
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Manualmusletesting 391 420
Similar to Manualmusletesting 391 420 (20)
More from Anaum1990
Recently uploaded
Recently uploaded (20)
Manualmusletesting 391 420
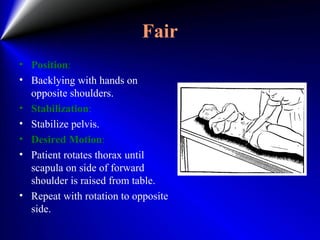
- 1. Fair • Position: • Backlying with hands on opposite shoulders. • Stabilization: • Stabilize pelvis. • Desired Motion: • Patient rotates thorax until scapula on side of forward shoulder is raised from table. • Repeat with rotation to opposite side.
- 2. Poor • Position: • Sitting with arms relaxed at sides. • Stabilization: • Pelvis stabilized. • Desired Motion: • Patient rotates thorax. • Repeat with rotation to opposite side.
- 3. Trace & Zero • Examiner palpates muscles as patient attempts to approximate thorax on left and pelvis on right. Repeat on opposite side. • Note: Observe deviation of umbilicus, which will move toward strongest quadrant if there is a difference in strength of opposing oblique muscles.
- 5. MUSCLE THAT ACT ON THE ANTERIOR THIGH (FEMUR)
- 6. MUSCLE THAT ACT ON THE POSTERIOR THIGH (FEMUR)
- 7. Elevation of pelvis • QUADRATUS LUMBORUM
- 8. QUADRATUS LUMBORUM • ORIGIN: Inferior border of 12th rib • INSERTION Apices of transverse processes of L1-4, iliolumber ligament and posterior third of iliac crest • ACTION Fixes 12th rib during respiration and lateral flexes trunk • NERVE Anterior primary rami (T12-L3)
- 9. QUADRATUS LUMBORUM • Range of Motion: • In standing position pelvis may he raised on one side until foot is well clear of floor. (Reverse action of Quadratus lumborum.) • Factors Limiting Motion: • Tension of spinal ligaments on opposite side • Contact of iliac crest with thorax • Fixation: • Contraction of spinal extensor muscles (o fix thorax
- 10. NORMAL AND GOOD • Position: Backlying (or Facelying) with lumbar area of spine in moderate extension. Patient grasps edge of table to stabilize thorax. (If-arm and shoulder muscles are weak, an assistant should stabilize thorax.) • Desired Motion: Patient draws pelvis toward thorax on one side. • Resistance is given above ankle joint.
- 11. FAIR AND POOR • Position: Backlying with legs straight and with lumbar area of spine in moderate extension. • Patient may grasp side of table to stabilize thorax (not shown in picture). • Desired Motion: Patient draws pelvis upward toward thorax. • Slight resistance is given for a fair grade. Completion of range is graded poor.
- 12. FAIR (Alternate) • Standing position. • Stabilize thorax. • Desired motion: Patient lifts pelvis toward thorax through ROM
- 13. TRACE AND ZERO • As patient attempts to draw pelvis cranial ward, a contraction of Quadratus lumborum may be determined by deep palpation in lumbar area under lateral edge of Erector spinae.
- 14. Sartorius Origin: Anterior superior iliac spine Insertion: medial surface of the tibia Function: Hip flexion, Abduction, and External Rotation with Knee Position Nerve supply: • Psoas major: lumbar plexus • Iliacus: lumbar plexus
- 15. Normal and Good Position: Sitting with thighs supported on the table and legs dangling off, the patient can place their hands down for support. Desired Motion: The patient flex, abduct, and externally rotate at the hip, and flex at the knee. Resistance. • One hand will be placed on the lateral surface of the knee, and the other will be placed on the medial aspect of the ankle. • The hand at the knee will resist hip flexion and abduction and the resistance will be given in a down and inward direction. • The hand at the ankle will be resisting external rotation and knee flexion and the resistance is in an up and outward direction. • Ask the patient to, “slide your heel up the shin of your other leg, don’t let me move your leg or straighten your knee.”
- 16. FAIR AND POOR Position: Sitting with thighs supported on the table and legs dangling off, the patient can place their hands down for support. Desired Motion: The patient flex, abduct, and externally rotate at the hip, and flex at the knee.
- 17. TRACE AND ZERO • Patient Position: • Supine, with the therapist supporting the limb. • The heel should be on the shin of the opposite leg. • While palpating the sartorius ask the patient to slide their heel up to their knee.
- 18. Hip Flexion • Sartorius • PSOAS MAJOR • ILIACUS
- 19. PSOAS MAJOR • ORIGIN: Transverse processes of L1-5, bodies of T12- L5 and intervertebral discs below bodies of T12-L4 • INSERTION: Middle surface of lesser trochanter of femur • ACTION: • Flexes and medially rotates hip • NERVE: • Anterior primary rami of L1,2
- 20. ILIACUS • ORIGIN: Iliac fossa within abdomen • INSERTION: Lowermost surface of lesser trochanter of femur • ACTION: Flexes medially rotates hip • NERVE: Femoral nerve in abdomen (L2,3)
- 21. Hip Flexion • Range of Motion: Factors Limiting Motion: • With knee Hexed, contact of thigh on abdomen • With knee extended, tension of hamstring muscles Fixation: 1.Contraction of anterior abdominal muscle to fix lumber spine and pelvis. 1.Weight at trunk
- 22. Normal and Good • Position: Sitting with legs over edge of table. • Stabilization: Stabilize pelvis. • Desired Motion: Patient flexes hip through last part of range of motion. Resistance is given proximal to knee joint.
- 23. Fair • Sitting with legs over edge of table. • Stabilize pelvis. • Patient flexes hip through last part of ROM.
- 24. Poor • Position: Sidelying with upper leg supported. Trunk pelvis and legs straight. • Stabilize pelvis. • Patient flexes hip through range of motion Knee is allowed to flex to prevent hamstring tension.
- 25. TRACE AND ZERO • Supine with leg supported. It may be possible to detect contraction in Psoas major just distal to inguinal ligament on medial side of Sartorius.
- 26. Note • Substitution by Sartorius in hip flexion will cause lateral rotation and abduction of thigh. Muscle may be seen and palpated near its origin during the motion. • Substitution by Tensor Fasciae Latae in hip flexion causes medial rotation and abduction of the thigh. Muscle may be seen and palpated at its origin.
- 27. Hip Extension • GLUTEUS MAXIMUS • BICEPS FEMORIS • SEMIMEMBRANOSUS • SEMITENDINOSUS
- 28. GLUTEUS MAXIMUS • ORIGIN Outer surface of ilium behind posterior gluteal line and posterior third of iliac crest lumbar fascia, lateral mass of sacrum, sacrotuberous ligament and coccyx • INSERTION Deepest quarter into gluteal tuberosity of femur, remaining three quarters into iliotibial tract (anterior surface of lateral condyle of tibia) • ACTION Extends and laterally rotates hip. Maintains knee extended via iliotibial tract • NERVE: Inferior gluteal nerve (L5, S1,2)
- 29. BICEPS FEMORIS ORIGIN Long head: upper inner quadrant of posterior surface of ischial tuberosity. • Short head: middle third of linea aspera, lateral supracondylar ridge of femur INSERTION Styloid process of head of fibula. lateral collateral ligament and lateral tibial condyle ACTION Flexes and laterally rotates knee. Long head extends hip NERVE Long head: tibial portion of sciatic nerve. Short head: common peroneal portion of sciatic nerve (both L5, S1)
- 30. SEMIMEMBRANOSUS • ORIGIN Upper outer quadrant of posterior surface of ischial tuberosity • INSERTION Medial condyle of tibia below articular margin, fascia over popliteus and oblique popliteal ligament • ACTION Flexes and medially rotates knee. Extends hip • NERVE Tibial portion of sciatic nerve (L5, S1)