
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Drugs Affecting Coagulation
Similar to Drugs Affecting Coagulation (20)
More from Dinesh Kumar
More from Dinesh Kumar (20)
Recently uploaded
Recently uploaded (20)
Drugs Affecting Coagulation
- 1. Drugs Affecting Coagulation By Dr. Dinesh Kumar G Pharm. D
- 2. ANTICOAGULANTS I. Used in vivo A. Parenteral anticoagulants (i) Indirect thrombin inhibitors: Heparin, Low molecular weight heparins, Fondaparinux, Danaparoid (ii) Direct thrombin inhibitors: Lepirudin, Bivalirudin, Argatroban B. Oral anticoagulants (i) Coumarin derivatives: Bishydroxycoumarin (dicumarol), Warfarin sod, Acenocoumarol (Nicoumalone), Ethylbiscoumacetate (ii) Indandione derivative: Phenindione. (iii) Direct factor Xa inhibitors: Rivaroxaban (iv) Oral direct thrombin inhibitor: Dabigatran, etexilate
- 3. II. Used in vitro A. Heparin: 150 U to prevent clotting of 100 ml blood. B. Calcium complexing agents: Sodium citrate: 1.65 g for 350 ml of blood; used to keep blood in the fluid state for transfusion; ANTICOAGULANT ACID CITRATE DEXTROSE SOLUTION 2.2 g/100 ml (75 ml is used for 1 unit of blood). Sodium oxalate: 10 mg for 1 ml blood Sodium edetate: 2 mg for 1 ml blood
- 4. Heparin Heparin is a non-uniform mixture of straight chain mucopolysaccharides with MW 10,000 to 20,000. It contains polymers of two sulfated disaccharide units: D-glucosamine-L-iduronic acid D-glucosamine-D-glucuronic acid Heparin carries strong electronegative charges and is the strongest organic acid present in the body. It occurs in mast cells as a much bigger molecule (MW ~75,000) loosely bound to the granular protein. Thus, heparin is present in all tissues containing mast cells; richest sources are lung, liver and intestinal mucosa. Commercially it is produced from ox lung and pig intestinal mucosa.
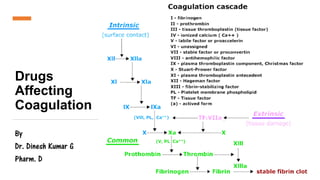
- 5. Mechanism of action • Anti thrombin III is a peptide synthesized in the liver and circulates in the plasma. • Clotting time is prolonged. Anticoagulant effect Prevents conversion of fibrinogen to fibrin Degrades thrombin, coagulation factors (Xa, IXa) Binds and activates plasma antithrombin III Heparin
- 6. PHARMACOKINETICS Heparin is a large, highly ionized molecule; not absorbed orally. Injected i.v. it acts instantaneously, but after s.c. injection anticoagulant effect develops after 60 mins. Bioavailability of s.c. heparin is inconsistent. Heparin does not cross blood-brain barrier or placenta (choice during pregnancy). It is metabolized in liver by heparinase and fragments are excreted in urine.
- 7. Dosage Heparin is conventionally given i.v. in a bolus dose of 5,000–10,000 U (children 50–100 U/kg), followed by continuous infusion of 750–1000 U/hr. Intermittent i.v. bolus doses of UFH are no longer recommended. The rate of infusion is controlled by aPTT measurement which is kept at 50–80 sec. or 1.5–2.5 times the patient’s pretreatment value. If this test is not available, whole blood clotting time should be measured and kept at ~2 times the normal value. Deep s.c. injection of 10,000–20,000 U every 8–12 hrs can be given if i.v. infusion is not possible. Needle used should be fine and trauma should be minimum to avoid hematoma formation. Hematomas are more common with i.m. injection—this route should not be used.
- 8. Dosage Low dose (s.c.) regimen 5000 U is injected s.c. every 8–12 hours, started before surgery and continued for 7–10 days or till the patient starts moving about. This regimen has been found to prevent postoperative deep vein thrombosis without increasing surgical bleeding. It also does not prolong aPTT or clotting time. However, it should not be used in case of neurosurgery or when spinal anesthesia is to be given. The patients should not be receiving aspirin or oral anticoagulants. It is ineffective in high-risk situations, e.g., hip joint or pelvic surgery.
- 9. Warfarin Prevents coagulation Coagulation factors deficiency Incomplete coagulation factor molecules formed Blocks carboxylation of glutamate residues in factors II, VII, IX, X Warfarin • Only in vivo, not in vitro. • Act indirectly by interfering with the synthesis of vit K dependent clotting factors in liver. • Competitive antagonists of vit K and lower the plasma levels of functional clotting factors in a dose-dependent manner. • Inhibit the enzyme vit K epoxide reductase (VKOR) and interfere with regeneration of the active hydroquinone form of vit K which acts as a cofactor for the enzyme γ-glutamyl carboxylase that carries out the final step of γ carboxylating glutamate residues of prothrombin and factors VII, IX and X. Dose (mg): 5 – 10
- 10. • Factor VII has the shortest plasma t½ (6 hr), its level falls first when warfarin is given, followed by factor IX (t½ 24 hr), factor X (t½ 40 hr) and prothrombin (t½ 60 hr). • Clotting factors diminishes within 2–4 hours of warfarin administration, anticoagulant effect develops gradually over the next 1–3 days as the levels of the clotting factors already present in plasma decline progressively. Thus, there is always a delay between administration of these drugs and the anticoagulant effect. Larger initial doses hasten the effect only slightly. Therapeutic effect occurs when synthesis of clotting factors is reduced by 40–50%.
- 11. Drug interactions Reduced anticoagulant action 1. Barbiturates (but not benzodiazepines), carbamazepine, rifampin and griseofulvin induce the metabolism of oral anticoagulants. The dose of anticoagulant determined during therapy with these drugs would be higher: if the same is continued after withdrawing the inducer—marked hypoprothrombinemia can occur—fatal bleeding is on record. 2. Oral contraceptives: increase blood levels of clotting factors.
- 12. Drug interactions Enhanced anticoagulant action 1. Broad-spectrum antibiotics: inhibit gut flora and reduce vit K production. 2. Newer cephalosporins (ceftriaxone, cefoperazone) cause hypoprothrombinemia by the same mechanism as warfarin —additive action. 3. Aspirin: inhibits platelet aggregation and causes g.i. bleeding—this may be hazardous in anticoagulated patients. High doses of salicylates have synergistic hypoprothrombinemia action and also displace warfarin from protein binding site. 4. Long-acting sulfonamides, phenytoin and probenecid: displace warfarin from plasma protein binding. 5. Chloramphenicol, erythromycin, celecoxib, cimetidine, allopurinol, amiodarone and metronidazole: inhibit warfarin metabolism.
- 13. USES OF ANTICOAGULANTS • Deep vein thrombosis (DVT) and pulmonary embolism (PE) • Myocardial infarction (MI) • Unstable angina • Rheumatic heart disease; Atrial fibrillation (AF) • Cerebrovascular disease • Vascular surgery, prosthetic heart valves, retinal vessel thrombosis, extracorporeal circulation, haemodialysis • Defibrination syndrome
- 14. ANTICOAGULANTS: HEPARINS DRUG NAME Unfractionated heparin; Low molecular weight heparin (LMWH): enoxaparin, dalteparin, tinzaparin MECHANISM OF ACTION Enhance the activity of antithrombin III → inhibit Factor Xa and Factor IIa (thrombin) → stop coagulation cascade INDICATIONS •Deep vein thrombosis, pulmonary embolism •Ischemic stroke, transient ischemic attack •Coronary artery disease •Cardiac valve replacement or coronary angioplasty •Dialysis and Surgical procedures: cardiopulmonary bypass, ECMO, PCI ROA Unfractionated heparin: IV, SubQ - LMWH: SubQ SIDE EFFECTS •Undue bleeding and Injection site reactions •Hyperkalemia •Heparin-induced thrombocytopenia (HIT) •Osteoporosis CONTRAINDICATIONS AND CAUTIONS •Active internal bleeding •Trauma in the past three months •History of intracranial hemorrhage or ischemic stroke or HIT •Gastrointestinal ulcers •Coagulopathies, bleeding disorders and Thrombocytopenia •Antiplatelet and thrombolytic medications (increased risk of bleeding) •Hepatic or renal disease •Alcohol use
- 15. ANTICOAGULANTS: HEPARINS ASSESSMENT AND MONITORING •Unfractionated heparin, LMWH Weight, Vital signs, Laboratory test results; CBC, PTT, aPTT, renal function tests Administration - Confirm prescribed dose per kg •Double check prescribed dose with a second nurse •Have protamine sulfate readily available •Unfractionated heparin SubQ • Inject 2 inches or 5 centimeters away from client’s navel • Pinch the skin slightly • Insert the needle at a 90 degree angle • Inject slowly • Withdraw needle; lightly press the site with dry gauze or an alcohol swab - do not massage the injection site •Monitor for signs / symptoms of bleeding; clot formation; aPTT; platelets CLIENT EDUCATION Report Signs of bleeding; e.g., oozing from the IV insertion site, nosebleed, sudden headache Signs of clot formation; e.g., new pain, swelling, or warmth in their leg; shortness of breath; sudden onset of confusion, vision changes, trouble speaking, or one-sided weakness LMWH (e.g., enoxaparin) self-administration Review appropriate technique for subcutaneous injections using prefilled syringe Inject the medication once per day, at the same time each day May feel minor discomfort or slight bruising may occur at the injection site Contact healthcare provider for signs of minor bleeding; e.g., bleeding gums, nosebleeds, longer than normal menstrual periods
- 16. ANTICOAGULANTS - WARFARIN CLASS Vitamin K antagonist MECHANISM OF ACTION •Blocks vitamin K epoxide reductase and prevent regeneration of vitamin K epoxide, which is a cofactor for the enzyme gamma-glutamyl carboxylase, which converts the non-functional forms of coagulation factors II, VII, IX, and X and anticoagulation proteins C and S, into their functional forms •Inhibits maturation of clotting factors II, VII, IX, X and anti-coagulation proteins C, S •Causes an initial period of hypercoagulation (due to protein C depletion) followed by anticoagulation INDICATIONS •Deep vein thrombosis, pulmonary embolism •Ischemic stroke, transient ischemic attack, Coronary artery disease •Cardiac valve replacement or coronary angioplasty •Coagulation disorders like antiphospholipid syndrome and DIC •Dialysis and Surgical procedures: cardiopulmonary bypass, ECMO, PCI ROA PO SIDE EFFECTS •Undue bleeding (antidote: Vitamin K1, called phytonadione) •Hair loss, Fever, Bone marrow depression •Gastrointestinal effects (anorexia, vomiting, diarrhea, abdominal cramps) •Warfarin-induced skin necrosis, purple toe syndrome •Teratogenic CONTRAINDICATIONS AND CAUTIONS •Active internal bleeding, recent trauma in the past three months, history of intracranial hemorrhage or ischemic stroke, gastrointestinal ulcers, coagulopathies or bleeding disorders •Surgery of the eye, brain, or spinal cord •Spinal anesthesia or spinal puncture, Pregnancy and breastfeeding
- 17. ASSESSMENT AND MONITORING Vital signs, signs of bleeding and Laboratory test results: CBC, PT, INR, renal and hepatic function; negative pregnancy test for female clients of childbearing age CLIENT EDUCATION •Purpose of medication: prevent clots, thromboembolism •Take exactly as directed • Contact the healthcare provider for a missed dose •Need for regular INR testing •Main side effect: bleeding •Bleeding precautions •Treatment for minor bleeding • Cuts: hold gauze or clean cloth over the affected area for 15 minutes • Nosebleed: tilt their head slightly forward; apply pressure above their nostrils for 15 minutes • Immediately notify their healthcare provider if injured, hit their head; experience bleeding longer than 15 minutes; notice blood in their vomit, stool, or urine; new onset of chest or back pain, shortness of breath, weakness, dizziness, or confusion • Dietary modifications and avoid large day-to-day variations in the amount of vitamin K • Avoid alcohol, nicotine products • Consult with healthcare provider before taking over the counter medications or supplements
- 18. Thank You