1. Participants
• Participants were males and females
drawn from the metropolitan Boston Area.
• There were 45 prodromal subjects and 39
healthy controls, who were matched
based on sex, age, education, race, and
ethnic group, as shown on the table
below.
Methodology
• Secondary analysis of a longitudinal
study in which the same group of subjects
were assessed twice.
• All participants provided informed
consent.
• Clinical high-risk approaches from various
clinical assessments and diagnostic
interviews were used.
• Assessments used included the following:
Structured Clinical Interview for DSM-IV,
Structured Interview for Prodromal
Symptoms, Beck Anxiety Inventory,
Social Phobia & Anxiety Inventory,
Anxiety Sensitivity Index.
I would like to express my gratitude to Jennifer
McKelvey, PhD of the Commonwealth Research
Center of Beth Israel Deaconess Medical Center
and the Massachusetts Mental Health Center, as
well as the study participants, for without them this
research would not be possible.
• Few existing studies have focused on the
presence of anxiety disorders in individuals
who are at clinical high risk (CHR) for
psychosis.
• Increasing interest in intervention for
psychosis during the clinical high-risk
phase has led to research on anxiety
sensitivity and prodromal symptoms.
• In this study, factors associated with co-
morbidity of anxiety disorders in the
clinical high-risk (prodromal) phase of
psychosis were investigated, as well as
the anxiety disorders that were most
prevalent in this population.
² 1. Higher scores on ratings of prodromal
symptoms will be correlated with higher
scores on measures of anxiety and
anxiety sensitivity.
² 2. Certain anxiety disorders will have a
higher prevalence with prodromal
symptoms, while others will have a lower
prevalence. In accordance with
research that has identified anxiety
disorders comorbid with psychosis, it is
hypothesized that social anxiety,
generalized anxiety disorder, and
possibly obsessive-compulsive disorder
will have a higher correlation with
prodromal psychosis, whereas
posttraumatic stress disorder and
specific phobia will have a lower
correlation.
² 3. Higher scores on a measure of
sensitivity to anxiety will be found for
participants identified as at clinical high
risk as compared to healthy controls.
• Also as predicted, clinical high risk
subjects had statistically higher levels of
anxiety sensitivity when compared to the
controls. The graphs labeled Figure 2 and
Figure 3 illustrate the results.
0
2
4
6
8
10
12
14
16
18
20
Clinical High Risk Healthy Controls
MeanBeckAnxietyScore
Group
Figure 2: Beck Anxiety
Scores by Group
0
50
100
150
200
250
300
350
Clinical High Risk Healthy Controls
MeanSocialPhobia&AnxietyInventoryTotal
Group
Figure 3: SPAI Scores by
Group
• Anxiety was found to be a prominent
concern in this sample, in which 26 of the
clinical high-risk subjects (58%) had at
least one diagnosis of anxiety, as well as
had significantly more anxiety than in the
general population.
• Results from this study indicate that
anxiety is a significant issue affecting those
who are identified as at clinical high-risk for
psychosis.
• These findings suggest that social anxiety,
general anxiety disorder, obsessive
compulsive disorder, and anxiety sensitivity
may have a significant impact both on the
functioning of clinical high-risk individuals
and on the development of psychosis.
Limitations
• Missing data on assessments & low
sample size reduced statistical power.
• Self report assessments may have resulted
in ambiguity.
• As expected, anxiety is a significant issue
affecting prodromal psychosis patients.
• There was not, however, a significant
correlation between anxiety sensitivity
and prodromal symptoms.
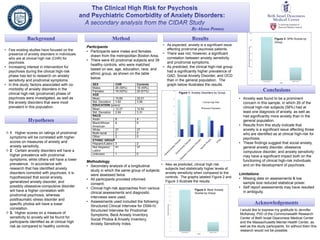
• As predicted, the clinical high-risk group
had a significantly higher prevalence of
GAD, Social Anxiety Disorder, and OCD
than in the general population. The
graph below illustrates the results.
0
5
10
15
20
25
30
Clinical High Risk
General Population
Figure 1: Anxiety Disorders by Group