
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Syphilis 2018
Similar to Syphilis 2018 (20)
More from BMCStudents
More from BMCStudents (20)
Recently uploaded
Recently uploaded (20)
Syphilis 2018
- 1. 1 SYPHILIS Urinary system Module HUMAM OMER ABDUL-LATEEF STAGEND2 UNIVERSITY OF BAGHDAD COLLEGE OF MEDICINE
- 2. 2 Contents: 1.Introduction ……………..…………………...……... 3 2.Search board and Discussion Definition and transmission ……………..…...... 5 History ……………………………………...…... 6 Etiology …………………………………………. 9 Signs and symptoms ………………………….. 10 Diagnosis ……………………………………..... 11 Treatment …………………………………...… 14 Epidemiology and prognosis …………………. 16 Prevention …………...………………………... 17 3.Summary ……………………………………...…… 18 4.References …………………………………….…… 19 5.Figures' references …………………………..……. 21
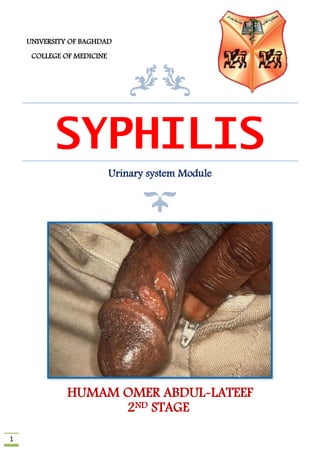
- 3. 3 Introduction Syphilis is a sexually transmitted disease (STD) caused by an infection with spirochete bacteria known as Treponema pallidum. Like other STDs, syphilis can be spread by any type of sexual contact. Syphilis can also be spread from an infected mother to the fetus during pregnancy or to the baby at the time of birth. The signs and symptoms of syphilis vary depending in which of the four stages it presents (primary, secondary, latent, and tertiary). [38] The primary stage classically presents with a single chancre (a firm, painless, non-itchy skin ulceration) but there may be multiple sores. [1] In secondary syphilis a diffuse rash occurs, which frequently involves the palms of the hands and soles of the feet. [1,2] There may also be sores in the mouth or vagina. [1] In latent syphilis, which can last for years, there are few or no symptoms. [1] In tertiary syphilis there are gummas (soft non-cancerous growths Syphilis has been described for centuries. It can cause long-term damage to different organs if not properly treated). Figure 1: Chancre on glans and vagina is one of the signs of Syphilis disease.
- 4. 4 Definition and Transmission Ways A chronic infectious disease caused by Treponema pallidum, either transmitted by direct contact, usually in sexual intercourse, or passed from mother to child in utero, and progressing through three stages characterized respectively by local formation of chancres, ulcerous skin eruptions, and systemic infection that leads to general paresis. [2] Syphilis has both acute and chronic forms that produce a wide variety of symptoms affecting most of the body's organ systems. The range of symptoms makes it easy to confuse syphilis with less serious diseases and ignore its early signs. Acquired syphilis has four stages (primary, secondary, latent, and tertiary) and can be spread by sexual contact during the first three of these four stages. Syphilis, which is also called lues (from a Latin word meaning plague), has been a major public health problem since the sixteenth century. The disease was treated with mercury or other ineffective remedies until World War I, when effective treatments based on arsenic or bismuth were introduced. These were succeeded by antibiotics after World War II. At that time, the number of cases in the general population decreased, partly because of aggressive public health measures. This temporary decrease, combined with the greater amount of attention given to AIDS in recent years, leads some people to think that syphilis is no longer a serious problem. In actual fact, the number of cases of syphilis in the United States has risen since 1980. This increase affects both sexes, all races, all parts of the nation, and all age groups, including adults over 60. The number of women of childbearing age with syphilis is the highest that has been recorded since the 1940s. About 25,000 cases of infectious syphilis in adults are reported annually in the United States. It is estimated, however, that 400,000 people in the United States need treatment for syphilis every year, and that the annual worldwide total is 50 million persons. In 1999, the Centers for Disease Control and Prevention (CDC) joined several other federal agencies in announcing the "National Plan to Eliminate Syphilis in the United States." Eliminating the disease was defined as the absence of transmission of the disease; that is, no transmission after 90 days following the report of an imported index case. The national goals for eliminating syphilis include bringing the annual number of reported cases in the United States below 1000, and increasing the number of syphilis-free counties to 90% by 2005. In November 2002, the CDC released figures for 2000–2001, which indicate that the number of reported cases of primary and secondary syphilis rose slightly. This rise, however, occurred only among men who have sex with other men. The CDC also stated that the number of new cases of syphilis has actually declined among women as well as among non-Hispanic blacks. [3] The increased incidence of syphilis since the 1970s is associated with drug abuse as well as changes in sexual behavior. The connections between drug abuse and syphilis include needle sharing and exchanging sex for drugs. In addition, people using drugs are more likely to engage in risky sexual practices. As of 2002, the risk of contracting syphilis is particularly high among those who abuse crack cocaine. With respect to changing patterns of conduct, a sharp increase in the number of people having sex with multiple partners makes it more difficult for public health doctors to trace the contacts of infected persons. Women are not necessarily protected by having sex only
- 5. 5 with other women; in the past few years, several cases have been reported of female-to- female transmission of syphilis through oral-genital contact. In addition, the incidence of syphilis among men who have sex with other men continues to rise. Several studies in Latin America as well as in the United States reported in late 2002 that unprotected sexual intercourse is on the increase among gay and bisexual men. Changing patterns of sexual behavior have led to a striking increase in the number of cases of syphilis in eastern Europe since the collapse of the Soviet Union; Slovenia reported an 18-fold increase in reported cases of syphilis just between 1993 and 1994. Over half of the new cases were linked to a source of infection in another European country. [4] In general, high-risk groups for syphilis in the United States and Canada include: sexually active teenagers people infected with another sexually transmitted disease (STD), including AIDS sexually abused children women of childbearing age prostitutes of either sex and their customers prisoners persons who abuse drugs or alcohol The chances of contracting syphilis from an infected person in the early stages of the disease during unprotected sex are between 30-50%. Figure 2: The ways of syphilis's transmission
- 6. 6 History The first known case of syphilis was documented by Dr. Pintor in 1493 in Rome. He called it the Morbus Gallicus (The French Disease), and assumed that it had been carried to Italy by the French Army. When the French began to notice it, they called it mal de Naples (the sickness of Naples). Emperor Maximilian officially referred to it as malum franciscum in 1495, but soon it was known by an altogether simpler name: The Pox. It was called this because of the noticeable effects the disease had on the skin of the afflicted, leaving lesions and decaying soft tissues that were sometimes mistaken for leprosy. The name syphilis comes from a Greek legend about a peasant Apollo had punished with poor health and lesions all over his body: the peasant’s name was Syphilus, and he could only be cured (rather chillingly) by Mercury. [5] It is generally believed that Columbus had brought the disease back with him from the Americas. It existed in the Americas before Columbus arrived, and the timing certainly was convenient. Some Renaissance thinkers suspected it had something to do with astrology (see right and above left), while others thought it was derived from leprosy. Francis Bacon believed that it was a result of cannibalism. [5] The oldest artistic representation of syphilis is considered one on a Peruvian jug dating back to VIth century, depicting a mother suffering from syphilis holding a child in her arms; the mother shows a saddle nose and superior incisive teeth with notches on their free margins. The piece belongs to a collection of jugs also encompassing two jugs illustrating leprosy and leishmaniasis. [6] Albrecht Dürer, a German artist, depicts in woodcuts, for the first time in Europe, in 1496, the image of a mercenary whose skin bears sores of multiple chancres (Fig. 3). Next to the image lays written a text by physician Theodorus Ulsenius warning on the new disease, also describing its signs and symptoms, mentioning that the illness is not curable and establishing a direct link between the epidemic and the grand astrological conjuction in 1484 [6,7] Figure 3: A mercenary whose skin presents multiple chancres, woodcut by Albrecht Dürer, 1496 –published in a Romanian book in 1933
- 7. 7 From the very beginning numerous theories on the origin of syphilis existed, most of which linking initially syphilis and leprosy together. According to several fables of the early XVI th century, syphilis was the result of a sexual relation between a Spanish prostitute and a leper. The prostitute also infected the soldiers of Charles VIII. Paracelsus (1493-1541) considered that syphilis was the result of a sexual intercourse between a prostitute suffering from gonorrhea and a French leper. In compliance to other theories of the time, the disease might have been the outcome of the relationship of a prostitute having a uterine abscess with a leper or the result of poisoning the wine with blood coming from a leper [8] . Sexual transmitted diseases were seen as a single disease for many centuries. The differentiation between gonorrhea, cancroids and syphilis as distinct maladies was achieved no earlier than XIXth century. In the beginning of XVIIIth century there were several doctors who treated syphilis and gonorrhea as separate entities. However, in 1767 John Hunter a famous physician of venereal diseases at that time (1728-1793) conducted an experiment consisting of an inoculation of the urethral secretion of a gonorrhea patient in the prepuce of a healthy patient, the last developing syphilis shortly afterwards. Consequently, his experiment proved that syphilis resulted from gonorrhea. What Hunter has missed out was that the patient from whom the urethral secretion was taken had both syphilis and gonorrhea. However, his experiment, widely acknowledged in his époque, delayed the differential diagnosis of the two diseases with a few decades [9,10] . In 1831 Ricord has designed a larger study on syphilis and gonorrhoea and succeeded to show that the last occurs only after contact with gonorrohea patients, whilst the former – only after contact with syphilis patients [9] . It was not earlier than 1905 that Schaudinn (1871-1906) and Hoffman (1868 – 1959) have discovered the etiologic agent of syphilis, whom they have named Spirochaeta pallida, on various syhilis lesions, proving its existence in both fresh and Giemsa coloured specimens. It was them who changed the name of the bacterium subsequently to Treponema pallidum [9,11,12] . In 1906 Landsteiner introduced the use of the dark-field microscopy method for the detection of the spirochete of syphilis. In 1910 the German bacteriologist August Wasserman (1866-1925) came with the first serologic test for syphilis and in 1949 Nelson and Mayer have conceived Treponema pallidum immobilization test (TPI), the first specific test for T. pallidum [11,13] . Their discoveries had a very important role in detecting the disease in patients who were suspected of syphilis, as well as in other healthy individuals, and in monitoring syphilis response to treatment. Syphilis treatments along the history Initially, the treatment of syphilis included less efficient methods that were accompanied by pain and multiple adverse reactions [11] . Taking into consideration that the disease was associated with the discovery of the American continent, numerous treatments included plants brought from the New World, such as the guaiac tree (lat. Guaiacum Officinale),
- 8. 8 known also as sasafras or willow (Salix), which led to the widest recognition at the time (Fig. 4). These plants acted as purgative agents, lead to sudoration, diarrhea and the increase in urinary debt and were believed to be “blood cleansers” [9] . One of the main supporters of the guaiac tree utilisation in the treatment of syphilis, and in the same time an ardupus opponent of mercury treatment, was Ulrich von Hutten (1488-1523), a former priest who described in a detail the manifestations of the disease as well the simptoms of mercury intoxication, based on his own experience as a sufferrer from the disease [14,15] . From the guaiac tree a decoction was made, the resulted potion was boiled and the patient was assumed to consume the mixture daily for 30 days. Before drinking the potion, the patient was covered in blankets in order to induce perspiration, and a mild purgative was also administered [14] . German scientist Paul Ehrlich (1854-1915) received Nobel Prize in Physiology and Medicine in 1908 for his discovery of arsphenamine (Salvarsan). The scientist discovered the compound that acted like an antibiotic by accident, while working on finding a cure for Trypanosoma brucei. Ehrlich’s desire was to discover a “magical bullet”- a drug able to specifically bind to a bacterium and kill it, without affecting human cells. Salvarsan was also denominated as “Compound 606”, as it was discovered after 606 failed experiments (Fig. 5) [9] . The safer novel drug that superseded the more toxic and less water-soluble salvarsan as a treatment for syphilis was Neosalvarsan, also an arsenic compound. Both Salvarsand and Neosalvarsan were replaced in the treatment of syphilis by Penicillin, after 1940. Figure 4: Guaiacum officinale (guaiac tree), used widely for the treatment of syphilis Figure 5: The laboratory in which famous 606 compound was invented
- 9. 9 Etiology The cause of syphilis is infection with the spirochete T pallidum.T pallidum is solely a human pathogen and does not naturally occur in other species. T pallidum has, however, been cloned in Escherichia coli and has been used experimentally in rabbits. Transmission of T pallidum occurs via penetration of the spirochetes through mucosal membranes and abrasions on epithelial surfaces. It is primarily spread through sexual contact but can be spread by exposure to blood products and transferred in utero. T pallidum is a labile organism that cannot survive drying or exposure to disinfectants; thus, fomite transmission (eg, from toilet seats) is virtually impossible. Unprotected sex is the major risk factor for the acquisition of syphilis, especially among men who have sex with men (MSM), who accounted for 83.7% of all syphilis cases in the United States. [16] There are two causes for syphilis disease which are: Bacteriology Treponema pallidum subspecies pallidum is a spiral-shaped, Gram-negative, highly mobile bacterium. [17] Three other human diseases are caused by related Treponema pallidum subspecies, including yaws (subspecies pertenue), pinta (subspecies carateum) and bejel (subspecies endemicum). Unlike subtype pallidum, they do not cause neurological disease. Humans are the only known natural reservoir for subspecies pallidum. It is unable to survive more than a few days without a host. This is due to its small genome (1.14 Mbp) failing to encode the metabolic pathways necessary to make most of its macronutrients. It has a slow doubling time of greater than 30 hours. [17] Transmission Syphilis is transmitted primarily by sexual contact or during pregnancy from a mother to her fetus; the spirochete is able to pass through intact mucous membranes or compromised skin. [18] It is thus transmissible by kissing near a lesion, as well as oral, vaginal, and anal sex. Approximately 30% to 60% of those exposed to primary or secondary syphilis will get the disease. Its infectivity is exemplified by the fact that an individual inoculated with only 57 organisms has a 50% chance of being infected. [17] Most (60%) of new cases in the United States occur in men who have sex with men. Syphilis can be transmitted by blood products, but the risk is low due to blood testing in many countries. The risk of transmission from sharing needles appears limited. It is not generally possible to contract syphilis through toilet seats, daily activities, hot tubs, or sharing eating utensils or clothing. This is mainly because the bacteria die very quickly outside of the body, making transmission by objects extremely difficult. [19]
- 10. 10 Signs and symptoms The first symptoms of syphilis can take 10 days to 3 weeks to appear after infection. The most common symptom is a painless sore that appears where the virus was transmitted - normally on the penis, vagina or anus. Your lymph glands (in the neck, groin or armpit) may also swell. [38] The sore will disappear in 2-6 weeks. However, if the infection itself is not treated, it will move to the second stage. You can't diagnose syphilis by looking at pictures because symptoms vary from person to person. If you think you have syphilis, see your doctor or healthcare worker as soon as possible. [20] Symptoms of secondary syphilis begin a few weeks after the disappearance of the sore and include: a non-itchy skin rash small skin growths on the vulva (in women) and around the anus (in both men and women) flu-like symptoms such as tiredness, headaches, joint pains and fever swollen lymph glands weight loss hair loss. These symptoms may disappear within a few weeks, or come and go over a period of months. Without treatment, syphilis becomes 'latent' whereby you do not experience any symptoms even though you remain infected. This stage can happen for years, even decades and there is a danger of moving onto the most dangerous stage - tertiary syphilis. [21] A third of people who are not treated for syphilis develop serious symptoms at this stage including: Fig (6): A maculopapular rash is pre- sent on the palm stroke dementia loss of co-ordination numbness paralysis blindness deafness heart disease skin rashes. At this stage, syphilis can also cause death. This is why it is important to see a healthcare professional and get tested and treated in the early stages of syphilis. [21]
- 11. 11 Diagnosis Patient history and physical diagnosis The diagnosis of syphilis is often delayed because of the variety of early symptoms, the varying length of the incubation period, and the possibility of not noticing the initial chancre. Patients do not always connect their symptoms with recent sexual contact. They may go to a dermatologist when they develop the skin rash of secondary syphilis rather than to their primary care doctor. Women may be diagnosed in the course of a gynecological checkup. Because of the long-term risks of untreated syphilis, certain groups of people are now routinely screened for the disease: [39] pregnant women sexual contacts or partners of patients diagnosed with syphilis children born to mothers with syphilis patients with HIV infection persons applying for marriage licenses When the doctor takes the patient's history, he or she will ask about recent sexual contacts in order to determine whether the patient falls into a high-risk group. Other symptoms, such as skin rashes or swollen lymph nodes, will be noted with respect to the dates of the patient's sexual contacts. Definite diagnosis, however, depends on the results of laboratory blood tests. [22] Blood tests There are several types of blood tests for syphilis presently used in the United States. Some are used in follow-up monitoring of patients as well as diagnosis. NONTREPONEMAL ANTIGEN TESTS. Nontreponemal antigen tests are used as screeners. They measure the presence of reagin, which is an antibody formed in reaction to syphilis. In the venereal disease research laboratory (VDRL) test, a sample of the patient's blood is mixed with cardiolipin and cholesterol. If the mixture forms clumps or masses of matter, the test is considered reactive or positive. The serum sample can be diluted several times to determine the concentration of reagin in the patient's blood. The rapid plasma reagin (RPR) test works on the same principle as the VDRL. It is available as a kit. The patient's serum is mixed with cardiolipin on a plastic-coated card that can be examined with the naked eye. Nontreponemal antigen tests require a doctor's interpretation and sometimes further testing. They can yield both false-negative and false-positive results. False-positive results can be caused by other infectious diseases, including mononucleosis, malaria, leprosy, rheumatoid arthritis, and lupus. HIV patients have a particularly high rate (4%, compared to 0.8% of HIV-negative patients) of false-positive results on reagin tests. False-negatives can occur when patients are tested too soon after exposure to syphilis; it takes about 14-21 days after infection for the blood to become reactive. TREPONEMAL ANTIBODY TESTS. Treponemal antibody tests are used to rule out false-positive results on reagin tests. They measure the presence of antibodies that are specific for T. pallidum. The most commonly used tests are the microhemagglutination-T. pallidum (MHA-TP) and the fluorescent treponemal antibody absorption (FTA-ABS)
- 12. 12 tests. In the FTA-ABS, the patient's blood serum is mixed with a preparation that prevents interference from antibodies to other treponemal infections. The test serum is added to a slide containing T. pallidum. In a positive reaction, syphilitic antibodies in the blood coat the spirochetes on the slide. The slide is then stained with fluorescein, which causes the coated spirochetes to fluoresce when the slide is viewed under ultraviolet (UV) light. In the MHA-TP test, red blood cells from sheep are coated with T. pallidum antigen. The cells will clump if the patient's blood contains antibodies for syphilis. Treponemal antibody tests are more expensive and more difficult to perform than nontreponemal tests. They are therefore used to confirm the diagnosis of syphilis rather than to screen large groups of people. These tests are, however, very specific and very sensitive; false-positive results are relatively unusual. INVESTIGATIONAL BLOOD TESTS. Currently, ELISA, Western blot, and PCR testing are being studied as additional diagnostic tests, particularly for congenital syphilis and neurosyphilis. [23] Other laboratory tests MICROSCOPE STUDIES. The diagnosis of syphilis can also be confirmed by identifying spirochetes in samples of tissue or lymphatic fluid. Fresh samples can be made into slides and studied under darkfield illumination. A newer method involves preparing slides from dried fluid smears and staining them with fluorescein for viewing under UV light. This method is replacing darkfield examination because the slides can be mailed to professional laboratories. SPINAL FLUID TESTS. Testing of cerebrospinal fluid (CSF) is an important part of patient monitoring as well as a diagnostic test. The VDRL and FTA-ABS tests can be performed on CSF as well as on blood. An abnormally high white cell count and elevated protein levels in the CSF, together with positive VDRL results, suggest a possible diagnosis of neurosyphilis. CSF testing is not used for routine screening. It is used most frequently for infants with congenital syphilis, HIV-positive patients, and patients of any age who are not responding to penicillin treatment. [24] Figure 7
- 13. 13 Table 1: Presentations and features of the phases of syphilis [25] Stage Features Primary syphilis (10- 90 days afterinitial in fection) Skin: papule develops at site of initial infection; undergoes ulceration to form apainless, firm chancre Lymphatics: painless regional lymphadenopathy Duration: lesion heals spontaneously in 2-3 weeks Comment: cervical and rectal lesions may go unnoticed Secondary syphilis (4 - 10 weeks afterappea rance of primary lesi on) Constitutional illness: fever, sore throat, malaise and arthral gia; inflammation of manyorgans, e.g. hepatitis, nephritis, a rthritis Skin: generalized papular, non- itchy rash involving plantar and palmar skin, butexcluding t he face; condylomata lata; oral and genital snail track ulcers Lymphatics: generalized lymphadenopathy Duration: signs subside in 3- 12 weeks, but 20% of cases show recurrent symptomsover 1 -2 years Tertiary syphilis (3- 30 years aftersecond ary stage has passed) Widely varying signs and symptoms Skin: granulomatous and ulcerating lesions (gumma) often developing at sites oftrauma Bone: gumma- like lesions develop in any bone causing local pain and path ologicalfracture Viscera: gumma- like lesions of the gastrointestinal tract, especially in the liv er, withresultant dysfunction Cardiovascular: aortitis and aortic aneurysm Neurosyphilis: aseptic meningitis, tabes dorsalis, general pa ralysis of the insane;Argyll Robertson pupils Congenital syphilis Early signs show at age 2-6 weeks, and include: Skin: chronic catarrhal inflammation of mucous membranes Failure to thrive Late signs show at 2+ years and include: Skin eruptions Corneal keratitis (corneal deposits) Tooth deformity: peg (Hutchinson) incisors, multicusped (m ulberry) molars Collapse of nasal cartilage (saddle nose) Bone deformity Neurosyphilis
- 14. 14 Treatment Approach Considerations Key principles for the treatment of syphilis include the following: [26] Penicillin is the drug of choice to treat syphilis. Doxycycline is the best alternative for treating early and late latent syphilis. Syphilis associated with HIV infection does not require any enhanced antimicrobial therapy. In the treatment of late syphilis by weekly injections, missing a dose of penicillin for a period of 10-14 days does not require restarting the entire course of injections. The exception to this is in the case of pregnant women in whom there is no latitude for missing a dose of penicillin. There is evidence that an interval of 7-9 days between doses may produce better results. CSF testing to detect neurosyphilis is strongly recommended in patients with tertiary syphilis or with neurological signs or symptoms consistent with neurosyphilis and in patients without symptoms whose serologic titers do not decline appropriately after being treated with recommended therapy. Reinfection rates among MSM are high, so frequent serological testing in this group is recommended. CDC recommends the use of the RPR-based screening algorithm. When there is a low epidemiologic risk or clinical probability of syphilis, the positive predictive value of an isolated unconfirmed reactive treponemal chemoluminescence test or enzyme immunoassay is low. Antibiotic Therapy Penicillin Penicillin was established as an effective treatment for syphilis before the widespread use of randomized clinical trials. [26] The treatment guidelines published by the CDC (see current CDC recommendations) are based largely on uncontrolled trials and expert opinion. Guidelines are based on staging, with later stages requiring longer courses of treatment due to the slower rate of bacterial replication. [27] Penicillin remains the mainstay of treatment and the standard by which other modes of therapy are judged. [28] The 2015 CDC STD treatment guidelines support the use of penicillin as the preferred drug for treating all stages of syphilis. [19] Penicillin is the only recommended therapy for neurosyphilis, congenital syphilis, or syphilis during pregnancy. Rarely, T pallidum has been found to persist following adequate penicillin therapy; however, there is no indication that the organism has acquired resistance to penicillin. The following regimens are recommended for penicillin treatment: Primary or secondary syphilis - Benzathine penicillin G 2.4 million units intramuscularly (IM) in a single dose Early latent syphilis - Benzathine penicillin G 2.4 million units IM in a single dose Late latent syphilis or latent syphilis of unknown duration - Benzathine penicillin G 7.2 million units total, administered as 3 doses of 2.4 million units IM each at 1-week intervals
- 15. 15 Pregnancy - Treatment appropriate to the stage of syphilis is recommended. Clinicians should be aware that only benzathine penicillin product (Bicillin L-A) should be used, not benzathine-procaine penicillin (Bicillin C-R). In addition, oral penicillin is never appropriate for the treatment of syphilis. If the patient arrives late for subsequent doses, clinical experience suggests that an interval of 10-14 days between doses of benzathine penicillin for latent syphilis might be acceptable before restarting the sequence of injections; however, according to pharmacokinetics/pharmacodynamics, an interval of 7-9 days between doses is more optimal. [29, 30, 31] In pregnancy, missed doses are not acceptable. Pregnant patients must repeat the full course of therapy. [28] In patients with a history of penicillin allergy, desensitization may be necessary in cases of pregnancy, neurosyphilis, congenital syphilis, or tertiary syphilis. According to the 2015 CDC STD guidelines, no treatment regimens for syphilis have been shown to be more effective in preventing neurosyphilis in patients who are HIV positive than the syphilis regimens recommended for patients who are HIV negative. Careful monitoring after therapy is required, as patients with HIV infection are at higher risk for reinfection and have a slower serologic response than patients without HIV infection. [32] Alternatives to penicillin As stated in the 2015 CDC guidelines, several therapies exist that might be effective in nonpregnant, penicillin-allergic patients with primary or secondary syphilis. [32] Surgical Care Surgical care is reserved for treating the complications of tertiary syphilis (eg, aortic valve replacement). Table 2
- 16. 16 Epidemiology and Prognosis In 2012, about 0.5% of adults were infected with syphilis, with 6 million new cases. In 1999 it is believed to have infected 12 million additional people, with greater than 90% of cases in the developing world. It affects between 700,000 and 1.6 million pregnancies a year, resulting in spontaneous abortions, stillbirths, and congenital syphilis. During 2010, it caused about 113,000 deaths, down from 202,000 in 1990. In sub-Saharan Africa, syphilis contributes to approximately 20% of perinatal deaths. Rates are proportionally higher among intravenous drug users, those who are infected with HIV, and men who have sex with men. In the United States, rates of syphilis as of 2007 were six times greater in men than women; they were nearly equal in 1997. African Americans accounted for almost half of all cases in 2010. As of 2014, syphilis infections continue to increase in the United States. [33] Syphilis was very common in Europe during the 18th and 19th centuries. Flaubert found it universal among nineteenth-century Egyptian prostitutes. In the developed world during the early 20th century, infections declined rapidly with the widespread use of antibiotics, until the 1980s and 1990s. Since 2000, rates of syphilis have been increasing in the USA, Canada, the UK, Australia and Europe, primarily among men who have sex with men. Rates of syphilis among American women have remained stable during this time, while rates among UK women have increased, but at a rate less than that of men. Increased rates among heterosexuals have occurred in China and Russia since the 1990s. This has been attributed to unsafe sexual practices, such as sexual promiscuity, prostitution, and decreasing use of barrier protection. [33] Untreated, it has a mortality rate of 8% to 58%, with a greater death rate in males. The symptoms of syphilis have become less severe over the 19th and 20th centuries, in part due to widespread availability of effective treatment, and partly due to virulence of the spirochaete. With early treatment, few complications result. Syphilis increases the risk of HIV transmission by two to five times, and coinfection is common (30–60% in some urban centers). In 2015, Cuba became the first country in the world to eradicate mother to child transmission of syphilis. Figure 8
- 17. 17 Prevention Syphilis is an infectious disease but it is preventable to a large extent. The best and the most certain method of prevention of this infection is to avoid sexual contact or only to maintain sexual contact with one faithful partner who has been tested and is not infected. Some of the tips to prevent transmission of syphilis include the safe sex measures. [34] Safer sex Safer sex measures include: Having sex with a single faithful, tested and non-infected partner. Sexual penetration or ejaculation does not need to take place for syphilis to spread. Condoms can be used to reduce the risk of catching syphilis, but cannot prevent it altogether. Some risk remains via exposure to the mouth (those having oral sex) or via anus (those having anal intercourse). It is important to use a condom during vaginal, oral and anal sex. Other forms of barriers like use of a dental dam (square of plastic) when having oral sex or when the mouth of an uninfected individual makes contact with partner's vagina or anus. This also prevents transmission of sexually transmitted infection (STI). Sex toys that have been used by another individual (possibly infected) should not be shared. For people who wish to use them can wash them after each use and use a fresh condom over them. [35] Syphilis and injection drug users Syphilis can also spread by sharing injection drug users. Injection drug users should avoid sharing needles. They can opt for needle-exchange programmes that are offered by many pharmacies and local authorities. In these used needles can be exchanged for new disposable clean ones. [36] Treatment of sexual partner Transmission needs to be prevented by routine testing and, if positive, treatment of sexual partners of infected individuals. The infected individuals are counselled regarding prevention of spread to their sexual partners. Individuals sexually exposed to a person with primary, secondary, or early latent syphilis within 90 days preceding the diagnosis should be assumed to be infected. All sexual partners of the infected person in the recent past need to be identified, notified and rapidly referred for medical evaluation and treatment. Long- term sex partners of patients with late syphilis should be evaluated clinically and serologically and treated appropriately. All patients with syphilis should be tested for HIV. Patient and partner education is important. [37] Figure 9
- 18. 18 Summary Treponema pallidum infection in men not only provoked a disease that represented a threat to humans for many centuries, but it also had a tumultuous history. From examining it, one could learn how easy was to place stigma not only on individuals affected by the disease, but on entire nations, as countries were blamed along the history for the spread of the disease. Throughout the centuries, syphilis has affected individuals of various origins, from monarchs, painters and philosophers to low income people, mainly due to promiscuity. Various treatments to cure the disease were tried along the centuries; nowadays, penicillin and prevention programs control the disease. Syphilis is difficult to diagnose clinically early in its presentation. Confirmation is either via blood tests or direct visual inspection using microscopy. Blood tests are more commonly used, as they are easier to perform. Diagnostic tests are unable to distinguish between the stages of the disease. Congenital syphilis is that which is transmitted during pregnancy or during birth. Two- thirds of syphilitic infants are born without symptoms. Common symptoms that develop over the first couple of years of life include enlargement of the liver and spleen (70%), rash (70%), fever (40%), neurosyphilis (20%), and lung inflammation (20%). If untreated, late congenital syphilis may occur in 40%, including saddle nose deformation, Higoumenakis sign, saber shin, or Clutton's joints among others. Infection during pregnancy is also associated with miscarriage. The signs and symptoms of syphilis vary depending in which of the four stages it presents (primary, secondary, latent, and tertiary). The primary stage classically presents with a single chancre (a firm, painless, non-itchy skin ulceration) but there may be multiple sores. In secondary syphilis a diffuse rash occurs, which frequently involves the palms of the hands and soles of the feet. There may also be sores in the mouth or vagina. In latent syphilis, which can last for years, there are few or no symptoms. In tertiary syphilis there are gummas (soft non-cancerous growths), neurological, or heart symptoms. Syphilis has been known as "the great imitator" as it may cause symptoms similar to many other diseases. Syphilis can be cured with the right antibiotics. However, treatment will not undo any damage that the infection has already caused.
- 19. 19 References 1- "Syphilis - CDC Fact Sheet (Detailed)". CDC. 2 November 2015. Archived from the original on 6 February 2016. Retrieved 3 February 2016. 2- "Syphilis". CDC. 4 June 2015. Archived from the original on 21 February 2016. Retrieved 3 February 2016. 3- Cuba, part of a regional initiative led by PAHO and WHO to eliminate vertical transmission of HIV and syphilis, achieved its goal by ensuring early access to prenatal care, HIV and syphilis testing for pregnant women and their partners, treatment for those who test positive and their babies, substitution of breastfeeding among those affected, and prevention of HIV and syphilis before and during pregnancy through promotion of condoms use and other measures. 4- Franzen, C (December 2008). "Syphilis in composers and musicians--Mozart, Beethoven, Paganini, Schubert, Schumann, Smetana". European Journal of Clinical Microbiology & Infectious Diseases. 5- Catharine Arnold, The Sexual History of London. 6- Syphilis in art: an entertainment in four parts. Part 1. Morton RS Genitourin Med. 1990 Feb; 66(1):33-40. 7- Who is Dürer's "Syphilitic Man"? Eisler CT Perspect Biol Med. 2009 Winter; 52(1):48-60. 8- Foa A, compiler. In: The new and the old: the spread of syphilis (1494–1530) Baltimore: Johns Hopkins University Press; 1990. pp. 26–45. 9- Forrai J, compiler. In: History of Different Therapeutics of Venereal Disease Before the Discovery of Penicillin,Syphilis - Recognition, Description and Diagnosis. Dr. Neuza Satomi Sato; 2011. 10- ohn Hunter's alleged syphilis. Qvist G Ann R Coll Surg Engl. 1977 May; 59(3):206-9. 11- The Great Pox that was...syphilis. Sefton AM J Appl Microbiol. 2001 Oct; 91(4):592-6. 12- De Souza EM. A hundred years ago, the discovery of Treponema pallidum. An Bras Dermatol. 2005;80:547–548. 13- [The significance of Karl Landsteiner's works for syphilis research]. Luger A Wien Klin Wochenschr. 1991; 103(5):146-51. 14- Quétel C, compiler. In: History of Syphilis. Polity; 1992. 15- 'Two minutes with venus, two years with mercury'--mercury as an antisyphilitic chemotherapeutic agent. O'Shea JG J R Soc Med. 1990 Jun; 83(6):392-5. 16- Patton ME, Su JR, Nelson R, Weinstock H, Centers for Disease Control and Prevention (CDC). Primary and secondary syphilis--United States, 2005-2013. MMWR Morb Mortal Wkly Rep. 2014 May 9. 63 (18):402-6. 17- Eccleston, K; Collins, L; Higgins, SP (March 2008). "Primary syphilis". International journal of STD & AIDS. 18- Mullooly, C; Higgins, SP (August 2010). "Secondary syphilis: the classical triad of skin rash, mucosal ulceration and lymphadenopathy". International journal of STD & AIDS. 19- G. W. Csonka (1990). Sexually transmitted diseases: a textbook of genitourinary medicine. Baillière Tindall. p. 232. ISBN 978-0-7020-1258-7. Archived from the original on 3 May 2016. 20- NHS Choices 'Syphilis - Symptoms' [accessed 27 October 2015] 21- WebMD 'Understanding Syphilis - Diagnosis and Treatment' [accessed 27 October 2015] 22- Foa A, compiler. In: The new and the old: the spread of syphilis (1494–1530) Baltimore: Johns Hopkins University Press; 1990. pp. 26–45. 23- Weissfeld AS. Infectious Diseases and Famous People Who Succumbed to Them Clinical Microbiology Newsletter. Clinical Microbiology Newsletter. 2009;31:169–172.
- 20. 20 24- De Souza EM. A hundred years ago, the discovery of Treponema pallidum. An Bras Dermatol. 2005;80:547–548. 25- Illustrated Dictionary of Podiatry and Foot Science by Jean Mooney © 2009 Elsevier Limited. All rights reserved. 26- Ghanem KG. Management of Adult Syphilis: Key Questions to Inform the 2015 Centers for Disease Control and Prevention Sexually Transmitted Diseases Treatment Guidelines. Clin Infect Dis. 2015 Dec 15. 61 Suppl 8:S818-36. 27- Ghanem KG, Workowski KA. Management of adult syphilis. Clin Infect Dis. 2011 Dec. 53 Suppl 3:S110-28. 28- Nathan L, Bawdon RE, Sidawi JE, Stettler RW, McIntire DM, Wendel GD Jr. Penicillin levels following the administration of benzathine penicillin G in pregnancy. Obstet Gynecol. 1993 Sep. 82 (3):338-42. 29- Collart P, Poitevin M, Milovanovic A, Herlin A, Durel J. Kinetic study of serum penicillin concentrations after single doses of benzathine and benethamine penicillins in young and old people. Br J Vener Dis. 1980 Dec. 56 (6):355-62. 30- Hagdrup HK, Lange Wantzin G, Secher L, Rosdahl VT. Penicillin concentrations in serum following weekly injections of benzathine penicillin G. Chemotherapy. 1986. 32 (2):99-101. 31- Frentz G, Nielsen PB, Espersen F, Czartoryski A, Aastrup H. Penicillin concentrations in blood and spinal fluid after a single intramuscular injection of penicillin G benzathine. Eur J Clin Microbiol. 1984 Apr. 3 (2):147-9. 32- Workowski KA, Bolan GA. Centers for Disease Control and Prevention Sexually Transmitted Diseases Treatment Guidelines. MMWR. June 5, 2015. 64(RR3):1-137. 33- lement, Meredith E.; Okeke, N. Lance; Hicks, Charles B. (2014). "Treatment of Syphilis". JAMA. 312 (18): 1905. doi:10.1001/jama.2014. 34- Ananya Mandal, MD,Syphilis Treatment,https://www.news medical.net/health/Syphilis- Treatment.aspx,Nov 28, 2012 35- Koss CA, Dunne EF, Warner L (July 2009). "A systematic review of epidemiologic studies assessing condom use and risk of syphilis". Sex Transm Dis. 36- Shahrook, S; Mori, R; Ochirbat, T; Gomi, H (29 October 2014). "Strategies of testing for syphilis during pregnancy". The Cochrane Database of Systematic Reviews. 37- Harper KN, Zuckerman MK, Harper ML. The origin and antiquity of syphilis revisited: an appraisal of Old World pre-Columbian evidence for treponemal infection. Am J Phys Anthropol. 2011;146:99–133. 38- Rubin R., Strayer D. (2012). Rubin’s pathology: Clinicopathologic foun- dations of medicine (6th ed.). Philadelphia, PA: Lippincott Williams & Wilkins. 39- Centers for Disease Control and Prevention. (2010). Syphilis statis- tics. http://www.cdc.gov/std/stats10/syphilis.htm. Accessed November 25, 2011. Figures' References 1- http://www.homeoresearch.com/differences-of-chancres-with-reference/ 2- https://medical-dictionary.thefreedictionary.com/syphilis 3- Venzmer G. O boala care dispare, Sifilisul. Atelierele Adevarul. 1933 4- http://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1001396 5- Rubin E., Gorstein F., Rubin R., et al. (Eds.) (2012). Rubin’s pathology: Clinicopathologic foundations of medicine (6th ed., p. 376). Philadelphia, PA: Lippincott Williams & Wilkins.)