Health ecosystem achieving impact in community health through public private partnership

This paper discusses how the failure of the public and the private healthcare systems has affected the poor. It also tries to explore the possibility of a financial mechanism like insurance and how it can bring about (from experiences drawn from other countries) the much needed health systems reform. This overall theme is known as the Health ecosystem Concept. This concept visualizes public health system beyond the realm of preventive/promotive care and explores newer avenues for Public-Private Partnership for curative care. In this document, insurance is visualized as not only paying for the curative care of the community but also tries to overcome the systemic errors in the current set up by improving infrastructure, providing incentives for man power and bringing about overall accountability into the system. It also suggests the use of technology to integrate and bring about efficiency in the entire health system and generate essential data in the process for evidence based action.

Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Health ecosystem achieving impact in community health through public private partnership
Similar to Health ecosystem achieving impact in community health through public private partnership (20)
More from CIRM
More from CIRM (20)
Recently uploaded
Recently uploaded (20)
Health ecosystem achieving impact in community health through public private partnership
- 1. HEALTH ECOSYSTEM: ACHIEVING IMPACT IN COMMUNITY HEALTH WITH PUBLIC PRIVATE PARTNERSHIP CONCEPTUALSIED AND COMPILED BY Dr.Imtiaz Ahmed CENTRE FOR INSURANCE AND RISK MANAGEMENT INSTITUTE FOR FINANCIAL MANAGEMENT AND RESEARCH 1
- 2. “The people’s health ought to be the concern of the people themselves. They must struggle for it and plan for it. The war against disease and for health can not be fought by physicians alone. It is a people’s war in which the entire population must be mobilized permanently. Henery Sigerist, Medical Historian. 2
- 3. Table of Contents Serial No. Topic Page No. 1. Introduction 6 2. Healthcare Financing Scenario in India 8 2.1 Indian Health care Financing-Broad Overview 8 2.2 Utilization of Healthcare Facilities 10 2.3 Source of Funding for Healthcare 11 3 Financing options for poor 12 3.1 Greater Public Health Investments 12 3.1.1 Health Infrastructure Inefficiency 12 3.1.2 Man Power Inefficiency 13 3.1.3 Programmatic and Management Inefficiency 14 3.2 Greater Private Sector Investment 15 3.3 Greater involvement of NGOs, MFIs and SHGs 15 3.4 External Funding 16 3.5 Micro Health Insurance 16 3.5.1 Evidence on the benefits of Micro Health Insurance 17 3.5.2 Micro Health Insurance in India 17 3.5.3 Way Forward 18 4 Health Ecosystem 19 4.1 Introduction 19 4.2 Strategy for Implementation 20 4.2.1 Primary Level 21 4.2.2 Secondary Level 24 4.2.3 Tertiary Level 26 3
- 4. 5 Conclusion 27 6 List of References 28 List of tables Table Title Page No. No. 1 Growth of Private Health Expenditure in India in comparison to 9 Public expenditure. 1951-2003 2 Private Health expenditure Trends 10 3 Share of each source in total reported out of Pocket expense on in 11 – patient care treatment 4 Expenditure by state department of health by system of medicine 14 in India,2001-02 List of Figures Figure No. Title Page No. 1 Vicious circle of poverty 7 2 Source of funds for availing healthcare in India 11 3 Percentage of community enrolled by distance 22 4
- 5. EXECUTIVE SUMMARY The public health system in India is plagued with the twin problem of an unresponsive, large, bureaucratic and heavily preventive/promotive focused government health system and an ever burgeoning, unregulated, costly and curative focused private health care system. The government health system has failed to provide preventive/promotive health care as most of its health resources be it infrastructure and manpower are in shambles. On the other hand the services offered by private health providers (though they provide state-of-the-art curative healthcare which is comparable with any such care provided worldwide) raises questions of equity, affordability and access (both in terms of physical as well as financial terms) for the general masses. About 70% of the private healthcare is situated in major cities and urban areas where only 30% of the country’s population lives. With an almost dysfunctional government healthcare system and absence of quality curative care in the public realm, the poor are forced to access private health facilities. To access such expensive care (in the absence of any comprehensive social security) the poor either have to borrow money or sell their asset which makes them vulnerable to poverty. This paper discusses how the failure of the public and the private healthcare systems has affected the poor. It also tries to explore the possibility of a financial mechanism like insurance and how it can bring about (from experiences drawn from other countries) the much needed health systems reform. This overall theme is known as the Health ecosystem Concept. This concept visualizes public health system beyond the realm of preventive/promotive care and explores newer avenues for Public-Private Partnership for curative care. In this document, insurance is visualized as not only paying for the curative care of the community but also tries to overcome the systemic errors in the current set up by improving infrastructure, providing incentives for man power and bringing about overall accountability into the system. It also suggests the use of technology to integrate and bring about efficiency in the entire health system and generate essential data in the process for evidence based action. One of the major focuses for implementing the health ecosystem concept is to see how efficiency can be brought into the whole system (the government and private sector) and how synergy can be brought about so that each system does what it is best suited to do with minimal investment in resource building and duplication. The ultimate focus of the argument is to make quality healthcare accessible, affordable and feasible for the poorest of the poor. 5
- 6. (1). Introduction: Health worldwide at an individual level, household or government level has not been a priority issue. Health has taken a backseat in the face of pressing and vital issues like livelihood and sustenance at an individual or household level and trade and commerce at a government level. However, considerable alarm and concern is expressed once a health situation gets out of control. It may be a catastrophic health event at the household level or an outbreak of an epidemic, a sharp rise in fatal diseases like cardiovascular diseases and the threat of HIV/AIDS assuming an epidemic or pandemic proportion at the government level. All of these events both at a micro or macro level gets accentuated and pose serious concerns in poor underdeveloped and developing countries. Developing countries are grappling with a constraint in resources, and are often mired with socio-political strife. In such a scenario, a health epidemic or pandemic will only aggravate the existing socio-economic conditions. Poverty as it is popularly said is the root cause as well as the effect of all the miseries and woes faced by a considerable chunk of population in these countries. So also it is with health. Poverty and ill health forms this vicious cycle depicted below: 6
- 7. Poverty Malnutrition Low income Disease Low Productivity Figure 1: Vicious Circle of Poverty and Disease At the global scenario, 84 percent of world’s poor share 93 percent of the global burden of disease.1 There are many reasons for such skewedness in the disease pattern world wide. There are issues of barrier to access which includes not only physical access but issues of affordability (financial accessibility) for the poor in availing quality healthcare. It is a most potent myth that availability of sophisticated and state-of-the-art curative care will ultimately address the issue of accessibility to quality healthcare. India has one of the largest private health sectors in the world with the quality of care comparable to the global standards. Yet, we as a country still grapple with diseases and ailments of 19th century Europe. The reason lies with the fact that such technology is not the most appropriate given the ground reality which often requires simple interventions rather than sophisticated technology Despite this fact the private healthcare market in developing countries like India, as in the USA, is based on a supply, induced by demand which keeps growing geometrically especially in the 1 Preker, A.S,. Carrin, G (2004) “Health Financing for Poor People – Resource Mobilization and Risk Sharing.” World Bank. 2004 7
- 8. context of new technologies2 which caters to a miniscule of the urban elite. On the other hand, the public health systems in India has a heavy preventive approach as far as rural areas are concerned whereas the curative care are concentrated in urban areas where only 25% of the country’s population lives. It is seen that when it comes to healthcare, poor and other excluded population are frequently forced to obtain care from private providers because public services in rural and low income urban areas are often scarce or plagued by understaffing, supply shortages and low quality care3. In order to avail quality healthcare, the poor access private facilities which are quite expensive and make low income households vulnerable to poverty. For example in India, nearly 40% of the poor either borrow money or sell assets to access private health care, 25% of them fall into poverty trap.4 In such a scenario where most of the poor access private healthcare and are vulnerable to poverty it becomes imperative to explore a synergy between the public and private healthcare institutions so that cheap and affordable healthcare of good quality is made available to the poor. Efforts should also be made to ensure the provision of an efficient financial option for the poor to protect them from the imminent health shock and long term financial risk. This paper would try to address these issues by analyzing the current health financing scenario in India. The paper also aims to delve on few questions like: what are the various financial options available for the poor, how can health insurance help in addressing the larger systemic challenges both in the public and private health domain and bring about an impact in the health infrastructure and manpower. The paper hopes to suggest an effective public-private partnership where health insurance will play a defining role in impacting health systems. (2) Healthcare financing scenario in India: (2.1) Indian Healthcare Financing- Broad Overview: The total value of the health sector in India is over Rs.15, 000 Billion or U.S $ 34 billion. This works out to about Rs. 1500 per capita which is about 6 per cent of GDP. Of this 15% is publicly financed, 4 percent is from social insurance and 1 per cent is from private insurance and the remaining 80 percent is out of personal resources as user fees.5 Historically healthcare financing in India can be broadly divided into public and private healthcare financing. As a percentage of GDP, the public expenditure on health has moved minimally from 0.71% in 1961 to 1% in 2003. In comparison, private expenditure on health increased from 2.25% of the GDP spent in 1961 to 5.6% of GDP in 2003. 2 Gangolli, Leena V., Duggal, R. Shukla, A. “Review of Healthcare in India.” CEHAT,2005 3 Preker A.S., H.Harding, and Girishankar. “Private Participation in supporting the social Contract in Health: New Insights from Institutional Economics”. Transaction Publishers,2001 4 Berman, P.,Macroeconomics and Health: Investing in Health for Economic Development. World Bank. 2001 5 Gangolli, Leena V., Duggal, R. Shukla, A. “Review of Healthcare in India.” CEHAT,2005 8
- 9. Table 1: Growth of Private Health Expenditure in India in comparison to Public Expenditures 1951-2003 When seen as percentage of total health expenditure, private health expenditure has grown from 78.43% in 1975-76 to 85.06% 2002-03 of total health expenditure. 9
- 10. Table 2: Trends in Private Health Expenditure Source: Gangolli, Leena V., Duggal, R. Shukla, A. “Review of Healthcare in India.” CEHAT ,2005 (2.2). Utilisation of healthcare facilities: When we see the utilisation of health expenditure trend across the 42nd and 52nd round of NSS, there is a 30 per cent decline in the use of public health care facilities in both rural and urban areas over the decade. This could be because the cost of treatment in public hospitals has increased over five fold in the given years. The other larger reason may be the fact that there is a perceived lack of quality of services being provided by these hospitals. This is reiterated by a study done by the Commission of Macro Economic and Health (CMH). According to this study, people regard national systems as impersonal and distant and they think that they will never benefit from its programmes.6 This view is reinforced when the national programs ration care to focus on “global” public health priorities which may have large externalities and benefits to society as a whole but often do not respond to the poor’s immediate day-to-day health care needs. Even where customised health services are provided at the village and at the sub-district level, the government cannot manage and monitor these services at the grass root level. Whatever the amount of funds spent, it does not produce the services people want and value, though the facilities are built and staffed. In such a scenario people are forced to seek private care which is relatively expensive for the poor. The various sources of healthcare funding in the country are discussed below to have a holistic view of the problem. 6 Berman, P., Macroeconomics and Health: Investing in Health for Economic Development. World Bank. 2001 10
- 11. (2.3). Sources of funding for healthcare: It is seen that about 72% of the entire funding for healthcare is from expenditure incurred directly by the household from their savings or other sources of out-of-pocket expenditure. Figure 2: Sources of funds for availing healthcare in India Source: National Health Accounts 2001-02 Table 3: Share of each Source in Total Reported Out- of- Pocket Expenditure on Inpatient Care As far as out of pocket expenditure is concerned, it is seen that on an average 39.1% of the money is being mobilised through selling of assets and borrowing across rural and urban households. It is 11
- 12. seen that as a result of such a step there is a chance of these households falling into a debt trap (49% in rural area and 28% in urban area).7 The impact of debt is significantly higher among low income households as debt recovery potential is lower which triggers the onset of poverty and ill health. (3). Financing options for the poor: In order to address this problem, there is a need to explore various options available and try to look at the efficiency of each. (3.1). Greater public health investment: With less than 1% of GDP devoted to financing public healthcare in the country, one logical argument can be to advocate an increase in the same by the government. It is seen that to meet a target of 3 per cent of GDP towards health expenditure, it necessitates 30 per cent of the government revenue but currently it stands at 3 per cent in India.8In a resource constraint country like India, there is a hesitancy to invest in the social sector like health and education where there is a long gestation period for such benefits to actually materialize. It is often seen as a deterrent for the government as compared to investment in trade and industries where the returns are tangible and faster. Due to the lack of government investment, the current public health system suffers from substantial inefficiencies. (3.1.1) Health infrastructure inefficiency: India follows a three tier health system of primary, secondary and tertiary level of health care delivery. The primary level of health care delivery consists of sub-centres and Primary Health Centres (PHC) which consist of a doctor, a nurse and other health staff. In most PHCs there is a severe lack of infrastructure facilities. Most PHCs are in need of modern diagnostics, clinical equipment and other problems which go unaddressed due to inefficiency in financial allocation and other managerial problems. This can be attributed to the large bureaucratic government structure attributed to the feeling of lack of ownership and gross inefficiency in the utilization of funds. Most funds as and when released do not get spent and often return back to the government on account of non-utilisation. It is estimated that nearly 60% of the total funds allocated for health goes towards paying salaries of the staff which has systematically gone up as a consequence of the 5th pay commission recommendation. It is because of such failures and other managerial inefficiencies, infrastructure and facilities within a government PHC and sub-centres continues to be of poor quality which discourages the population from utilizing it. The problem plaguing public health systems especially infrastructure in India can be summed up in the words of the National health Policy 2002 which says “It would detract from the quality of the exercise if, while framing a new policy, it were not acknowledged that the existing public 7 Gangolli, Leena V., Duggal, R. Shukla, A. “Review of Healthcare in India.” CEHAT,2005 8 Preker, A.S,. Carrin, G. “Health Financing for Poor People – resource Mobilisation and Risk Sharing.” World Bank. 2004 12
- 13. health infrastructure is far from satisfactory. For the outdoor medical facilities in existence, funding is generally insufficient; the presence of medical and para-medical personnel is often much less than that required by prescribed norms; the availability of consumables is frequently negligible; the equipment in many public hospitals is often obsolescent and unusable; and, the buildings are in a dilapidated state. In the indoor treatment facilities, again, the equipment is often obsolescent; the availability of essential drugs is minimal; the capacity of the facilities is grossly inadequate, which leads to overcrowding, and consequentially to a steep deterioration in the quality of the services.” (- National Health Policy, 2002) In such a scenario, low income households continue to use home remedies, self medication or traditional healers and local providers who are often outside the formal health system. The poor people often pay substantial amounts of money to get quality care from local healers, quacks and doctors thus becoming impoverished in the process besides exposing themselves to health hazards. (3.1.2). Manpower Inefficiency: It is seen that even where PHCs of satisfactory quality are present, there is a severe crunch of medical manpower to run these facilities. It is seen that there is a concentration of doctors in urban areas is at 73.6% whereas only 26.4% of the population live in rural areas.9 Most of the qualified doctors who are allopathic practitioners constitute a very strong lobby as majority of them belong to the private sector. There is virtually no regulation of the sector. The medical councils of the various systems of medicine perform only the function of registering qualified doctors and issuing them the license to practice. There is no monitoring, continuing education, price regulation, prescription and vetting either by the medical councils or the government. The private healthcare sector is strongly backed by the private pharmaceutical industry (largely multinational) which again constitutes a very powerful lobby that has kept at bay any progressive policy initiatives.10 There has also been a serious lack of interest on the part of the government to integrate the alternative health system practitioners in the realm of Indian Systems of Medicines and Homoeopathy (ISM & H) as is seen from the budgetary allocation 9 Park, K. “Park’s Textbook of Preventive and Social Medicine”. Banarasidas Bhanot, 2002. 10 Gangolli, Leena V., Duggal, R. Shukla, A. “Review of Healthcare in India.” CEHAT,2005 13
- 14. Table 4: Expenditure by the State Department of health on different systems of medicine in India, 2001-02 Source: National Health accounts 2001-02 In this regard the example of China is glaring and revealing. The basic unit of healthcare in China was called the Village health Station which served a population of 500-1000. Village stations are staffed by part time doctors whose training consisted of 3-6 months of basic medical education after junior middle school. The example of the integration of bare foot doctors in China which reinforces the fact that integration of alternative health system practitioners and local healers has always served the cause of improving the overall health status. (3.1.3). Programmatic and management inefficiency: As a state policy, the constitution of India has made healthcare services largely a responsibility of the state governments. However, there is room for greater ability to maneuver by the centre. As a result the health policy and implementation strategy are suggested by the Central government to be implemented by the state government. Under this policy the Central government has systematically pushed for vertical National Health Programmes which was not related to the health needs of the community and nor was the community ever consulted on the ways and means of implementing it. This led to lots of duplication of effort where central and state government machinery worked in a parallel manner without any coordination and synergy. The state government played the role of a passive onlooker because the funds were received from the central government. Besides, even the state health system adopts a heavy preventive/promotive approach which emphasizes on immunisation, awareness building and family planning activities. However, in most places these facilities are dysfunctional and services non-existent. 11 Another gross inefficiency which is evident in the entire health system of the country is the lack of a formal referral system for patients as seen in the National Health Services (NHS) in U.K. The absence of a referral system leads to a huge accumulation of patients at the secondary and tertiary level hospitals. Patients with minor ailments who could be treated conveniently at a primary centre go to a super specialist who forms the tertiary care. This hampers the optimum service delivery of these institutions and in the process also increases the waiting time of patients who actually need specialty care. 11 Gumber, A., Kulkarni, V., “Health Insurance for informal sector: case study of Gujarat, economic and political Weekly,30th September,2001 14
- 15. (3.2). Greater private sector investment: Private sector as is seen through the years has emerged as a major health sector player in the country. 83% of the total health care expenditure in the country is in the private sector. Although the private sector has the financial capabilities and the wherewithal to make investments in strengthening health system in India, but in reality such efforts has been entirely missing. One example can be cited of the bigger charitable trust hospitals which were given generous subsidies, tax exemptions and incentives by the government in return of the commitment that a certain percentage of the beds would be allocated free of cost or at a minimal cost for the poor. In reality how much of it is practiced is debatable. (3.3). Greater Involvement of Private Sector Organizations (NGO, MFIs and SHG): Community based organizations like Non-Government Organizations (NGOs), Micro Finance Institutions (MFIs) and Self Help Groups (SHGs) play a vital role in bridging the gaps between an inefficient, unresponsive, large and bureaucratic government system and an unregulated, costly though efficient private system. Such experiments in other sectors like education and financial inclusion has been tried out successfully and has yielded rich benefits. As community organizations are good aggregators, they can contribute a lot in terms of preventive/promotive health efforts. Besides organisations like MFIs and SHGs who already have financial programmes for greater financial inclusion of the poor, community organizations can be roped in to mobilize the community for collective risk pooling in the form of social health insurance or micro health insurance. Community orgnisations can also act as good mobilizers of community who can demand for their health rights through policy level advocacy which can bring in more accountability and efficiency in the health systems of the country. 15
- 16. (3.4). External Funding: Funding from international organisations to improve the overall health systems of the country may help in the short run but may not be sustainable in the long run. Moreover, the donors may be very rigid in allowing little flexibility in the spending programs. Donors may also resist having their budgets channeled to other programs. Donor aid is also unlikely to be a solution by itself but may be important at the margins if it is well utilized to bring about systemic reforms. (3.5). Micro Health Insurance: Micro health insurance as the name implies, is insurance for the socially and economically weaker sections which implies periodic (usually on an annual basis) payment of a small amount of money called premium to cover for the health risks that the individual/household faces. This arrangement allows for pooling of financial burden of illness to be shared between the relatively rich and poor, between the healthy and sick and between the gainfully employed and economically inactive. Such pooling also provides insurance against the expenditure variance related to uncertainty in the severity and cost of illness; a mechanism that is equally needed at low income levels.12 There is a clear advantage that insurance has over out of pocket expenditure. While out- of- pocket expenditure implies either getting money from savings, borrowing or selling of assets. These informal coping strategies generally provide insufficient protection. Many risk management strategies, such as spreading financial and human resources across several income generating activities, result in low returns. Informal strategies for coping with risk tend to cover only a small portion of the loss, so the poor has to garner resources together from a variety of sources. Even then, informal risk hedging does not stand up well against a series of perils, which unfortunately is a situation often experienced by the poor. Before the household has a chance to fully recover from one crisis, they are often struck by another.13 Where household survey data have been analysed, a consistent observation was that community based health financing has been effective in reaching low income population who otherwise would have no financial protection against the cost of illness.14Improved financial protection is achieved through reducing the members’ out of pocket spending while increasing their utilization of healthcare services.15 In a country like India where there is a large gap which is being left by the failure in both public and private health delivery to reach out to the poor, there is a need for a health care financing mechanism like insurance which functions on the principle of risk pooling and solidarity to reduce this gap through a comprehensive safety net approach. It is hoped that insurance can make quality healthcare accessible to the poor besides help bringing systemic improvement and changes in the existing health systems in the country. 12 Preker, A.S and Langenbrunner, J.C., “Spending Wisely- Buying Health Services for the Poor”, The World Bank, 2005 13 Churchill, C, “Protecting the Poor-A Microinsurance Compendium”, International Labour Organisation, 2006 14 Litvack, J.I., and C.I. Bodart. 1992. “User fees Plus quality equals improved Access to Health Care: Results of a Field experiment in Cameroon.” Social Science and Medicine 37(3): 369-83 15 Atim, C. 1998. “Contribution of Mutual Health Organisations to Financing delivery, and access to Health care: Synthesis of Research in Nine West and Central African countries. Technical Report 18. partnership for Health Reform project, Abt Associates Inc., Bethesda,Md 16
- 17. (3.5.1). Evidence on the benefits of micro health insurance: However, it is seen that due to the low level of awareness, low income households are initially reluctant to join insurance schemes. It has been the experience that when they are told that in the absence of risk protection, the cost of care becomes a barrier in obtaining health care and how the lack of immediate cash leads to catastrophic events in the household. Most of the poor households are willing to pay some amount of money for availing a risk pooling option. It has been observed that as a result of Health Insurance, there is a tremendous improvement in the financial accessibility of its members to modern healthcare system particularly for women, children and the poor. 16 Further due to Health Insurance, the out- of- pocket expenditure per illness are significantly lower for members as compared with non- members.17 The other beneficial effects of Health Insurance shows that the overall use of curative services for adults and children and preventive health services for children and women was up to five times higher for members than non- members.18 This shows that Health insurance also helps improve the health seeking behaviour of a population. (3.5.2). Micro Health insurance in India: However, when we look at the current state of micro health insurance in India, we find that there are not many successes in this realm. Universal Health Insurance Scheme (UHIS) of the government has been the biggest attempt by the government of India to provide universal insurance coverage for the country. However, the fact remains is that there is not much success achieved in terms of its penetration. Till date it has reached less than 1% of the country’s population despite heavy government subsidies and patronage. The government insurance companies started its first health insurance in 1986, under the name mediclaim; thereafter Mediclaim has been revised to make it an attractive product. Mediclaim is a reimbursement base insurance for hospitalization. It does not cover outpatient treatments. A person between 3 months to 80 years of age can be granted mediclaim policy up to maximum coverage of Rs. 5 lakh against accidental and sickness hospitalization during the policy period. Current statistics on health insurance indicate that out of 1 billion people in India only about 2 million are covered by the Mediclaim scheme. Most of the pro-poor health insurance schemes like the Jan Arogya Policy (JAP) run by the public health insurers are not for profit generating activities as the claims to premium ratio are high. One such interaction of the author with an official of a public insurer revealed that the only reason for running such a product is because it is being driven by the government as a social cause. When we look at the various schemes of the private insurer, we see that there is not much innovation seen in the product in terms of its customisation for the needs of the rural poor and is done more to meet the rural and social sector business mandate as laid down in the Insurance 16 Preker, A.S,. Carrin, G. “Health Financing for Poor People – resource Mobilisation and Risk Sharing.” World Bank. 2004 17 Ibid 18 Schneider P., and F.Diop. 2001. “Synopsis of Results on the Community – Based Health Insurance (CBHI) on Financial Accessibility to Healthcare in Rwanda. World Bank, HNP Discussion Paper. Washington, D.C 17
- 18. Regulatory and Development Authority (obligations of insurers to rural social sectors) regulations, 2002. There are about 400 million employed population in India out of which only 28 million is in the organized sector which leaves about 372 million people in the unorganized sector without any cover for their health risks. Of the 28 million, 8 million are being covered by the Employee State Insurance Scheme. It is financed jointly through contribution from workers (2.25% of their wage), the employee (4-5% of the wage) and the government which bears 1/4th to 1/8th of the expenses on medical benefits. This is a substantial expenditure in comparison to what the government spends on general health services. It has not however led to an improvement in the quality of care. Instead, the scheme has invested its funds and as of 1989, enjoyed a surplus income of Rs. 1240.55 million. All this amounts to mis-management and misuse of resources.19 While ESIS caters to a 3.2% of the entire population, about 0.5% of the population are being covered by the Central Government Health scheme (CGHS). Overall when we look at all the products of both public and private insurers, we find that not only the product has minimal penetration but also is poorly designed. Moreover, all of these schemes cover only hospitalisation and have varied exclusion criteria which again narrows down the spectrum of services provided. Illness brings with itself other ancillary costs other than the hospitalisation costs. This includes traveling costs, loss of wages for the patient and the attendant, diagnostic costs, medications and OPD charges. All of these costs are not covered currently within the existing insurance schemes. In this context, the existing insurance mechanisms have failed both in terms of penetration as well as being a comprehensive social security measure for the poor. In the absence of such a safety net mechanism, the poor borrows money or sells their assets to meet these expenses and consequently fall in to the vicious circle of poverty. (3.5.3). Way Forward: With this background in mind, the way forward can be by coupling the best practices in public and social medicine with an all inclusive health financing model which will ensure greater accessibility of the poor to quality healthcare. As popularly known, the study by John Snow during the great Cholera epidemic in London, paved the way for the great sanitary awakening in the west and ultimately the rise of public health. Since then public health has made a deep impact in improving the health status of the population worldwide. In India due to its slow progress, we face health problems faced by the western world 100 years ago. The overall morbidity profile of the country presents a disturbing picture with communicable diseases accounting for a majority of the burden and the rest being accounted for chronic and life style diseases which is already showing a steep rise and is costlier and requires sustained interventions for effective control demanding larger budgetary allocation. This coupled with an ever burgeoning elderly population adds to the cup of woes for health planners and the government in the country. One of the major reasons why public health has systematically failed in the country is because we as a country have typically focused on curative and non-ambulatory care. However we have somewhere missed the essence of preventive and promotive healthcare. Hence the present approach taken by the country is more a “fire fighting approach” rather than “preventing the-fire- from-occurring approach”. Hence there is a need to focus much more on such services for any 19 Preker, A.S,. Carrin, G. “Health Financing for Poor People – resource Mobilisation and Risk Sharing.” World Bank. 2004 18
- 19. health care provider who wants to focus on providing comprehensive health care and bring about visible improvement in the overall health status of the community. In such a scenario, where both public and private health systems have failed to provide comprehensive quality healthcare to the poor and also where financing for illness acts as a major stumbling block for poor households to avail care, there is a need for a mechanism in the form of insurance which needs to be integrated which not only addresses the issues of financial accessibility but also provides a broad social security mechanism. It is also hoped that insurance will bring about systemic changes in the health systems of the country through Public-Private Partnership. Overall such a mechanism will ensure sustainability of the programme (as a financing mechanism will pay for it) and efficiency (as it would be run through synergistic effort of government and private stakeholders). Let us now look at a comprehensive blue print on how such a health ecosystem can be implemented with health insurance playing a central and defining role. (4).Health Ecosystem: (4.1). Introduction: As discussed above, with an inefficient, large and bureaucratic public health system focused on primary, preventive and promotive care which is provided inefficiently and inadequately and a private health sector which is growing with absolutely no regulation and is expensive for a large section of the population who has no choice other than to choose the latter over the former. However, the flip side of the story is that when the poor try to access the expensive private healthcare they have to sell assets or borrow money which leads to severe impoverishment and pushes them below the poverty line. In such a scenario, there is a need for a financing mechanism which not only addresses the immediate financial needs of the poor household due to ill health but also provides a comprehensive social protection mechanism which aims to strengthen and bring synergy in the existing public and private health care delivery in the country. In the U.S such experimentation has been tried out successfully under the Healthcare Maintenance Organisation (HMO) concept where the healthcare provision and its management is outsourced to a third party entity which carries out this function and brings in operational efficiency. However, there is a fear that such a model may not work in a poor and resource constraint country like India where the health needs and operational issues with regard to health is very different from that in the western countries. However such fear can be allayed to the fact that the core concept of such a model can be used in India with enough community ownership and with sufficient inter-sectoral stakeholder involvement so that the maximum benefit from such a programme is being reaped by the poor. In such a context the four cardinal guiding principles of Primary health which is as follows needs to be always kept in mind: • Equitable Distribution • Community Participation • Inter-sectoral coordination and, • Use of Appropriate technology20 21 20 Alma Ata declaration 1978 21 WHO, 1976. WHO chronicle 30, 304 19
- 20. Till now most of the insurance programmes for the poor have not been able to achieve comprehensive care within these broad guiding principles. To start with, there is a serious problem in terms of equitable distribution of services as the services are only available to the members of the intermediaries (NGOs, SHGs, MFIs etc) as micro insurance is always given as a group policy in the name of the NGO where the name of the individual members are listed. Micro health insurance till now has only focused on hospitalisation for the poor which is not the pressing need of the population. The pressing needs include services like OPD, coverage for the loss of wages, traveling expenses, expenses incurred on medication and disability due to any ailments. Traditionally micro health insurance has not till date focused on preventive and promotive health care and continues to be involved in ‘fire fighting operations’. Most of the micro health insurance products existing in the market are either urban based products provided for the rural poor or a product in which not much thought has been spent in designing it to the needs of the poor. Hence there is no element of community participation. As a result the product fails miserably and incurs loss for the company who may eventually opt out of the business. Further as the commercial insurers have less knowledge of the context, they generally tie up with a community based organisations to deliver such a product. In geographies where such aggregators are efficient and have a good rapport with the local community, the products even if poorly designed work well. But the real problem arises when such a product is scaled up to other geographies and contexts and there is no proper customization or fine tuning done with the product to cater to the needs of the local population. The product is also likely to fail when the insurer/community organization does not tie up with all other stakeholders (like hospitals, primary care providers, PRI, Anganwadi etc). Most micro insurance schemes do not take the help of technologies like Management Information System (MIS), advanced technologies of management and latest technologies used by formal Third party Administrator (TPA). In this regard, there is lack or no use of appropriate technology. Within this context let us try to examine how a model of healthcare can operate with health insurance playing a central role to solve the challenges of financial risk mitigation for the poor but also addresses the larger challenges of public health in the realm of strengthening the infrastructure, incentivising the manpower, bringing in managerial intervention, using the latest technology to bring efficiency and systematically help bring down the overall cost involved for the poor in availing quality healthcare. This ‘Health Ecosystem’ model would try to act according to the guiding principles of primary healthcare as given in the Alma ata declaration. (4.2) Strategy for implementation: The strategy for implementation of the entire health ecosystem argument has to be a bottom-up approach rather than a top down approach. The strategy is put together based on the supposition that health insurance shall play a central role to which all services are linked to at each level of the health system of the state. The strategy at each level broadly explains what the health insurance coverage will be for that level, how it will impact (implicitly or explicitly) the health infrastructure, manpower and services, what will be the nature of public private partnership at each level and lastly how Information, Communication and Technology (ICT) can help integrate the entire system and bring about efficiency. At each step it will try to keep the guidelines of primary healthcare (as given in the Alma ata declaration) and see that it is adhered to in day- to- day operations. 20
- 21. Pre- enrolment Phase: A Community Needs Assessment (CNA) needs to be done where the community is brought together and asked to list down the following through a participative process: • Their health needs • The Willingness to pay (WTP) • The healthcare facility that they would like to access under the insurance scheme based on a map of the healthcare facility in the geography starting from the Primary up to the Tertiary level which is undertaken • The type of premium and payout that they are expecting from the insurance scheme • The broad range of social protection measures that they want the insurance to take up eventually i.e transportation, loss of wages, disability compensation etc. Depending on the mapping exercise undertaken by the health providers in the area and also the preference of the population for a given provider, rate negotiation (for consultation, hospitalisation and other associated cost) can be done with the provider hospitals to show them the business logic of increased footfall of patients and increased bed occupancy in their respective hospital. Based on the information provided by the community and also the negotiated rate from the hospitals, an actuarially sound product is designed after which there is another round of consultation with all the stakeholders’ i.e. the community, aggregator, and provider hospitals. This product is then taken to commercial insurers and negotiations are done with them so that whoever gives the best quote in terms of premium and payout amount is selected to be the insurer for the given scheme. This is done again in consultation with all stakeholders concerned. It is preferable that the community aggregator (NGO, MFIs, SHGs etc) plays the role of a TPA as they have got the maximum knowledge of the context and the community as a whole. The aggregator then can be given the stipulated fees for acting as the TPA which can be used to incentivise the field workers. Once the insurance policy is launched, the cascade of events at the various tiers of health care will proceed to maximize efficiency. At each tier, the terms of coverage which insurance will provide, the infrastructure, manpower and services through Public-Private Partnership, and the role of ICT in bringing in efficiency at each level will be looked at for ensuring that the health care received by poor is affordable, accessible, comprehensive and is of quality which is acceptable by the community as a whole. (4.2.1). Primary level: It is visualized that the enrolment of health insurance will be on a household/family basis which will ensure that the whole family/household and in turn the entire community will get health care on a cashless basis. It will also ensure the uniform spreading of risk at the family level and ultimately at the community level. (4.2.1.1). Insurance Coverage: The insurance will pay for the following services to the family/household at the primary level: 21
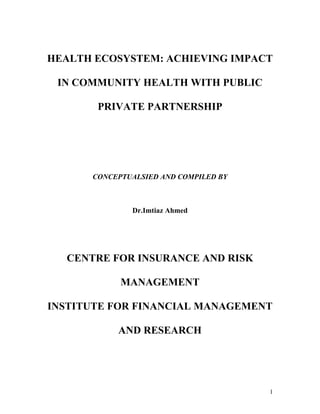
- 22. • User charge • Diagnostic charges • Expensive medication (like life saving drugs, higher antibiotics etc), injectibles and other consumables not usually available in the primary health centre • Specialist’s fee It is proposed that the primary healthcare provider or the first touch point should be quite nearby as studies reveal that household living less than 30 minutes from the health facility of insurance scheme were four times more likely to belong to pre-payment schemes than household living farther away.22 Percentage of Community Enrolled,by Distance 60 percent of community enrolled 50 40 30 20 10 0 0 14 26 distance from hospital (Km) Source: Preker, A.S,. Carrin, G. “Health Financing for Poor People – resource Mobilisation and Risk Sharing.” World Bank. 2004 Based on the scale and/or the insurance experience in 1st year, further benefits can be added as follows: • Reimbursement of transportation charges • Reimbursement of wage loss due to the illness (before, during and after illness) • Some financial compensation for the attendant accompanying the patients • Disability compensation and rehabilitative care Depending on the scale and volume of uptake of insurance, some money can be utilized for carrying out preventive/promotive health services from 1st/2nd year. 22 Preker, A.S,. Carrin, G. “Health Financing for Poor People – resource Mobilisation and Risk Sharing.” World Bank. 2004 22
- 23. (4.2.1.2). Impacting infrastructure, Manpower and Services through Public - Private Partnership: Infrastructure: Depending on the claims experience and the volume, some money can be utilized to purchase new or replace old goods/equipment at the Primary Health Centre (PHC). Some minimum fund can be given to the local Panchayat or a certain percentage of premium collected can be allowed to remain with them and the rest be spent for these purposes according to their discretion and mutual decision. If there is a need for 5-10 beds per hospitals at the taluk or at a district level in severely resource constrained area where such care is situated in far flung areas or in places where there is a serious issue of geographical accessibility. Emerging entrepreneurs like the Vatsalaya hospitals who have already set up such hospitals elsewhere in the country successfully needs to be encouraged and roped in to set up such hospitals. Local doctors looking at running hospitals can set up such hospital and run it on a franchise model. There is also a need for high end diagnostic chain to come in to the rural space. These diagnostic companies like Nicholas Piramal, Ranbaxy laboratories can set up satellite diagnostic centre at the taluk or district level. They can have sample collection units which collect the pathological samples from the villages and bring it to the satellite centre where it is examined. The report is either passed on to the patient the next day when the sampling collection team goes to the villages or can be sent directly to the referred doctor under the health insurance scheme. The logic behind the argument of these national level commercial players like hospitals, diagnostic and pharmaceutical majors coming to the rural space is the fact that most of these companies are exploring newer markets and consumers that have not been covered. Hence as part of their business expansion strategy in the rural area, it will auger well for these companies to join forces with such unique health ecosystem which will ensure that there is some profit involved and they do not do it entirely as a charitable undertaking. From the community perspective it is a sustainable proposition as quality medication are provided at a lower price on a sustained basis. Manpower: The Auxilliary Nurse Mid wives (ANM), Community Health Workers, Accredited Social Health Activists, Multi-Purpose Workers can be incentivised to provide their services more efficiently and quickly from a fund given to the Panchayat either from the government or from the insurance fund. At present the ANM spends about 40% of her time collecting health data and documenting it. It is assumed that with the introduction of ICT component (refer to the ICT sub point below) like smart cards, 40% of time wasted will be saved. This will give her more time to cover more villages, services and bring about efficiency in the overall health care delivery. It will also reduce paper work and make information easily accessible at each level. To incentivise the doctors to work in the PHC, posting qualified graduate doctors in PHCs can be made mandatory and also it can be made a pre-requisite for eligibility to sit for the Post- Graduate Medical Entrance Examination. Top 10 or 20 high performing PHC doctors in the entire state might be allowed to join the specialty of their choice in post-graduate courses directly or some higher percentage of the quota may be assigned to them which will facilitate them to get admission. This will incentivise young medical graduates to join PHC hence solving the technical medical manpower crunch at the primary level. 23
- 24. Services: It is high time that the public health system woke up to the fact that most of the curative primary care and to some extent secondary care is being provided by untrained healthcare practitioners, alternative system doctors and similar “unqualified” personnel. Efforts can be made to identify and train such personnel in basic curative care which can be handled efficiently by them while ensuring a satisfactory level of quality. They can be named as First Contact Health Personnel for the community. The extent of their interventions and associated technicalities can be sorted out by the government after discussion with various stakeholders. Transparency and accountability in the whole service delivery can be brought about by making the health manpower within the PHCs and other levels accountable to the PRIs and the Village Health Committee through a rigorous and scientific accountability system. Incentives or disincentives to the health staff can be based on the final opinion reached by the committee based on their evaluation. Information and Communication Technology (ICT): It is envisaged that an ICT component in the form of smart card technology be introduced. The smart card technology will be an exhaustive and comprehensive MIS which will capture all the data at present collected by the ANM in addition to other health data deemed necessary apart from financial data like insurance. The smart card will be a biometric card which will ensure that fraud is minimized. The smart card can be upgraded at each tier of health care offline as in villages power supply is erratic or absent and the internet connectivity is lacking. This would require a decoder cum uploading device which will be portable and hand held. This can be used by ANM/Health staff/PRI/Hospitals to upload or read information starting from the primary to tertiary level. The smart card will be able to transmit images of radiographic reports (X-ray and ultrasound) apart from other routine test results. Smart cards can be the precursor of telemedicine option to come in full force in this given health ecosystem. With internet connectivity through a satellite which is now provided free of cost by ISRO to interested NGOs and CBOs will mean that the patients would not have to travel to district level or tertiary level care and can walk into such tele-consulting centres within the village where his/her diagnostic reports are accessed by punching in the unique I.D number of the patient on the smart card. The specialist sitting at the district level can then assess the prognosis of the case and decide whether the patient needs to travel or else advice the local doctor on what is the line of treatment for the patient which then can be carried out locally. This will save a lot of money (on traveling and loss of wages), time and resources which the patient would have spent otherwise. It is also visualized that the smart card technology will be used to increase transparency and accountability of the health staff. In this the gram panchayat will completely evaluate the work of ANM and other staff including the doctor. Their performance will be graded on a scale devised in consultation with them and accordingly incentive/disincentive can be given based on the score and also common consensus of the pancahayat. This information can be made available online for access. (4.2.2). Secondary level: (4.2.2.1). Insurance Coverage: At secondary level the insurance will cover the cost of: • Hospitalisation 24
- 25. • Diagnostic services • Medicine and consumables • Consultation In addition, others services will be provided as was mentioned for primary level based on the volume of uptake and/or the claims experience. (4.2.2.2). Impacting infrastructure, Manpower and Services through Public Private Partnership: Infrastructure: At the secondary level, the private care hospitals needs to be identified as they are the most prominent player in the realm of curative care. There is now overwhelming body of evidence that most goods and services can be produced at good quality and at a lower price by non- governmental producers and that the state can achieve both efficiency and equity objectives through an active process of contracting, commissioning such services from those providers rather than passive subsidies.23 For such a thing to materialize, one of the best possible ways is to allow insurance to step in and help in the gradual transition of such private care to a more formalized provider which is financially sustainable in the long run. The private care hospitals can be encouraged to take up franchises of bigger corporate hospitals and operate as the local franchise. This will not only ensure a certain level of quality but also ensure that a referral linkage from these hospitals to parent hospitals is formalized. These hospitals then can be asked to increase the spectrum of specialized services offered by them gradually so that the patients do not have to travel long distances to the tertiary level. Manpower: Insurance can be used to incentivise the health manpower especially in the government system where the cost of curative care is very cheap. People getting admitted in such facilities that provide care at a subsidized rate, insurance could pay the hospital to the full amount that it pays for such ailments in any private facilities. This can be routed through the Rogi kalyan Samiti or the District Health Society which then can incentivise the medical staff based on their performance on a regular basis. Services: There is an acute need for standardization of treatment and diagnostic protocol so that the poor avail healthcare at a reasonable price rather than arbitrary ones which varies from one provider to the other. In the long run the national and state governments will have to play a benevolent intermediary role of bringing along all doctors (both government and private) on a common platform and ask them to mutually iterate and decide on a standardized treatment and diagnostic protocol. For this to eventually happen, as a beginning step, this could be tried out by the insurer with the private provider which will be quicker and hence demonstrable on a pilot basis. Eventually its success can be shown to the government doctors and hospitals so that they also help in bringing about the standardization of protocol in their hospitals as well. Lastly this evidence can be shown to both central and state governments for policy level advocacy and change. 23 Preker, A.S and Langenbrunner, J.C., “Spending Wisely- Buying Health Services for the Poor”, The World Bank, 2005 25
- 26. As far as costly life saving drugs, it is required at the secondary level, private pharmaceutical firms can be shown the business logic of doing business in the rural areas and be brought on board. They will help provide cheap generic medicine which will substantially bring down costs. Among services, insurance can also provide additional services for the National Health Programmes. It can work with various District Health Societies to offer rehabilitative care and financial help to patients who have recovered but are disabled due to diseases like leprosy or polio. It can also help the People Living with HIV/AIDS by providing additional services like providing nutritional supplement and other additional services which are not provided by the current national programme on HIV/AIDS. Insurance can acts as an effective risk mitigating tool for diseases like HIV/AIDS and lifestyle diseases which are rare but require costlier treatment and is insurable as a concept. Information and Communication Technology (ICT): There needs to be a secondary level data upgrading system which will either be software or just a portable device which will be put in the district hospital and will update data automatically. (4.2.3). Tertiary level: (4.2.3.1). Insurance Coverage: It will cover all high cost, sophisticated care which may not be available at the secondary level. (4.2.3.2). Impacting infrastructure, Manpower and Services through Public Private Partnership: It is envisaged that the government medical college hospitals, other government health institutions, central or regional health institutions operating in the state can act as the tertiary care provider. Insurance can start paying for upgrading infrastructure and incentivise the medical work force in a similar way as was explained under primary level care. Besides private healthcare who will start the franchise model or those interested and agreeable to the negotiated rate for the insured will act as the tertiary care provider. The benefit will be two fold - it will provide quality care to the poor and will also help reduce crowding in the government hospital. At the tertiary level, a working arrangement should be made with national level government hospital (like AIIMS,CMC etc), regional institutes, post graduate medical institutes (JIPMER) and large private/corporate hospital (Apollo, Wockhardt, Fortis etc) so that patient requiring advanced critical care can be referred to them. The government should play a central and leading role in developing a strong referral linkage in the state. Effort should be made right from the sub-centre level up to tertiary level so that only those patients who are referred to the next level can avail treatment at that level.(In line with the NHS model followed in Great Britain) As discussed, it is a fact that most high level tertiary care hospitals are charitable trust hospitals and get lots of subsidies and exemptions from the government in return for providing subsidized services for the poor but in reality a very few actually provide such services. The government can be advocated with these facts so that it is made mandatory and compulsory for these hospitals to treat the insured poor. Information and Communication Technology (ICT): 26
- 27. There will be a central data warehouse which will integrate all the information collected from the primary level upwards, making it accessible to each level and hence acting as a central store house of information. Additionally it will have personnel’s who will analyse such data. Such analysis will be invaluable for monitoring, evaluation and mid-course correction. The developing of referral linkages is possible with insurance playing a central role and ICT in the form of smart card technology will ensure equity, efficiency and quality in healthcare delivery at each level. The coupling of the whole machinery with tele- medicine will bring about synergy and help the poor in terms of saving money on traveling and also loss of wages. It has to be always borne in mind by all the stakeholders that all components of health care i.e. preventive, promotive, curative and rehabilitative care should work together harmoniously and efficiently with insurance playing a defining role. Conclusion: Promoting health and confronting challenges of diseases requires action across a range of activities in the health system. This includes improvements in policy making and the role of the government; better access to human resources, drugs, medical equipment, and consumables; and a greater engagement of both public and private providers of health services. In this context health insurance can play a pivotal role in redefining and restructuring health systems so that quality healthcare is affordable and accessible for the poorest of the poor. 27
- 28. List of References 1) Preker, A.S,. Carrin, G (2004) “Health Financing for Poor People – resource Mobilisation and Risk Sharing.” World Bank. 2004 2) Gangolli, L.V., Duggal, R. Shukla, 2005A. “Review of Healthcare in India.” CEHAT, 3) Preker A.S., H. Harding, and Girishankar. 2001 “Private Participation in supporting the social Contract in Health: New Insights from Institutional Economics”. Transaction Publishers, 4) Berman, P., 2001Macroeconomics and Health: Investing in Health for Economic Development. World Bank. 5) CSO-GOI National Accounts Statistics,2003 6) National Health Accounts 2001-02 7) Park, K. 2002 “Park’s Textbook of Preventive and Social Medicine”. Banarasidas Bhanot, 8) Gumber, A., Kulkarni, V., “Health Insurance for informal sector: case study of Gujarat, economic and political Weekly,30th September,2001 9) Preker, A.S and Langenbrunner, J.C., 2005 “Spending Wisely- Buying Health Services for the Poor”, The World Bank, 10) Churchill, C, 2006 “Protecting the Poor-A Microinsurance Compendium”, International Labour Organisation, 11) Schneider P., and F.Diop. 2001. “Synopsis of Results on the Community – Based Health Insurance (CBHI) on Financial Accessubility to Healthcare in Rawanda. World bank, HNP Discussion Paper. Washington, D.C 12) WHO, 1976. WHO chronicle 30, 304 13) Roberts, M.J., Hsiao, W., Berman, P., Reich, M.R 2004 “Getting health reforms right-A guide to improving performance and equity” Oxford University Press. 14) Duggal R., Nandaraj S., Shetty S. The Foundation for Research in community Health, 1992. 15) Gill, S., Kavadi S.N.1999 “Health financing and costs-a comparative study of trends in eighteen countries with special reference to India” The Foundation for Research in community Health 16) . Upelkar, M.W., Antia, N.H 1996 “Healthcare Financing in India” The Foundation for Research in community Health. 17) Dror, D.M., Preker, A.S. 2002” Social Reinsurance” World bank and ILO 28
- 29. 18) Mizunoya,S. Behrendt., C. Pal., K ., Léger, F,2006 “Costing of basic social protection benefits for selected Asian countries: First results of a modeling exercise. ILO , STEP. 19) Health Micro-Insurance Schemes: Feasibility Study Guide,2005. ILO, STEP 29