
Recommended
More Related Content
Similar to Screening of covid 19 patient
Similar to Screening of covid 19 patient (20)
More from Abhishek Srivastava
More from Abhishek Srivastava (11)
Recently uploaded
Recently uploaded (20)
Screening of covid 19 patient
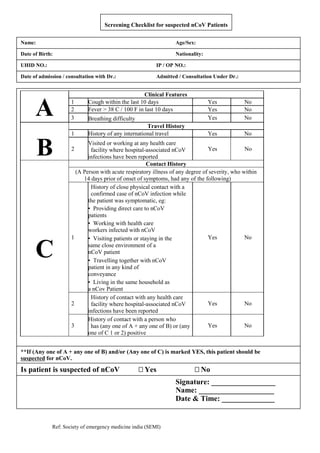
- 1. Ref: Society of emergency medicine india (SEMI) Screening Checklist for suspected nCoV Patients Patient Information: Name: Age/Sex: UHID NO.: IP / OP NO.: Date of admission / consultation with Dr.: Admitted / Consultation Under Dr.: Date of Birth: Nationality: A Clinical Features 1 Cough within the last 10 days Yes No 2 Fever > 38 C / 100 F in last 10 days Yes No 3 Breathing difficulty Yes No B Travel History 1 History of any international travel Yes No 2 Visited or working at any health care facility where hospital-associated nCoV infections have been reported Yes No C Contact History (A Person with acute respiratory illness of any degree of severity, who within 14 days prior of onset of symptoms, had any of the following) 1 History of close physical contact with a confirmed case of nCoV infection while the patient was symptomatic, eg: Yes No • Providing direct care to nCoV patients • Working with health care workers infected with nCoV • Visiting patients or staying in the same close environment of a nCoV patient • Travelling together with nCoV patient in any kind of conveyance • Living in the same household as a nCov Patient 2 History of contact with any health care facility where hospital-associated nCoV infections have been reported Yes No 3 History of contact with a person who has (any one of A + any one of B) or (any one of C 1 or 2) positive Yes No **If (Any one of A + any one of B) and/or (Any one of C) is marked YES, this patient should be suspected for nCoV. Is patient is suspected of nCoV Yes No Signature: _________________ Name: ____________________ Date & Time: ______________
- 2. Ref: Society of emergency medicine india (SEMI)