LUMBER PUNCTURE By Dr Bashir Ahmed Dar Associate Professor Medicine Chinkipor...
meningococcus PPT
1. NEISSERIA MENINGITIS
IntroductionIntroduction
N. Meningitis is an aerobic,
gram negative diplococci which causes
septicaemia and meningitis
There are 13 capsulated serogroups
causing invasive meningococcal
diseases, of these the majority are
serogroup A, B, C, W-135, X and Y.
N. Meningitis is an aerobic,
gram negative diplococci which causes
septicaemia and meningitis
There are 13 capsulated serogroups
causing invasive meningococcal
diseases, of these the majority are
serogroup A, B, C, W-135, X and Y.
Source and TransmissionSource and Transmission
Source: They are normal flora found at the
back of the nose and throat of humans.
Human beings are the definitive host for
meningococcal bacteria
Transmission: Person to person prolonged
close contact: coughing, sneezing, kissing
and breathing each others breath with
infected individual
Source: They are normal flora found at the
back of the nose and throat of humans.
Human beings are the definitive host for
meningococcal bacteria
Transmission: Person to person prolonged
close contact: coughing, sneezing, kissing
and breathing each others breath with
infected individual
EpidemiologyEpidemiology
Meningococcal serogroups A, B, C, W-135, X and
Y are globally distributed in different regions.
The highest prevalence globally is in Africa around
the Meningitis belt in the Sub-Saharan Africa where
by serogroup A is most common followed by other
serogroups. Asia is second where by serogroup A
and C are most common. In UK there are around
1500 cases per year, majority of cases are Serogroup
B followed by serogroup C and W. In America:
serogroup B and C are common followed by Y and
W-135.
Meningococcal serogroups A, B, C, W-135, X and
Y are globally distributed in different regions.
The highest prevalence globally is in Africa around
the Meningitis belt in the Sub-Saharan Africa where
by serogroup A is most common followed by other
serogroups. Asia is second where by serogroup A
and C are most common. In UK there are around
1500 cases per year, majority of cases are Serogroup
B followed by serogroup C and W. In America:
serogroup B and C are common followed by Y and
W-135.
Virulence factors and pathogenesisVirulence factors and pathogenesis
N. Meningitis enters the blood stream as a result of
damaged nasopharyngeal mucosa. Pili, Opa and
Opc facilitate attachment and binding to the host
cells. In the bloodstream, polysaccharide capsule
protect N. meningitis against complement-mediated
lysis and phagocytosis as a result the bacteria
replicate rapidly and cause septicaemia. The
bacteria also produce enterotoxin (LOS) Increased
bacteria in the blood facilitate the bypassing of
Blood Brain barrier and cause meningitis. Antigenic
variability and capsular switching are major cause
of virulence to N. Meningitis
N. Meningitis enters the blood stream as a result of
damaged nasopharyngeal mucosa. Pili, Opa and
Opc facilitate attachment and binding to the host
cells. In the bloodstream, polysaccharide capsule
protect N. meningitis against complement-mediated
lysis and phagocytosis as a result the bacteria
replicate rapidly and cause septicaemia. The
bacteria also produce enterotoxin (LOS) Increased
bacteria in the blood facilitate the bypassing of
Blood Brain barrier and cause meningitis. Antigenic
variability and capsular switching are major cause
of virulence to N. Meningitis
Risk factorsRisk factors
Under five children, aged 11 to 17 and
younger adults
Upper Respiratory infection
Immunocompromised individuals
Crowding
Dry season and template climate
Others like smoking, pub and low social
economic status
Under five children, aged 11 to 17 and
younger adults
Upper Respiratory infection
Immunocompromised individuals
Crowding
Dry season and template climate
Others like smoking, pub and low social
economic status
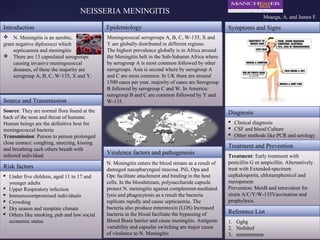
Symptoms and SignsSymptoms and Signs
DiagnosisDiagnosis
Clinical diagnosis
CSF and blood Culture
Other methods like PCR and serology
Clinical diagnosis
CSF and blood Culture
Other methods like PCR and serology
Treatment and PreventionTreatment and Prevention
Treatment: Early treatment with
penicillin G or ampicillin. Alternatively
treat with Extended-spectrum
cephalosporin, chloramphenicol and
meropenem
Prevention: MenB and tetravalent for
strain A/C/Y/W-135Vaccination and
prophylaxis.
Treatment: Early treatment with
penicillin G or ampicillin. Alternatively
treat with Extended-spectrum
cephalosporin, chloramphenicol and
meropenem
Prevention: MenB and tetravalent for
strain A/C/Y/W-135Vaccination and
prophylaxis.
Reference ListReference List
1. Gghg
2. Nnfnhnf
3. mnmnmnmn
1. Gghg
2. Nnfnhnf
3. mnmnmnmn
Msanga, A. and James F.