
Recommended
More Related Content
What's hot
Viewers also liked
Similar to Oregon DMV Change of Gender Form
Similar to Oregon DMV Change of Gender Form (20)
Recently uploaded
Recently uploaded (20)
Oregon DMV Change of Gender Form
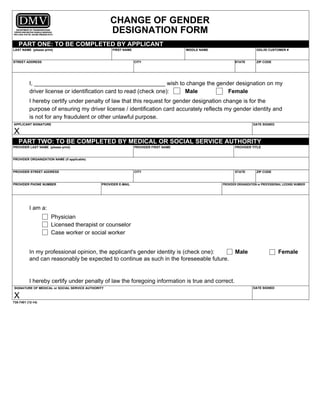
- 1. CHANGE OF GENDER DESIGNATION FORM PROVIDER ORGANIZATION NAME (if applicable) PROVIDER ORGANIZATION or PROFESSIONAL LICENSE NUMBERPROVIDER E-MAILPROVIDER PHONE NUMBER ZIP CODESTATECITYPROVIDER STREET ADDRESS PROVIDER TITLEPROVIDER FIRST NAMEPROVIDER LAST NAME (please print) PART TWO: TO BE COMPLETED BY MEDICAL OR SOCIAL SERVICE AUTHORITY PART ONE: TO BE COMPLETED BY APPLICANT LAST NAME (please print) FIRST NAME MIDDLE NAME STREET ADDRESS CITY STATE ZIP CODE ODL/ID CUSTOMER # I, _________________________________________ wish to change the gender designation on my driver license or identification card to read (check one): Male Female I hereby certify under penalty of law that this request for gender designation change is for the purpose of ensuring my driver license / identification card accurately reflects my gender identity and is not for any fraudulent or other unlawful purpose. I am a: Physician Licensed therapist or counselor Case worker or social worker In my professional opinion, the applicant's gender identity is (check one): Male Female and can reasonably be expected to continue as such in the foreseeable future. I hereby certify under penalty of law the foregoing information is true and correct. SIGNATURE OF MEDICAL or SOCIAL SERVICE AUTHORITY DATE SIGNED X APPLICANT SIGNATURE X DATE SIGNED 735-7401 (12-14) Print Form Reset Form