Call Girls Rishikesh Just Call 9667172968 Top Class Call Girl Service Available
NCP-AKD.docx
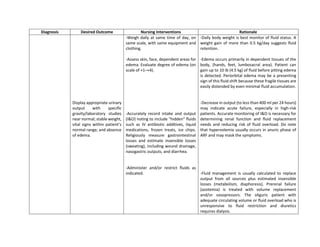
1. Diagnosis Desired Outcome Nursing Interventions Rationale
Display appropriate urinary
output with specific
gravity/laboratory studies
near normal; stable weight,
vital signs within patient’s
normal range; and absence
of edema.
-Weigh daily at same time of day, on
same scale, with same equipment and
clothing.
-Assess skin, face, dependent areas for
edema. Evaluate degree of edema (on
scale of +1–+4).
-Accurately record intake and output
(I&O) noting to include “hidden” fluids
such as IV antibiotic additives, liquid
medications, frozen treats, ice chips.
Religiously measure gastrointestinal
losses and estimate insensible losses
(sweating), including wound drainage,
nasogastric outputs, and diarrhea.
-Administer and/or restrict fluids as
indicated.
-Daily body weight is best monitor of fluid status. A
weight gain of more than 0.5 kg/day suggests fluid
retention.
-Edema occurs primarily in dependent tissues of the
body, (hands, feet, lumbosacral area). Patient can
gain up to 10 lb (4.5 kg) of fluid before pitting edema
is detected. Periorbital edema may be a presenting
sign of this fluid shift because these fragile tissues are
easily distended by even minimal fluid accumulation.
-Decrease in output (to less than 400 ml per 24 hours)
may indicate acute failure, especially in high-risk
patients. Accurate monitoring of I&O is necessary for
determining renal function and fluid replacement
needs and reducing risk of fluid overload. Do note
that hypervolemia usually occurs in anuric phase of
ARF and may mask the symptoms.
-Fluid management is usually calculated to replace
output from all sources plus estimated insensible
losses (metabolism, diaphoresis). Prerenal failure
(azotemia) is treated with volume replacement
and/or vasopressors. The oliguric patient with
adequate circulating volume or fluid overload who is
unresponsive to fluid restriction and diuretics
requires dialysis.
2. Excess fluid volume
related to
compromised
regulatory
mechanism (renal
failure) as
evidenced by
generalized tissue
edema, weight gain
Risk for Imbalanced
Nutrition: Less Than
Body Requirements
Maintain/regain weight as
indicated by individual
situation, free of edema.
-Assess and document dietary intake.
-Give patient/SO a list of permitted
foods or fluids and encourage
involvement in menu choices.
-Monitor laboratory studies: BUN,
albumin, transferrin, sodium, and
potassium.
-Aids in identifying deficiencies and dietary needs.
General physical condition, uremic symptoms
(nausea, anorexia), and multiple dietary restrictions
affect food intake.
-Provides patient with a measure of control within
dietary restrictions. Food from home may enhance
appetite.
-Indicators of nutritional needs, restrictions, and
necessity for and effectiveness of therapy.
Risk for Decreased
Cardiac Output
related to Uremic
effects on cardiac
muscle/oxygenation
Maintain cardiac output as
evidenced by BP and
HR/rhythm within patient’s
normal limits; peripheral
pulses strong and equal
with adequate capillary
refill time.
-Monitor BP and HR.
-Investigate reports of muscle cramps,
numbness of fingers, with muscle
twitching, hyperreflexia.
-Fluid volume excess, combined with hypertension
(common in renal failure) and effects of uremia,
increases cardiac workload and can lead to cardiac
failure. In ARF, cardiac failure is usually reversible.
-Neuromuscular indicators of hypocalcemia, which
can also affect cardiac contractility and function.
3. -Note occurrence of slow pulse,
hypotension, flushing, nausea and
vomiting, and depressed level of
consciousness.
-Note occurrence of slow pulse, hypotension,
flushing, nausea and vomiting, and depressed level of
consciousness.