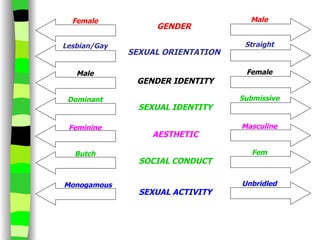
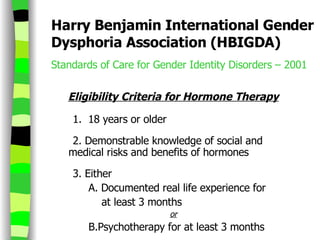
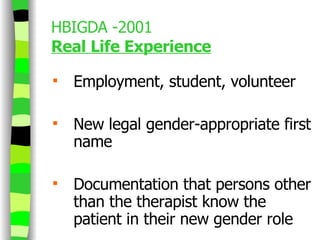
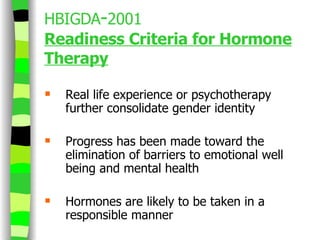
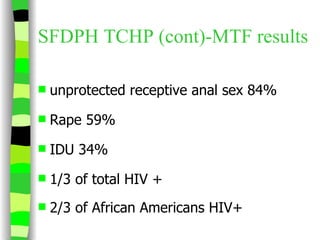
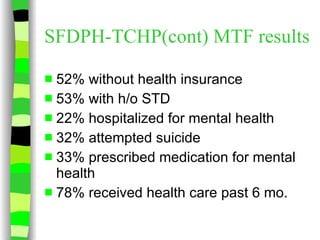
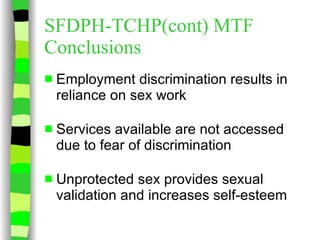
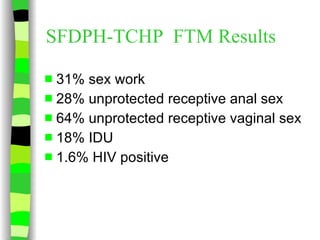
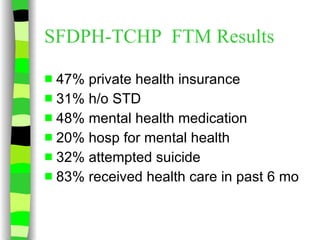
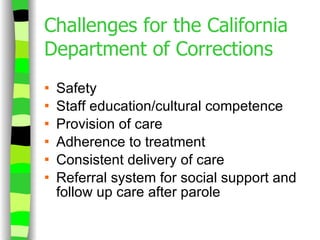
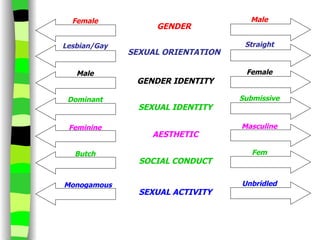
The document summarizes primary care considerations for transgender patients. It discusses clinical background, barriers to care, standards of care from organizations like HBIGDA, and models of care including hormone therapy options and risks, surgical options, screening guidelines, and challenges providing care to transgender individuals. It also presents results from studies on transgender health issues and HIV risk.