
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Approach to a patient with GI hemorrhage
Similar to Approach to a patient with GI hemorrhage (20)
Recently uploaded
Recently uploaded (20)
Approach to a patient with GI hemorrhage
- 1. “Approach to a patient with GI Hemorrhage” Dr.Bajrang Bawliya Dept. of Surgery Sir H.N. Reliance foundation hospital, mumbai DNB General surgery Resident
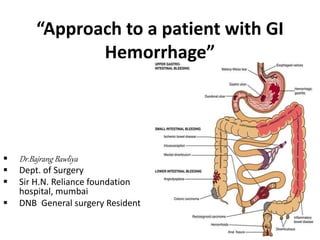
- 2. GI Haemorhage can be TRIVIAL (per rectal bleeding in case of fissure in ano) or MASSIVE (variceal bleeding) GI bleeding can occur anywhere from Mouth to Anus
- 3. Site of Bleeding Upper GI bleeding Lower GI bleeding
- 4. Forms of GI bleeding Hematemesis Vomiting of blood - s/o Upper GI bleeding a) Bright red colour b) Coffee Ground Vomitus Melena Black, Tarry, Foul smelling stool - Usually s/o Upper GI bleed - Can also be seen in Lower GI bleed Hematochezia Bright red blood may or may not be mixed with stool s/o Distal Colonic Pathology
- 5. Melena Versus Stool of patient on Iron supp. Melena – Black, Tarry, Foul smelling stool Guaiac test - Positive Greenish Black stool with h/o iron suppl. Guaiac test - Negative
- 6. Nomenclature Occult bleeding Bleeding which is not visible to patient , which is suspected when patient presents with anaemia Obscure bleeding Bleeding that PERSIST or RECUR even after negative finding in endoscopy
- 8. Approach to a patient with GI haemorrhage INITIAL ASSESSMENT AND RESUSCITATION A) Airway, Breathing and Circulation B) Magnitude of bleeding - by history and vitals C) Monitoring of vitals D) Laboratory evaluation - cbc, blood grouping and cross matching, lft, coag. profile HISTORY AND PHYSICAL EXAMINATION A) Site of bleeding - Upper/Lower GI bleed (hematemesis/melena/hematochezia) B) Cause of bleeding C) Any past history of such episode or h/o patient on any medications(NSAIDs,SSRI,Salicylates) D) Keep monitoring vitals LOCALIZE BLEEDING A) Endoscopy – EGDscopy/Colon oscopy TREATMENT OF CAUSE A) Pharmacological therapy B) Endoscopic therapy C) Angiographic therapy D) Surgery
- 9. RESUSCITATION Feeble pulse, Tachycardia, Hypotension (Hypovolemic Shock) Needs Aggressive management A) 2 large bore (16G, 18G) IV cannula B) Start Bolus fluid with Crystalloid – RL C) Foley’s Catheter – monitor urine output D) Oxygen supplementation – maximize oxygen carrying capacity E) Blood Transfusion F) FFP transfusion
- 10. Overview of a ACUTE GI HAEMORRHAGE History and Findings s/o Upper/Lower GI bleed Can put Nasogastric tube to confirm diagnosis Upper GI bleed Lower GI bleed Early Upper GI Scopy (within 24 hrs) Diagnostic Treatment accordingly Non-Diagnostic Further decision is taken depending on VOLUME of bleeding Slow bleeding Massive bleeding COLONOSCOPY ANGIOGRAPHY Diagnostic Non-Diagnostic a) RBC scan b) CT angiography c) Capsule Endoscopy Slow bleeding Massive Bleeding with stable patient ANGIOGRAPHYRBC Scan
- 12. Causes of UPPER GI Haemorrhage NON-VARICEAL bleeding (80%) VARICEAL bleeding(20%) 1) m/c – GASTRIC & DUODENAL ULCER (30-40%) 2) Gastritis/Duodenitis (20%) 3) Mallory Weiss tears (5-10%) 4) Esophagitis (5-10%) 5) A-V malformation (5%) 6) Tumor (5%) 7) Others 1) m/c – GASTRO ESOPHAGEAL VARICES (>90%) 2) Hypertensive Portal Gastropathy (<5%) 3) Isolated Gastric Varices - rare
- 13. Management of UPPER GI BLEEDING UPPER GI SCOPY Difficult to diagnosis Patient STABLE ANGIOGRAPHY UNSTABLE Non-variceal bleeding – PEPTIC ULCER Disease VARICEAL BLEEDING ENDOSCOPIC THERAPY SURGICAL INTERVENTION Diagnosis made - Due to EXCESSIVE BLOOD impairing visualization If bleeding PERSIST YES NOMonitor REBLEEDINGYES REPEAT ENDOSCOPY REBLEEDING + YES NO Monitor REBLEEDING YES SURGERY
- 14. ENDOSCOPIC THERAPY FOR PEPTIC ULCER BLEEDING 1) Inj. Adrenaline (1;10,000) is injected around bleeding ulcer f/b TAMPONADE f/b ELECTROCOAGULATION with cautery, laser or APC(Argon Plasma Coagulation) 2) If there is a visualised vessel than HEMOCLIP is used
- 15. FORREST CLASSIFICATION • It is a classification used to describe peptic ulcer and risk of rebleeding • Class 1a,1b and 2a – High risk for rebleed • Class 2b – Intermediate risk • Class 2c and 3 – low risk
- 16. Management acc. to forest classif. • Class 1a, 1b and 2a – as described earlier • Class 2b – Endoscopicaly clot is dislodged and observed • Class 2c and 3a – observed
- 17. SCORES • This scores are used to identify the individuals who are at HIGH RISK for MAJOR BLEEDING and have HIGH MORTALITY and so they need aggressive management. • The Rockall score utilizes clinical as well endoscopic findings , range- 0 to 11 ,higher score higher risk • Blatchford score ,lesser used , maimum score - 23 Blatchford score
- 19. Indication of Surgery in PUD 1. Failure of Endoscopic approach to control bleeding. 2. Recurrent hemorrhage after initial attempt of Endoscopic control. 3. Hemodynamically unstable patient inspite of receiving >6 units of blood transfusion. 4. Continuous slow bleeding with requirement of transfusion >3 units per day 5. Shock a/w Recurrent hemorrhage
- 20. Surgery done for Gastric Ulcer 1. Gastrotomy f/b Suture Ligation – has 30% chance of rebleed. 2. Simple Excision of Ulcer – as all Gastric ulcer have 10% chances of Malignancy so excision is consider better than suture ligation. Has 20% chance of rebleed. 3. Distal Gastrectomy - considered in cases of Recurrent PUD with bleeding Ulcers larger than 2 cm, posterior duodenal ulcers, and gastric ulcers have significantly higher risk of rebleeding
- 21. Surgery done for Duodenal Ulcer 1. Longitudnal duodenotomy / Duodeno-pylomyotomy f/b suture ligation - If ulcer is on posterior duodenal wall than there are high chance of REBLEED due to involvement of branches of GASTRO-DUODENAL or PANCREATICO-DUODENAL ARTERY. - For this vessel is ligated proximal as well as distal to ulcer with “U” STITCH underneath ulcer
- 23. Infectious – Herpes Esophagitis • Complaints are Melena + Anemia > Hematemesis • TOC – Endoscopic electocoagulation
- 24. Mallory Weis tears • it is a mucosal and submucosal tear seen near GE jn. along lesser curvature. • mostly seen in patient after binge alcohol drinking due to intense retching and vomitting. • Also seen in patient with multiple episode of emesis. • Rx - Usually doesn’t require any active management, sometimes may require endoscopic compression.
- 25. Dieulafoy lesion • It is a VASCULAR MALFORMATION • Seen on LESSER CURVATURE within 6cm of GE junction • Represent rupture of LARGE vessel(1-3mm) in Submucosa • TOC – Endoscopic electrocoagulation – successful in 80 % - if fails – Angiographic embolization – if fails – Gastrotomy f/b hemostasis and suturing of mucosal defect – if fails – partial gastrectomy.
- 26. GAVE – Gastric Antral Vascular Ectasia • Also k/a WATERMELON stomach due to its endoscopic appearance. • This appearance is due to DILATED VENULES in ANTRAL part of stomach converging longitudinally towards pylorus • Anemia+Melena > Hematem. • TOC – APC (Argon Plasma Coag.)
- 28. Iatrogenic causes Post Procedural- • Nasogastric tube erosions,endoscopic biopsy,endoscopic polypectomy,endoscopic sphincterectomy • Percutenous endoscopic gastrotomy (PEG) • Percutenous transhepatic procedures
- 30. VARICEAL BLEEDING suspected ABC ensured and Resuscitation done Start on OCTREOTIDE Infusion Upper GI scopy Variceal bleeding diagnosis confirmed Endoscopic Band ligation > Sclerotherapy (SE-Stricture, perforation, mediastinitis) Bleeding Stopped Balloon tamponade (sengstaken – blakemore tube) or Self expanding Esophageal Stents are used TIPS (Transjugular Intrahepatic Portosystemic Shunt • Continue Octreotide • Continue IV antibiotics • Repeat Band Ligation after 14 days YES NO Still bleeding
- 31. Endoscopic Procedures Band Ligation Sclerotherapy Sclerosant – Ethanolamine, Sodium tetradecyl Sulphate
- 32. Balloon tamponade it is done with SENSTAKEN BLAKEMORE tube
- 34. Portal Hypertensive Gastropathy • It is a disease involving diffuse gastric mucosa making it friable with ectatic blood vessel at some places • Shows Mosaic pattern and snake skin-like appearance with cherry-red spots on Endoscopy • Difficult to manage endoscopically due to diffuse nature of disease • TOC – PPI , if fails than TIPS is the only option
- 37. Causes of LOWER GI Haemorrhage COLONIC pathology(95%) SMALL BOWEL pathology (5%) 1) m/c – DIVERTICULA (30-40%) 2) Ano-rectal disease (10-15%) 3) Ischemia (5-10%) 4) Neoplasia (5-10%) 5) Infectious colitis(3-8%) 6) IBD (3-5%) 7) Angiodysplasia (3%) 8) Radiation Proctitis (1-3%) 9) Others (1-5%) 10) Unknown – (10-25%) 1) Angiodysplasia 2) Meckels Diverticulum 3) Ulcers/erosions 4) Chrons 5) Radiation 6) Neoplasm 7) Aorto-enteric fistula
- 38. Colonic Diverticula- m/c cause of lower GI bleed • m/c on LEFT colon • But RIGHT bleeds>left • Bleeding is from NECK of diverticula • 75% bleed stops spontaneously • TOC – Colonoscopic injection of Adr. +/- electocoagulation +/- clip -- if fails – Angiography f/b embolization – if fails – Exploration with colonic resection • Mesenteric Angiography Selective angiography, using either the superior or inferior mesenteric arteries, can detect hemorrhage in the range of 0.5 to 1.0 mL/min and is generally employed only in the diagnosis of ongoing hemorrhage. It can be particularly useful in identifying the vascular patterns of angiodysplasias. It may also be used for localizing actively bleeding diverticula.
- 39. Ano rectal pathology causing Lower GI Bleeding • Anal fissures-rarely cause large amount of blood loss,bleeding usually ceases spontaneously • Hamorrhoids- 2-9 % cases of lower GI bleed ,fresh blood seen on tissue paper or bowl and around the stools.Mx-Rubber band ligation,injection Sclerotherapy,infrared coagulation ,in refractory cases surgical haemrrhodectomy • Solitory rectal ulcers- arises as result of local ischemia due t internal rectal prolapse , rarely causes bleeding • Anorectal varices-arise in patients of portal hypertension and can bleed in 18 % of those patients • Colorectal Neoplasia
- 40. Obscure Lower GI bleeding • Bleeding persisting or recurring after negative esophagogastroscopy and colonoscopy occurs in approximately 5 % of cases is termed oscure bleeding • Often result due to angiodyplastic lesions,Dieulafoy’s lesions , Mekel’s Diverticula ,small bowel Neoplasm
- 41. Investigations used in neg. Colonoscopy 1. Radionuclide tagged RBC scan • Patient’s RBC’s are withdrawn from the patient and labelled with Tc-99 and Re-injected in patient. • Most sensitive but less accurate • Labelled RBC’s extravasates in Bowel and detected on scan • Diagram – shows filling of bulbous structure, probably caecum at 20 min
- 42. 2.ENTEROSCOPY / SMALL BOWEL ENDOSCOPY • Initially scope which were available were limited upto 50-70 cm from ligament of Treitz. • Nowadays DOUBLE- BALLOON endoscopy is used to visualize whole of the small bowel
- 43. 3. CT - Enterography • It is CT scan after giving Oral conrast with IV contrast 4. Small bowel Enteroclysis • Here contrast is given through tube, movement of contrast dye is visualised • Not done nowadays
- 44. 5. Video Capsule Endoscopy • A small capsule which has video camera in it is given to patient to swallow and images are taken all through the parts of bowel. • It is patient friendly but time consuming and non-therapeutic
- 45. 6. Intra-operative endoscopy • Reserved for patient to diagnose bleeding intraoperatively in an hemodynamically unstable patient.