1. Cultural Humility vs. Cultural Competency:
An Approach to Health
Udit Bhavsar, Emily Dennis, Michael Guo, John Peterson
Faculty Advisor: Dr. Stephen C. Alder
Patient-Provider
Relationship
ACKNOWLEDGEMENTS
Conclusion
Faculty, staff, and students from the following:
•The Honors College (University of Utah)
•University of Utah Division of Public Health (Department of Family and
Preventative Medicine)
•Global Health Scholars (The Honors College)
Abstract Patients’ Anecdotes
In our current health care
paradigm, the physician acts on the
patient in an effort to improve their
health. Using prescriptions, procedures,
and protocols, the provider does all they
can to make the individual “better.”
However, this perspective is hurting the
patient's health and blinding the provider
to the actual needs of their patient.
Health care is not a service, but a
shared endeavor where both the one
providing and the one receiving the care
work together toward a healthy solution.
This new mindset promotes a focus on
lifelong learning rather than following
protocol (. It also highlights the important
role of listening and asking questions in
building a relationship between the
provider and receiver. Using these tools,
the provider and receiver work toward a
collaborative and sustainable health
solution. Our objective is persuading
health professionals to stop working on
their patients and begin working with
their patients toward health.
For example, one African-American patient who had
been diagnosed with diabetes reported a very negative
experience. While writing a prescription, the doctor told
her, “I need to write this prescription for these pills, but
you’ll never take them and you’ll come back and tell
me you’re eating pig’s feet and everything...” (unequal
treatment 2 copy)
A nurse who was treating a Latina patient who had left
surgery several hours before disregarded the patient’s
moans of pain because she “knew” from her cross-
cultural medicine course in nursing school that Latino
patients tend to exaggerate their pain
Cultural Humility
Problems with System
• Medical school curricula focus on
dispensing information about different
cultures, but does not teach the
provider to keep an open mind about
possible diversity within a culture.
• This pedagogy creates its own form of
academic stereotyping.
• Disrupts the continuity of care for
patients with chronic illnesses.
• Creates misconception that culture is
static which does not prepare medical
providers for the dynamic environment
of global health.
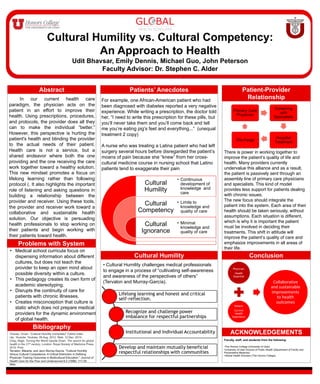
Cultural
Humility
Cultural
Competency
Cultural
Ignorance
• Continuous
development of
knowledge and
care
• Limits to
knowledge and
quality of care
• Minimal
knowledge and
quality of care
• Cultural Humility challenges medical professionals
to engage in a process of “cultivating self-awareness
and awareness of the perspectives of others”
(Tervalon and Murray-García).
Primary Care
Physician
Screening
with
Specialists
Hospital
Treatment
Discharge
There is power in working together to
improve the patient’s quality of life and
health. Many providers currently
undervalue this alliance and as a result,
the patient is passively sent through an
assembly line of primary care physicians
and specialists. This kind of model
provides less support for patients dealing
with chronic issues.
The new focus should integrate the
patient into the system. Each area of their
health should be taken seriously, without
assumptions. Each situation is different,
which is why it is important the patient
must be involved in deciding their
treatments. This shift in attitude will
improve the patient’s quality of care and
emphasize improvements in all areas of
their life.
Bibliography
Chavez, Vivian. “Cultural Humility (complete)” Online video
clip. Youtube. Youtube, 09 Aug. 2012. Web. 12 Dec. 2014.
Crisp, Nigel. Turning the World Upside Down: The search for global
health in the 21st century. London: Royal Society of Medicine Press,
2010. Print.
Tervalon, Melanie, and Jann Murray-García. "Cultural Humility
Versus Cultural Competence: A Critical Distinction in Defining
Physician Training Outcomes in Multicultural Education." Journal of
Health Care for the Poor and Underserved 9.2 (1998): 117-25.
Web.