Bilharziasis and Associated Malignancies
•Download as PPTX, PDF•
7 likes•418 views

The document discusses various parasitic diseases including schistosomiasis and echinococcosis. It describes the causative agents, transmission, pathogenesis and complications of schistosomiasis including urinary schistosomiasis and intestinal schistosomiasis. Long-term infection with urinary schistosomiasis can lead to squamous cell carcinoma of the bladder due to chronic irritation and squamous metaplasia. Hydatid cysts caused by echinococcus granulosus are also discussed, including their gross and microscopic appearance. Images show examples of lesions caused by these parasitic infections.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Bilharziasis and Associated Malignancies
Similar to Bilharziasis and Associated Malignancies (20)
More from DOCTOR WHO
More from DOCTOR WHO (20)
Recently uploaded
Recently uploaded (20)
Bilharziasis and Associated Malignancies
- 1. Bilharziasis
- 2. Learning Objectives 1. Aetiology , mode of transmission and pathogenesis of urinary and intestinal Schistosomiasis 2. Description of the morphology of colonic and urinary Schistosomiasis (sandy patches, polyps, ulcer, cystitis, cystic cystitis, glandularis, Brunn’s nests) 3. The relationship of squamous metaplasia in urinary Schistosomiasis to development of carcinoma. 4. Complications of Schistosomiasis like hepatic fibrosis and others 5. The gross and histological appearance of the hydatid disease and the hydatid cyst.
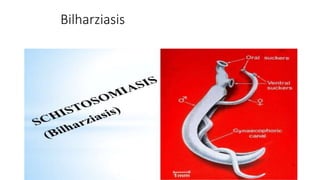
- 3. Schistosomiasis • Also known as bilharzia or bilharziosis • Parasitic disease caused by several species of trematodes • This disease is most commonly found in Asia, Africa and South America, especially in areas where the water contains numerous freshwater snails, which may carry the parasite
- 4. Schistosoma Species of Schistosoma that can infect humans: • Schistosoma mansoni cause intestinal schistosomiasis • Schistosoma haematobium causes urinary schistosomiasis • Schistosoma japonicum causes Asian intestinal schistosomiasis
- 5. Schistosoma Route of Entry • Human can acquire the disease by swimming or playing in infected water • Parasitic larvae easily enter through skin and further mature within organ tissues life cycle
- 6. Pathological Lesions Continuing infection and irritation may cause granulomatous reactions and fibrosis in the affected organs, which may result in manifestations that include: • Colonic polyposis with bloody diarrhea (Schistosoma mansoni ) • Portal hypertension with hematemesis and splenomegaly (S. mansoni, S. japonicum) • Cystitis, ureteritis and hematuria (S. haematobium) continuous irritation causes squamous metaplasia, dysplasia and squamous cell carcinoma of the bladder • Glomerulonephritis • Central nervous system granulomatous lesions
- 8. Schistosoma haematobium Infection of the bladder with numerous calcified eggs and extensive scarring
- 9. Schistosoma mansoni Granuloma with a miracidium-containing egg (center) and numerous, adjacent, scattered eosinophils.
- 10. Schistosoma mansoni Pipe stem Fibrosis; Pipe-shaped fibrosis formed around hepatic portal veins in some cases of long-continued heavy infection with Schistosoma mansoni
- 11. Clinical Manifestations Acute schistosomiasis: may occur weeks after the initial infection with following clinical manifestations : • Mild itching and a papular dermatitis of the feet after swimming in polluted streams containing cercariae • Abdominal pain and diarrhea • Fever, cough and fatigue • Hepatosplenomagly and esophageal varices Chronic Schistosomiasis: clinical features includes: • Hematuria and mild anemia • Malnutrition
- 12. Diagnosis • Detection of parasitic antigens by ELISA in a patient blood sample. This screening method is highly effective • Microscopic identification of eggs in stool or, less commonly in the urine is another way of arriving at a positive diagnosis
- 14. Echinococcosis Causative agent: A parasitic disease caused by Echinococcus granulosis Transmission: Fecal-oral contamination Distribution: Worldwide where sheep are common Life cycle: The ingestion of infective eggs by man is followed by hatching of oncospheres in the intestine which penetrate the intestinal wall and migrate to various tissues , often liver or lungs, where hydatid cyst development occurs over many years
- 15. Life Cycle of Echinoccocus
- 16. Pathological Lesion Grossly: • Intact cyst from an infected viscera shows gray-white to off-white membranous unilocular cyst filled with clear fluid which is separated from the visceral tissue by fibrous tissue • Cutting open cyst shows large number of daughter larvae with characteristic hooklets of the scolex which settle out and form the so-called hydatid sand Microscopically: • Basophilic laminated cyst wall lined by a germinal epithelium and scattered hooklets and multiple scolex • Surrounding visceral tissue shows chronic inflammation and fibrosis
- 17. Gross Morphology Hydatid Cyst
- 18. Microscopy: Hydatid Cyst wall and Scolices Laminated cyst wall with hydatid sand Scattered hooklets and multiple scolex
- 19. Echinococcosis Clinical manifestations • The hydatids produce cystic mass lesions • Rupture of hydatid cysts may produce anaphylaxis • Scolices released from ruptured cyst can produce additional cysts Diagnosis: • Ultrasound or CT scan to locate hydatid cysts • Serologic methods by ELISA may aid in diagnosis • Microscopic examination of hydatid sand, hook lets and scloex
- 20. Protozoal Infections Name of protozoa Disease Entameba histolytica: Dysentery, Amebic live abscess Giardia lamblia: Noisy watery diarrhea with abdominal cramps Leishmania donovani: Non healing cutaneous ulcer and bone marrow involvement Plasmodium; vivax, falciparum: Malaria fever with chills Trichomonas vaginalis: Foul smelling vaginal discharge
- 22. Amebic Typhilitis • Flask shaped ulcer in cecum due to Entameba histolytica • Under high power, some of the organisms Trophozoite form shows ingested red blood cells
- 24. Home Assignment Q. Which type of malignancy is associated with schistosomiasis? 2/19/2018
- 25. Learning Outcomes 1. Know the different types of causative agents and mode of transmission of Schistosomiasis 2. Understand the pathogenesis of both urinary and intestinal Schistosomiasis. 3. List the complications of both urinary and intestinal Schistosomiasis. 4. Know the relation between malignancy and urinary Schistosomiasis 5. Diagnosis of Schistosomiasis 6. Identify gross and histological appearance of the hydatid cyst. 7. Identify trophozoites of ameba in amebic ulcer
- 26. References • Robbins Basic Pathology, 9th Edition (2013) By: Kumar, Abbas, Aster Web Path • www.fleshandbone.com • www.studentconsult.com