
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Eoms & ocular motility
Similar to Eoms & ocular motility (20)
Recently uploaded
Recently uploaded (20)
Eoms & ocular motility
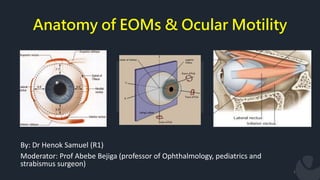
- 1. Anatomy of EOMs & Ocular Motility 1 By: Dr Henok Samuel (R1) Moderator: Prof Abebe Bejiga (professor of Ophthalmology, pediatrics and strabismus surgeon)
- 2. Contents • Introduction • Recap on Embryology & microscopic anatomy • Gross Anatomy of EOM • Origin, Nerve and blood supply • Action of EOM • Basic Kinematics, Mechanics • Ocular Movements • Fundamental Laws governing ocular motility 2
- 3. Why do we move our eyes? A. To acquire objects for central viewing Saccadic eye movements B. To maintain objects in foveal view Pursuit eye movements C. To stabilize the world on the retina 3
- 4. Extraocular Muscles 4 EOMS are: Striated voluntary muscles Among muscles with fastest but also most sustained contraction Get high blood flow exceeded only by myocardium Have got high innervation ratio
- 5. Extraocular Muscles 5 Play a vital role in Stereopsis Conjugate eye movements Maintenance of primary gaze position Motor fusion – maintaining corresponding visual elements within the binocular field on corresponding retinal loci. Following of moving objects (smooth pursuit) Accomplish rapid changes in fixation (saccades).
- 6. Embryology The EOMs are derived from three primordial condensations - paraxial and prechordal mesoderm. A pair of premandibular mesodermal condensation – 26th day Those muscles innervated by CNIII MR, SR, IR & IO . Two maxilomandibular condensations – 27th Superior oblique . Lateral rectus . Associated periorbital CT and smooth muscle are derived from the neural crest. 6
- 7. Embryology Their development begins at 3–4 weeks gestation. All of the extraocular muscles and their surrounding tissues are present and in their final anatomic positions by 6 months gestation. The tendon insertions initially extend from the limbus to the equator. Continue to change until 18 months to 2 years after birth - 2–3.0 mm narrower in infants At about 1 month, the nerves to the extraocular muscles reach their respective destinations in the sequence oculomotor, abducens, and trochlear. 7
- 8. Microscopic Anatomy of EOMs Different from other skeletal muscles by their Diameter of its fibers is small Contain both slow and fast fibers denser connective tissue & blood supply Contain an enormous amount of fibroelastic tissue connective tissue sheaths are more delicate & richer in elastic fibers Have a large nerve to muscle fiber ratio; about 1:5 to 1:10 compared to 1:100 or more in other skeletal muscles 8
- 9. Microscopic Anatomy of EOMs Components of a muscle fiber Sarcolemma: the plasma cell membrane surrounding each muscle fiber. Transverse tubules (T tubules): a series of invaginations of the sarcolemma into the cell. Sarcoplasm: is the cell cytoplasm & contains normal cellular structures and special muscle fibers, THE MYOFIBRILS. 9
- 10. Microscopic Anatomy of EOMs Components of a MYOFIBRIL; two types 1. Thick myofilaments 2. Thin myofilaments 10
- 11. Microscopic Anatomy of EOMs Twitch single innervated fibers ( thick ):- contain little mitochondria ( i.e. anaerobic metabolism ) → rapid response to the stimulus with rapid contraction of high amplitude & short duration. responsible for saccadic eye movement & help fixation & pursuit movement. Tonic multiple innervated fibers ( thin ):- contain numerous mitochondria ( i.e. aerobic metabolism ) → slow response to the stimulus with slow contraction of low amplitude & long duration. responsible for gaze in all positions including 1ry position. 11
- 12. Bony orbit • 12
- 13. Extraocular Muscles (EOMs) Vertical rectus - Superior rectus - Inferior rectus Horizontal rectus - Medial rectus - Lateral rectus Obliques - Superior oblique - Inferior oblique 13
- 14. Origin of EOMs The four recti muscles have their origin on the common tendinous ring (annulus of Zinn). The area enclosed by the tendinous ring is called the oculomotor foramen Superior Oblique originates from the lesser wing of sphenoid Inferior Oblique originates from the maxillary bone 14
- 15. Several blood vessels & nerves pass through oculomotor foramen 1. The optic nerve 2. Ophthalmic artery 3. Abducens nerve 4. Oculomotor nerve Upper and lower divisions 5. Nasociliary branch of the ophthalmic 15
- 16. Insertion Scleral insertions are by tendons whose fibres are parallel to the long axis of the muscle. The tendon fibres enter the superficial sclera and quickly merge into it. The EOMs penetrate it ≈10 mm posterior to their insertions 16 MUSCLE LENGTH OF TENDON IN mm MEDIAL RECTUS 3.7 LATERAL RECTUS 8.8 SUPERIOR RECTUS 5.8 INFERIOR RECTUS 5.5 SUPERIOR OBLIQUE 25 INFERIOR OBLIQUE 1
- 17. Arterial supply Three main sources 1. Muscular branches of ophthalmic artery Upper (lateral) branch Lower (medial) branch 1. Infraorbital artery from ECA 2. Lacrimal artery 17
- 18. Arterial supply The muscular branches give rise to the anterior ciliary arteries accompanying the rectus muscles; each rectus muscle has 1–4 anterior ciliary arteries. Anterior segment circulation is most dependent on arteries from vertical rectus muscles and least dependent on arteries from the lateral rectus muscle Surgical manipulation of the rectus muscles permanently disrupts the anterior ciliary arteries. 18
- 19. Venous drainage 19 Follow the arterial path EOMs drain into two veins: 1) Superior ophthalmic vein and 2) Inferior ophthalmic vein
- 20. Nerve 20 Without neural activity, the visual axes are usually mildly to moderately divergent. The major tonic input to ocular motility is supplied CNs III, IV, and VI
- 21. Superior rectus • Origin • Insertion • Nerve supply • Blood supply 21
- 22. Inferior rectus • Origin • Insertion • Nerve supply • Blood supply 22
- 23. Medial rectus • Origin • Insertion • Nerve supply • Blood supply 23
- 24. Lateral rectus • Origin • Insertion • Nerve supply • Blood supply 24
- 25. Spiral of tillaux 25 Imaginary line joining the insertions of the 4 recti and is an important anatomical landmark when performing surgery.
- 26. Superior Oblique • Origin • Insertion • Nerve supply • Blood supply 26
- 27. Inferior Oblique • Origin • Insertion • Nerve supply • Blood supply 27
- 28. Introduction • Obliques are inserted behind equator & form an angle of 51° with visual axis. 28
- 29. Orbital Connective Tissue Tenon's capsule (fascia bulbi) a layer of delicate connective tissue that completely envelops the globe - EOMs penetrate it ≈10 mm posterior to their insertions The fascial sheath of the SR muscle closely adheres to the sheath of LPS of upper lid in front of the equator which accounts for the cooperation in elevation of the eye. The sheath of the IO muscle fuses with the sheath of the IR and forms the suspensory ligament of lockwood. 29
- 30. Pulleys of the EOMs Are about 2mm in length & located near the equator Function as a mechanical origins of the EOMs Reduce sideslip of the extraocular muscles during globe rotation and help to determine the effective direction of pull 30
- 31. Pulleys of the EOMs They are Composed of Elastic fibers Collagenous The smooth muscles The most prominent smooth muscle is the inframedial orbital muscle extending between the MR and IR pulleys. Anteriorly, these sleeves thin to form slings known as the intermuscular septum. 31
- 32. Muscle Capsule Each rectus muscle has a surrounding fascial capsule Extends with the muscle from its origin to its insertion Its smooth avascular surface allows the muscles to slide smoothly over the globe. 32
- 33. Action of extraocular muscles Types of Eye Movements 1. Ductions refer to monocular movements of each eye. 2. Versions refer to binocular conjugate movements of both eyes. 3. Vergences refer to binocular disjunctive movements. 33
- 34. Uniocular movements Ductions – only one eye is open, the other covered/closed tested by asking the pt. to follow a target in each direction of gaze. Types of ductions:- 1. Adduction 2. Abduction 3. Supraduction 4. Infraduction 5. Incycloduction 6. excycloduction 34
- 35. Three Axes of Eye Rotations Fick’s Axis Listing Plane 35 Uniocular movements
- 36. Binocular movements 36 Versions:-both eyes open, attempting to fixate a target & moving in same direction. Binocular, simultaneous, conjugate movements in same direction. Abduction of one eye accompanied by adduction of other eye is called conjugate movements.
- 37. Introduction Types of versions:- Dextroversion & laevo version Supraversion & Infraversion Dextro elevation & dextro depression Laevo elevation & laevo depression 37
- 38. Introduction • Torsional movements/righting reflexes:- When you tilt head to maintain upright image. • Vergences:- binocular,simultaneous,disjugate/disjunctive movements (opp direction) Convergence– simultaneous adduction Divergence– outward movement from convergent position 38
- 39. Actions of EOMs • The anterior pole of the globe is the reference point used in the description of any eye movement • Eye movements are described based on the movement of the muscle insertion towards its origin. • The primary action of a muscle is its major effect when the eye is in the primary position. • Subsidiary/secondary actions are the additional effects & depend on the position of the eye • The point at which the center of the muscle or its tendon first touches the globe is called the tangential point and indicates the direction of the pull. • Muscles exert force in proportion to their cross-sectional area and length. • For normal amplitude of rotation (45-50 degree ) 10mm change in muscle length is required in each direction 39
- 40. Positions of Gaze Primary position: defined as position of the eye with Both head & body erect Both eyes are looking straight ahead Object of regard is at infinity The eye located at the intersection of the sagittal plane of the head and the horizontal plane passing through the centers of rotation of bot eyes 40
- 41. Positions of Gaze Secondary position are rotations around either the vertical axis or the horizontal axis. ADDUCTION ABDUCTION ELEVATION DEPRESSION 41
- 42. Positions of Gaze Teritiary position: are rotations around both the vertical & horizontal axis DEXTROELEVATION DEXTRODEPRESSION LEVOELEVATION LEVODEPRESSION 42
- 44. Medial Rectus Lies parallel to the sagittal axis & perpendicular to the vertical axis As a result has only one action, which is rotation around the vertical axis medially => ADDUCTION 44
- 45. Lateral Rectus Lies parallel to the sagittal axis & perpendicular to the vertical axis Contraction causes rotation in a temporal direction ABDUCTION 45
- 46. Superior Rectus Run in line with the orbital axis and are inserted in front of the equator. Forms an angle of 23° with the visual axis. With the insertion above the origin and on the anterior globe, movement around the horizontal axis causes ELEVATION – PRIMARY ACTION. 46
- 47. The muscle insertion is lateral to the origin, so movement around the vertical axis causes ADDUCTION. Its oblique insertion with the nasal side closer to the limbus than the temporal side on the superior surface of the globe causes INTORSION on contraction. 47 Superior Rectus
- 48. Inferior Rectus Its insertion is below its origin and on the anterior globe, so movement around the horizontal axis causes DEPRESSION 48
- 49. Inferior Rectus The muscle insertion is lateral to the origin, so movement around the vertical axis causes ADDUCTION. Its oblique insertion on the inferior surface of the globe causes EXTORSION on contraction. 49
- 50. Superior Oblique The oblique insertion on the posterosuperior lateral aspect of the globe causes rotation of the eye around the sagittal axis causing INTORSION. 50
- 51. Superior Oblique The insertion is posterior and inferior to the physiologic origin; contraction of the muscle pulls the back of the eye up, and the anterior pole moves down- DEPRESSION. 51
- 52. Superior Oblique Because the insertion is lateral to the trochlea, contraction pulls the back of the globe medially, thus moving the anterior pole laterally – ABDUCTION. 52
- 53. Inferior Oblique Because the muscle wraps around the lower portion of the globe and the insertion is superior and lateral to the origin contraction causes EXTORSION. 53
- 54. Inferior Oblique Because the insertion is on the posterior eye and above the origin, contraction pulls the back of the eye down, elevating the front – ELEVATION. 54
- 55. Inferior Oblique because the insertion on the back of the eye is pulled toward the medial side; thus the anterior pole is moved laterally in ABDUCTION 55
- 56. Actions of the EOMs from secondary position HORIZONTAL RECTUS MUSCLES: LR & MR If the eye is elevated, contraction of the LR & MR no longer causes strictly adduction or abduction but also causes a slight elevation if the eye is depressed, contraction causes further depression 56
- 57. VERTICAL RECTUS MUSCLES : SR & IR 57 When the globe is abducted 23°, the visual and orbital axes coincide. In this position they have no secondary actions The SR can act only as an elevator & IR only as a depressor
- 58. VERTICAL RECTUS MUSCLES : SR & IR When the eye is adducted 670 the plane of the vertical rectus muscles is at a right angle to the sagittal axis and thus parallel to the horizontal axis. The superior rectus could only act as an intortor & the inferior rectus could act only as an extortor. 58
- 59. THE OBLIQUE MUSCLES : SO & IO The obliques form an angle of 51° with the visual axis So if the eye is adducted 510, the plane of the oblique muscles becomes parallel to the sagittal axis and perpendicular to the horizontal axis. Thus contraction of the SO will cause only depression, and the IO will cause only elevation 59
- 60. THE OBLIQUE MUSCLES : SO & IO When the eye is abducted 390, the plane of the oblique muscles makes a right angle with the sagittal axis & parallels the horizontal axis, The superior oblique can cause only intorsion & the IO extorsion 60
- 62. Fundamental Laws governing Ocular Motility Synergists:- refers to muscles having same primary action in same eye. Ex:- sup.rectus & inf.oblique----elevators inf.rectus & sup.oblique-----depressors Antagonists:- muscles having opposite action in same eye Ex:- sup. & inf. Recti sup. & inf.oblique 62
- 63. Fundamental Laws governing Ocular Motility Yoke muscle (contralateral synergists):- Ref. to pair of muscles (one from each eye) which contract simultaneously during version movements. Ex :- In dextroversion RLR &LMR Contralateral antagonist:- pair of muscle (one from each eye) having an opposite action. Ex:-In dextroversion RLR & LLR 63
- 64. Fundamental Laws governing Ocular Motility 64 DONDER’S LAW To each positon of line of sight belongs a definite orientation of the vertical and horizontal retinal meridians relative to the coordinates of space. The orientation of the retinal meridians pertaining to a particular position of globe is achieved irrespective of the path the eye has taken to reach that position. In short, it implies that there is one and only one orientation of the retinal meridians with each position of the eyes.
- 65. Fundamental Laws governing Ocular Motility Hering’s Law of Equal Innervation Also known as Hering’s law of motor correspondence States ‘ equal and simultanous innervation flows from the brain to a pair of muscles of both eyes (yoke muscles) which contract simultaneously in different binocular movements.’ Eg: Right Lateral R and Left Medial rectus: Dextroversion Both Medial Rectus : Convergence Right IR and Left Superior Oblique: Dextrodepression 65
- 66. Fundamental Laws governing Ocular Motility Sherrington’s Law of Reciprocal Innervation ‘During ocular motility, an increased flow of innervation to the contracting agonist muscle is accompanied by a decreased flow of innervation to the relaxing antagonist muscle’. Eg. During Dextroversion, Increased innervation – Right LR and Left MR Decreased innervation – Left LR and Right MR 66
- 67. References Wolf anatomy of the eye and orbit Clinical anatomy and physiology of the visual system Duane’s Ophthalmology 2007 edition parts 1 and 2 Kanski clinical ophthalmology 7thedition chapter18 BCSC 2019, section 2 and 7 67
- 68. 68 Thank You!
Editor's Notes
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- In the retina we have a highly specialized system in higher mammals and humans where there is only small area where there is high density photoreceptor so to see fine detail u need to move your eyes to location u need to analyze with high level of acuity. It involves Acquire object for central viewing bcz its central viewing that allows u to have high acuity. Those accomplish predominantly by saccadic eye movt – which r rapid eye movt fr one location to another. Another impt whn u see like a bird flying…in order to analyze it u track z object – smooth pursuit mechanism which enable u to analyze the world accurately. Another factor is that whn we move abt its imp for eyes to be stable with respect to the world out there. One of the mechanism is Accessory optic system controlling eye visual stimuli and vestibular system.
- There are 7 extraocular muscles (EOMs) in the human eye: 4 rectus muscles 2 oblique muscles levator palpebrae superioris muscle All these muscles except LPS work with the surrounding orbital tissues to provide smooth movements of the globes and allow for binocular vision. Seventh muscle called LPS Similar in innervations Physiologically and metabolically different
- There are 7 extraocular muscles (EOMs) in the human eye: 4 rectus muscles 2 oblique muscles levator palpebrae superioris muscle All these muscles except LPS work with the surrounding orbital tissues to provide smooth movements of the globes and allow for binocular vision. Seventh muscle called LPS Similar in innervations Physiologically and metabolically different
- The EOMs form from paraxial and prechordal mesoderm, following cues from the developing eye as well as from surrounding neural crest mesenchyme Their development begins at 3–4 weeks gestation All of the extraocular muscles and their surrounding tissues are present and in their final anatomic positions by 6 months gestation.
- At about 7 weeks the dorsomedial aspect of the superior rectus muscle gives rise to the levator muscle they do not begin development at their origins and sprout toward their respective insertions
- Epimysium : a connective tissue sheath surrounding the entire muscle Perimysium: continuous with epimysium infiltrates the muscle & divides it into bundles Endomysium: a delicate connective tissue enclosure that surrounds the individual muscle fiber within the bundle
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- thick myofibrils composed of hundreds of myosin subunits These filaments lie next to each other and form the “backbone” of the myofibril thin myofibrils formed by the protein actin arranged in a double-helical filament & a molecular complex of troponin and tropomyosin lying within the grooves of the double helix
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Each eye lies within the orbit The medial walls of the orbit are parallel to the midsagittal plane The lateral walls form an angle of ≈ 900 with each other. medial and lateral orbital walls thus form an angle of ≈ 450 with each other. Each orbital axis diverges from the midline by 22.50 and from the axis of the other orbit by 450
- Origin Common tendinous ring: “annulus tendinous communis”, the annulus of Zinn SR and MR closely attached to the dural sheath of the optic nerve at their origin
- the annulus of Zinn SR and MR closely attached to the dural sheath of the optic nerve at their origin It is this attachment of the superior and medial recti to the nerve sheath which is responsible for the characteristic pain which accompanies extreme movements of the globe in retrobulbar neuritis. Superior Oblique originates from the lesser wing of sphenoid
- In thyroid orbitopath MR and IR thickens especially ner the orbital apex compressing the optic nerve as it enters the optic canal
- They resemble scleral fibres, being of the same tissue, but differ in size and, whereas tendon fibres are mostly longitudinal, the scleral fibres run in many directions Only the cessation of the thick elastic fibres marks the junction of tendon with sclera Medial rectus muscle is suseptable to injury during anterior segment surgery inadvertent removal of the MR is a well known complication of perygyium removal. If integrity of tenon capsule lost during trauma or surgery 10mm posterior to limbus fatty tissue prolapse will result in restrictive adhesion and limit ocular motility
- SUPERIOR/LATERAL BRANCH - LR , SO, SR INFERIOR/MEDIAL BRANCH – MR, IO, IR The arteries to the four rectus muscle give rise to the ant ciliary arteries Blood supply to EOM supplies most of ant segment thus simultaneous surgery on 3 recti induces ant segment ischemia External carotid - Maxillary artery - Infraorbital artery Inferior rectus Inferior oblique
- These cilliary vesels pass to the episclera of the globe and then supply blood to the anterior segment The long posterior ciliary arteries also supply the anterior segment of the eye with blood via the major arterial circle of the iris. These long posterior ciliary arteries allow collateral blood flow after rectus muscle surgery. The blood vessels that supply the oblique muscles do not carry any circulation to the anterior segment.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Except for IO, innervation to each of the EOMs occurs ≈1/3 the distance from the apex IO receives its innervation at ≈ its midpoint All 6 EOMs receive their innervation on the inside surface, except for SO, where branches of CN IV terminate on the upper (outer) surface
- Arises from upper part of annulus o zinn. Below the attachment of levator M. Continuous with attachment of med.,&lat. Recti Pierces tenon’s capsule &it is inserted into sclera 7.7 mm from superior limbus. Length 48 mm;width 9mm. N.supply:-sup.divison of oculomotor N. B.supply:-lat. Muscular branch of ophthalmic A
- Shortest of all recti Arises from lower part of optic foramen. Attached to sclera at 6.5 mm from inferior limbus Lies b/w globe and inf.oblique. Also attached to fascial sheath of lower lid. Length 40mm;width 9mm N.supply:-branch of inf divison of oculomotor N. B.supply:-medial muscular branch of ophthalmic A
- Largest ocular M& stronger than lateral rectus. Arise from medial & inferior sides of optic foramen Passing along medial wall of orbit ;inserts 5.5mm from nasal limbus. Length 40mm;thicker than other EOM. N.supply:-inf.divison of oculomotor N. B.supply:-medial muscular branch of ophthalmic A
- Arises from annular tendon. Pierces tenon’s capsule &inserts in sclera at 6.9 mm from temporal limbus. Length 48mm;2/3 of cross sectional area of MR. N.supply:-Abducent N enters lR on its ocular aspect,just post.to its mid point.
- The insertions are located progressively further away from the limbus in a spiral pattern. the medial rectus insertion is closest. Superior rectus is farthest
- Longest& thinnest EOM. Arises from common origin at the apex of orbit; superomedial to optic foramen. Runs forward to trochlea(cartilaginous ring at upper&inner angles of orbit) After threading through this it becomes tendinous It changes its direction completely and runs over the globe under SR to attach above & lat, to posterior pole. N.supply:-Trochlear N(4) after dividing into 2-3 branches enters muscle superiorly. B.supply:-superior muscular branch of ophthalmic A. The trochlea redirects the tendon inferiorly, posteriorly, and laterally, with the tendon forming an angle of 51° with the visual axis in primary position
- Only EOM not arising from apex of orbit It arises anteriorly from lower & inner orbital walls near lacrimal fossa. Running below inf.rectus& attaches below&lat. to post.pole of globe. N.supply:-Inf.divison of oculomotor N. B.supply:-Infraorbital &medial muscular branches of ophtalmic A
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Apart from serviing as cavity, support and protection of the globe, they play an important role in control of eye movement, reducing retraction
- They are Composed of Elastic fibers which provide reversible extensibility collagenous pulley ring forms the fulcrum of the pulley that inflects the EOM path The smooth muscles provide modulatory force on the pulleys Pulley displacement can clinically mimic muscle dysfunction, and orbital imaging may be needed to distinguish it accurately from a palsy. The pulling direction of each EOM is thus defined by the line segment connecting the EOM's scleral insertion to the respective pulley
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- center of rotation, located 13.5 mm behind the apex of the cornea & 1.3mm behind the equatorial plane this point varies in ametropia, is slightly more posterior in myopia, and is slightly more anterior in hyperopia 3 types of rotation: Listing Plane is an imaginary coronal plane passing through the center of rotation of globe 1. Rotation around fick vertical axis Z—side to side 2. “ “ fick horizontal axis X– up&down 3. “ “ fick antero posterior axis– torsion Torsions or cyclorotations are rotations around the sagittal axis and are described in relation to a point at the 12-o’clock position on the superior limbus.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- ; When the front of the eye moves up, the back moves down When the front of the eye moves right, the back of the eye moves left tangential point is called physiological insertion
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- The anterior pole of the globe is the reference point used in the description of any eye movement; When the front of the eye moves up, the back moves down When the front of the eye moves right, the back of the eye moves left Eye movements are described based on the movement of the muscle insertion towards its origin. The primary action of a muscle is its major effect when the eye is in the primary position. Subsidiary/secondary actions are the additional effects & depend on the position of the eye The point at which the center of the muscle or its tendon first touches the globe is called the tangential point and indicates the direction of the pull Muscles exert force in proportion to their cross-sectional area The power of the muscle is proportional to its length For normal amplitude of rotation (45-50 degree ) 10mm change in muscle length is required in each direction
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- As the position of the globe changes, the relationship between the muscle origin and insertion changes relative to the axes contraction of a muscle has a different effect than when the eye is in primary position
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Both obliques have same tertiary action because inserted behind the center of rotation, pull post. pole of globe medially when they contract ant.portion of eye so it causes abduction Both recti have same tertiary action bcz they inserted anterior to centre of rotation pull ant.portion of globe medially so it causes adduction • In adduction, obliques are the prime vertical movers • In abduction, recti are the prime vertical movers,
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Orientation depends solely on amount of elevation or depression and lateral rotation of the globe.
- Major physiologic principle involved in the binocular motor co-operation of the eyes Applicable to all normal ocular movements including vergence and involuntar movemens Exception: Assymmetric convergence
- Implies that the state of tension in the agonist exerts a regulatory influence on the state of tension in the antagonist and vice versa.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.
- Although the eye is responsible for transducing patterns of light energy into neuronal signals, it is the brain that is ultimately responsible for visual perception and cognition.