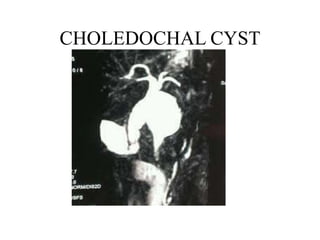
2. Choledochal cyst
• Focal or diffuse dilatation of biliary tree
• Common congenital abnormality of the biliary
tree
• Most common in Asia with incidence of 1 in
13000 population and common in japan with
an incidence of 1 in 1000
• 60% present in the first decade
• 25% present in adult
2
3. Alonso – LEJ/Todani classification
TYPE EXPLANATION
Type I
IA
IB
IC
Classic type, dilatation of CBD, most common 50-80%
Cystic
Fusiform
Saccular
Type II Simple diverticulum of the extrahepatic biliary tree, 2-3%
Type III Cystic dilatation of the intraduodenal portion of CBD, also called
choledochocele, <10%
Type IV
IV A
IV B
Involve multiple cysts of intra and extra-hepatic biliary tree
Both intra and extra-hepatic cysts, 30-40%
Multiple extra-hepatic cysts without intrahepatic involvement <5%
Type V Isolated intrahepatic biliary cystic disease, caroli’s disease, associated
periportal fibrosis or cirrhosis, can be multilobar or confined to single
lobe
3
5. Pathogenesis
• The cause is unknown. There are theories
proposed.
• Theory I – defect in maturation with ductal plate
malformation.
– Describe development of intrahepatic liver progenitor
cells that are in contact with the mesenchyme of portal
vein and are remodeled intomature ducts.
– Defective bile duct plate remodeling in embryogenesis
results in inflammation and ulceration forming larger
ducts
5
6. • Theory II
– Bile duct obstruction or distention in the prenatal
or neonatal period leading to cyst formation
– Obstruction may be secondary to stricture, web ,or
sphincter of Oddi dysfunction
– Pancreatic juice reflux into biliary tree causing
chronic inflammation and increased bile duct
pressure leading to cyst formation
– Animal models
6
7. • Theory III
– Most common proposed model for choledochal
cyst
– Related to pancreaticobiliary maljunction
– Defined as an extramural junction of pancreatic
and biliary duct in the duodenum beyond the
intramural sphincter function
– Characterised by long common channel.
– Significant risk for developing
cholangiocarcinoma
7
8. Pancreaticobiliary
maljunction
Long common channel
Pancreatic reflux and mixing
with bile
Mixed juice potentially
stagnates in bile tree/gall
bladder
Cycles of inflammation,
activation of proteolytic
enzymes, alteration in bile
composition
Damage to biliary tree
epithelium
Duct distention and may
progress to malignancy
8
9. Presentation
• Classic triad of jaundice, abdominal pain and
Rt upper quadrant mass in children
• Infants present with elevated conjugated
bilirubin(80%), failure to thrive or abdominal
mass(30%)
• Abdominal mass becomes less comman with
increasing age
9
10. • In adults – abdominal pain, recurrent cholangitis
are more common presentation
• Abdominal pain usually mimics that of calculous
cholecystitis and many individuals may have gall
stones in cyst or in the gall bladder
• May also present with intermittent jaundice, or as
pancreatitis(30%)
• 38% of adults will undergo cholecystectomy
before diagnosis of choledochal cyst.
• Rarely it may present as intraperitoneal rupture or
bleeding due to erosion into adjacent vessels.
10
11. Diagnosis
• Requires high suspicion
• Type I cyst may mimics biliary dilatation secondary to
obstruction, difference is elevated ALP in obstruction
• USG is most common first line imaging used in 93% of
pediatric and 72% of adults
• CT is appropriate in adults in whom the differential
diagnosis is broader
• Important consideration in CT is assessing the
hepatobiliary and pancreatic anatomy, with evaluation
of possible biliary malignancy, metastatic disease and
vascular encasement.
11
12. • When choledochal cyst is suspected –
visualisation of the pancreatic, extrahepatic
and intrahepatic ductal anatomy is required.
• MRCP is the non-invasive procedure of choice
• Many consider MRCP as the only imaging
required for diagnosis and operative planning.
• Cholangiography is considered gold standard,
can show areas of cystic dilatation, presence of
stone and exclude complete obstruction of bile
duct
12
13. Management
• Management of acute symptoms like
pancreatitis, cholangitis, improving general
condition followed by operative management
• Cholecystectomy + complete excision of the
cyst + bile duct reconstruction.
• Type I – complete cyst excision + Roux-en-Y
hepaticojejunostomy reconstruction
• Type II – complete cyst excision + CBD wall
defect closure with or without T-tube
13
14.
15. • Type III – primarily treated with ERCP +
endoscopic unroofing of the choledochoceles +
sphincterotomy is done
• Type IV – similar to type I , cholecystectomy +
complete cyst excision + biliary enteric
anastamosis
15
16. • Type V – caroli’s disease, begin with conservative
management by treating infection, complications
of drainage, stone extraction antibiotics and
ursodiol
• Single lobe – resection of the parenchyma
involved.
• Bilobar – ursodiol and antibiotics improve bile
flow, in the absence of complications Roux-en-Y
hepaticojejunostomy + b/l transhepatic silastic
stent
• Liver transplant
16