
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Manualmusletesting 211 240
Similar to Manualmusletesting 211 240 (20)
Recently uploaded
Recently uploaded (20)
Manualmusletesting 211 240
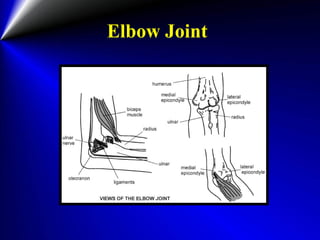
- 1. Elbow Joint
- 3. Muscles contribute to Elbow Flexion Brachioradialis • Origin: • Upper 2/3 of lateral supracondylar ridge of humerus • Insertion: • Styloid process of radius • Action: • Elbow Flexion • Nerve supply:
- 4. Muscles contribute to Elbow Flexion Biceps Brachii • Origin: • Long head: supraglenoid tubercle • Short head: coracoid process • Insertion: • Radial tuberosity • Action: • Elbow Flexion • Nerve supply
- 5. Muscles contribute to Elbow Flexion Brachialis • Origin: • Lower portion of anterior surface of humerus • Insertion: • Coronoid process of ulna • Action: • Elbow Flexion • Nerve supply
- 6. Normal & Good • Position: • Sitting with slight shoulder flexion and the elbow flexed past 90°, forearm is supinated. • Ask the patient to, “hold your elbow bent, and don’t let me straighten it out.” • Palpation: • Muscle belly or just medial on crease of elbow tendon. • Stabilization: • Stabilizing hand is placed on the shoulder. • Desired Motion: • Patient flexes elbow through range of motion. • Resistance • Is given at the wrist in a downward direction.
- 7. Normal & Good Brachioradialis: forearm in midposition between pronation and supination Biceps brctchii : forearm in supination Brachialis : forearm in pronation
- 8. Fair • Position: • Sitting with arm at side and forearm supinated • Stabilization: • Stabilize upper arm. • Desired Motion: • Patient flexes elbow through range of motion.
- 9. Poor • Position: • Supine with shoulder abducted to 90 and laterally rotated ْ. • Stabilization: • stabilizing hand is placed on the shoulder. • Desired Motion: • Patient slides forearm along table through complete range of elbow flexion. • (If range of motion is limited in lateral rotation at shoulder joint, test may be given with arm medially rotated.)
- 10. Trace & Zero • Examiners palpate the flexors on the forearm; muscle fibers may be found on anterior surface of arm.
- 11. Alternate Test for Elbow Flexion • This alternate test is performed if the biceps and brachialis are weak. • Pronating the hand will instead use the brachioradialis, extensor carpi radialis longus, pronator teres, and other wrist flexors. • Patients positioning is the same, except the forearm is now pronated and the stabilizing hand is under the elbow joint. • Testing procedure is the same as before.
- 12. Note • Note: • The wrist flexors may be contracted for assistance in elbow flexion. • Wrist will be strongly flexed as a result. Wrist should be relaxed.
- 13. Note • Range of motion: 0º to 145º - 160º • Factors Limiting Motion: 1-Contact of muscle masses volar aspect of arm and forearm. 2-Contact of coronoid process with coronoid fossa of humerus • Fixation: 1-Weight of arm 2-Fixator muscles of scapula • Substitutions: 1. Brachioradialis 2. Flexors group of the wrist and fingers:FCR, FCU, palmaris longus, FDS, FPL and pronator teres.
- 15. Muscles contribute to Elbow Extension Triceps Brachii • Origin: • Long head: Scapula, infraglenoid tubercleScapula, infraglenoid tubercle • Lateral head: Humerus, 1/3 lateral-posterior surface • Medial head: Humerus, lower 3/4 of posterior surface • Insertion: Olecranon process of ulna • Nerve supply
- 16. Note • Range of Motion: 145º – 160º to 0º • Factors Limiting Motion: 1-Tension of anterior, radial and ulnar collateral ligaments of elbow joint. 2-Tension of flexor muscles of forearm. 3-Contact of olecranon process with olecranon fossa on posterior aspect of humerus. • Fixation: 1-Weight of arm 2-Contraction of Fixator muscles of scapula. • Substitutions Muscles: 1-Rotators 2-Wrist extensors 3-Anconeous
- 17. Normal & Good • Position: • Patient is prone on the table with the shoulder abducted to 90°, the entire arm should be off the table and the therapist can stabilize the arm at the humerus just above the elbow. The elbow should be in full extension. • Palpation: Proximal to olecranon process. • Stabilization: Stabilize arm. • Desired Motion: Patient extends elbow through ROM. • Resistance: Is applied at wrist in a downward direction.
- 18. Fair • Position: Supine with shoulder flexed to 90ْand elbow flexed. • Palpation: The same as before • Stabilization: Stabilize arm. • Desired Motion: Patient extends elbow through range of motion Alternate
- 19. Poor • Position: Supine with arm abducted to 90 degrees and laterally rotated. Elbow is flexed. • Stabilization: Stabilize arm. • Desired Motion: Ask the patient to, “straighten your elbow, don’t let him bend it down. (if range of motion is limited in lateral rotation at shoulder joint, test may be given with arm medially rotated)
- 20. Trace & Zero • Examiner may palpate tendon of Triceps brachii at the elbow joint and muscle fibers on posterior surface of arm.
- 21. Muscles contribute to Forearm Supination Biceps Brachii Supinator Teres
- 22. Biceps Brachii • Origin: • Long head: supraglenoid tubercle • Short head: coracoid process • Insertion: Radial tuberosity • Nerve supply
- 23. Muscles contribute to Forearm Supination Supinator Teres • Origin: • lateral epicondylelateral epicondyle of Humerusof Humerus • posterior part of ulnaposterior part of ulna • Insertion: upper 1/3 lateral surface of Radius. • Nerve supply
- 24. Note • Range of motion: 0ºTO 90º Supination from midposition • Factors Limiting Motion: 1-Tension of Volar radioulnar ligament and ulnar collateral ligament of wrist joint. 2-Tension of oblique cord and lowest fibers of interosseous muscles of forearm. • Fixation: • Weight of arm
- 25. Normal & Good • Position: Sitting with arm at side, elbow flexed to 90 degrees and forearm pronated to prevent rotation at the shoulder. Muscles of wrist and fingers are; relaxed. • Stabilization: Stabilize arm. • Desired Motion: Patient supinates forearm. • Resistance: Is given on dorsal surface of distal end of radius. (Resistance may be given by grasping around the dorsal surface of the hand instead of the position illustrated.)
- 26. Fair & Poor • Position: • Silting with arm at side, elbow flexed to 90º, forearm pronated and supported by examiner. • Muscles of wrist and fingers are relaxed. • Desired Motion: • Patient supinates forearm through full range of motion for fair grade and through partial for poor grade. Fair Poor
- 27. Trace & Zero • Supinator muscle is palpable on radial side of forearm if overlying extensor muscles are not functioning. Tendon of Biceps brachii is found in antecubital space
- 28. Note • Patient should not be allowed to laterally rotate arm and move elbow across thorax as forearm is supinated. • As a result of this movement the forearm may appear to be supinated, but range of motion is incomplete. • This motion may "roll" the forearm into supination without a muscular contraction taking place.
- 30. Muscles contribute to Forearm Pronation Pronator Teres • Origin: • Humerus, medial epicondyleHumerus, medial epicondyle • Insertion: • Radius, middle 3rd of lateral surface • Action: • Forearm Pronation • Nerve supply