provide the patient with a written self-management action plan. Should be taught how to use a peak flow meter and monitor morning peak flows at home. Signs of severe obstruction in children are increased RR, increased HR,inability to speak more than 1 or 2 words between breaths. O2 saturations should be measured in all patients not responding to initial therapy. On admission, the peak flows or clinical symptoms should be monitored every 2 to 4 hours. Prior to discharge from the ED or hospital, the patient should be given a sufficient supply of prednisone, taught purpose of the medications,proper inhaler technique. referred to followup asthma care within 1 to 4 weeks. Key to Successful Treatment Early recognition of deterioration/Easy access by telephone to healthcare providers. aggressive treatment/availability of oral prednisone to begin at home/ patient and/or parent education. teaching self management skills/written action plans/
- 31. Treatment/Chronic Asthma Diagnosis challenge testing with exercise, histamine, methacholine, or mannitol can be used. Serum IgE and sputum and blood eosinophil determinations. Very high peripheral blood eosinophil counts ……allergic bronchopulmonaryaspergillosis. Skin testing for identifying triggers. Hyperinflation… chest roentgenogram. Pharmacologic Therapy (Table 15-12) Page 927 Dipiro ICSs are considered the preferred long-term control therapy for persistent asthma. Low- to medium-dose ICSs improve lung function, and reduce severe exacerbations. more effective than cromolyn, theophylline. reduces the risk of dying from asthma. safe for long-term administration. Dose (TABLE 15-12 page 928 Dipiro) ICS and LABA: For those patients inadequately controlled on low-dose ICSs. either an increased dose of the ICS. Or combination of ICS and LABA. Alternatives could be theophylline to ICSs. combination of ICS/LABA more effective than doubling ICS dose. high doses ICSs plus LABA reserved for patients with severe persistent asthma
- 32. Drug Class Information/Chronic Asthma Inhaled Corticosteroids Details (Table 15-13) Page 931 Dipiro high topical potency to reduce inflammation. Low systemic activity. Different devices may result in twofold differences in delivery. delivery method make a significant difference. beclomethasone dipropionate, budesonide, ciclesonide, flunisolide, fluticasone propionate, and mometasone furoate. systemic clearance of the available ICSs is very rapid. all undergo extensive first-pass metabolism. Mouth rinsing and spitting will also reduce the oral availability ICSs produce dose-dependent systemic effects. Symptoms improve in the first 1 to 2 weeks of therapy. will reach maximum improvement in 4 to 8 weeks. ADR from ICSs include oropharyngeal candidiasis and dysphonia that are dose dependent. spacer device with MDIs can decrease oropharyngeal deposition. twice-daily dosing of most ICSs. Milder asthma, once-daily dosing is often sufficient Long-Acting Inhaled β2-Agonists LABA (Page 933 Dipiro) LABAs are recommended for chronic therapy only in combination with ICSs (formoterol and salmeterol) provide long-lasting bronchodilation. LABAs has not yet been approved for asthma. LABAs will produce dose-dependent systemic β2-agonist effects. formoterol has a more rapid onset of action. LABAs should not be used as monotherapy for asthma.
- 33. Contd-LAB A in children 12 years and older…. LABAs are preferred adjunctive therapy to ICSs. Combination treatment with ICS/LABA provides greater asthma control. LABAs should not be used as monotherapy for asthma. an increased risk for severe, life-threatening exacerbations and asthma-related death with LABA monotherapy. tolerance is produced with chronic administration of LABAs. Methyl-xa nthines high risk of severe life-threatening toxicity and numerous drug interactions. Theophylline…moderately potent bronchodilator with mild anti-inflammatory properties. Sustained release product is the preferred oral preparation. Toxicities include nausea, vomiting, tachycardia, jitteriness, and difficulty sleeping ,cardiac tachyarrythmias and seizures. Routine monitoring of serum concentrations is essential for the safe and effective use. Theophylline clearance is age dependent. The addition of theophylline to ICSs is similar to doubling the dose of the ICS. overall less effective than the LABAs as adjunctive therapy Cromolyn Na mast cell stabilizer and inhibits/only effective by inhalation, inhibits neurally mediated bronchoconstriction, it does not have bronchodilatory effect. intensity and duration of protection against various challenges are dose dependent. Cromolyn is no more or less effective than theophylline. not as effective as the ICSs for controlling persistent asthma. patients will experience an improvement in 1 to 2 weeks. initially should receive cromolyn four times daily, and then only after stabilization of symptoms may the frequency be reduced to three times daily.
- 35. Leukotriene Modifiers zafirlukast and montelukast, zileuton. they reduce allergen-, exercise-, cold-air hyperventilation–, irritant-, and aspirin-induced asthma. not preferred alternatives in mild persistent asthma nor as alternative add-on therapy for moderate persistent asthma. improve pulmonary function tests, decrease nocturnal awakenings and β2-agonist use, and improve asthma symptoms. Effective orally, and can be administered once or twice a day. less effective in asthma than low doses of ICSs. not as effective as LABAs when added to ICSs for moderate persistent asthma. there is some evidence that patients with aspirin-sensitive asthma do well. also have modest efficacy in allergic rhinitis. idiosyncratic syndrome has been reported in a small number of patients treated with zafirlukast and montelukast. Anti-IgE Omalizumab Page 938 Dipiro. recombinant anti-IgE antibody. for the treatment of allergic asthma administered subcutaneously. Doses range from 150 to 375 mg and are given at either 2- or 4-week intervals. approved for patients greater than 12 years. Other options Miscellaneous Therapies (Immunomodulators) Future Therapies.