Deceleration form related to travel history & health condition in view of outbreak of COVID - 19
•
0 likes•68 views
Deceleration form related to the travel history of patient
Report
Share
Report
Share
Download to read offline
Recommended
Recommended
east zone medico legal services pvt.ltdForm consent for_release_of_medical_records_use_disclosure_of_phi
Form consent for_release_of_medical_records_use_disclosure_of_phieast zone medico legal services pvt.ltd
More Related Content
What's hot
What's hot (8)
KZN Health MEC refutes false and irresponsible reporting on coronavirus
KZN Health MEC refutes false and irresponsible reporting on coronavirus
Similar to Deceleration form related to travel history & health condition in view of outbreak of COVID - 19
east zone medico legal services pvt.ltdForm consent for_release_of_medical_records_use_disclosure_of_phi
Form consent for_release_of_medical_records_use_disclosure_of_phieast zone medico legal services pvt.ltd
Similar to Deceleration form related to travel history & health condition in view of outbreak of COVID - 19 (20)
Form consent for_release_of_medical_records_use_disclosure_of_phi
Form consent for_release_of_medical_records_use_disclosure_of_phi
Apollo Munich Easy Health Insurance Pre Authorization Form
Apollo Munich Easy Health Insurance Pre Authorization Form
Patients NameBirth Date AgeStreet AddressPhone Nu.docx
Patients NameBirth Date AgeStreet AddressPhone Nu.docx
this is a discussion not a paper I need a paragraph under each quest.docx
this is a discussion not a paper I need a paragraph under each quest.docx
Health Suraksha Health Insurance Claim Form - HDFC ERGO
Health Suraksha Health Insurance Claim Form - HDFC ERGO
More from Abhishek Srivastava
More from Abhishek Srivastava (11)
Medication Error as per 5th Edition Standard of NABH
Medication Error as per 5th Edition Standard of NABH
Invasive Bedside Procedure Verification Checklist or Bedside Invasive Procedu...
Invasive Bedside Procedure Verification Checklist or Bedside Invasive Procedu...
Documentation needed by treating consultant & doctor as per standards of ...
Documentation needed by treating consultant & doctor as per standards of ...
Recently uploaded
(Deeksha) 💓 9920725232 💓High Profile Call Girls Navi Mumbai You Can Get The Service Of A Mumbai Call Girl At Any Time
WHATSAPP On Here:9920725232
Today call girl service available 24X7*▬█⓿▀█▀ 𝐈𝐍𝐃𝐄𝐏𝐄𝐍𝐃𝐄𝐍𝐓 CALL 𝐆𝐈𝐑𝐋 𝐕𝐈𝐏 𝐄𝐒𝐂𝐎𝐑𝐓 SERVICE ✅
⭐➡️HOT & SEXY MODELS // COLLEGE GIRLS
AVAILABLE FOR COMPLETE ENJOYMENT WITH HIGH PROFILE INDIAN MODEL AVAILABLE HOTEL & HOME
★ SAFE AND SECURE HIGH CLASS SERVICE AFFORDABLE RATE
★ 100% SATISFACTION,UNLIMITED ENJOYMENT.
★ >> 03-05-2024 (GRV)
★ All Meetings are confidential and no information is provided to any one at any cost.
★ EXCLUSIVE PROFILes Are Safe and Consensual with Most Limits Respected
★ Service Available In: - HOME & HOTEL 24x7 :: 3 * 5 *7 *Star Hotel Service .In Call & Out call SeRvIcEs :
★ A-Level (5 star escort)
★ Strip-tease
★ BBBJ (Bareback Blowjob)Receive advanced sexual techniques in different mode make their life more pleasurable.
★ Spending time in hotel rooms
★ BJ (Blowjob Without a Condom)
★ Completion (Oral to completion)
★ Covered (Covered blowjob Without condom
100% SAFE AND SECURE 24 HOURS SERVICE AVAILABLE HOME AND HOTEL SERVICES(Deeksha) 💓 9920725232 💓High Profile Call Girls Navi Mumbai You Can Get The S...
(Deeksha) 💓 9920725232 💓High Profile Call Girls Navi Mumbai You Can Get The S...Ahmedabad Call Girls
Recently uploaded (20)
Rajkot Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Rajkot Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
raisen Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
raisen Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
bhubaneswar Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
bhubaneswar Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Jalna Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Jalna Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
nagpur Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
nagpur Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Best Lahore Escorts 😮💨03250114445 || VIP escorts in Lahore
Best Lahore Escorts 😮💨03250114445 || VIP escorts in Lahore
Premium Call Girls Bangalore {7304373326} ❤️VVIP POOJA Call Girls in Bangalor...
Premium Call Girls Bangalore {7304373326} ❤️VVIP POOJA Call Girls in Bangalor...
Call Girl in Bangalore 9632137771 {LowPrice} ❤️ (Navya) Bangalore Call Girls ...
Call Girl in Bangalore 9632137771 {LowPrice} ❤️ (Navya) Bangalore Call Girls ...
Russian Call Girls in Noida Pallavi 9711199171 High Class Call Girl Near Me
Russian Call Girls in Noida Pallavi 9711199171 High Class Call Girl Near Me
bhopal Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
bhopal Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
ooty Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
ooty Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Mangalore Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Mangalore Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Muzaffarpur Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Muzaffarpur Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Jaipur Call Girls 9257276172 Call Girl in Jaipur Rajasthan
Jaipur Call Girls 9257276172 Call Girl in Jaipur Rajasthan
Sambalpur Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Sambalpur Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Call Girls in Udaipur Girija Udaipur Call Girl ✔ VQRWTO ❤️ 100% offer with...
Call Girls in Udaipur Girija Udaipur Call Girl ✔ VQRWTO ❤️ 100% offer with...
Tirupati Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Tirupati Call Girls 👙 6297143586 👙 Genuine WhatsApp Number for Real Meet
Krishnagiri call girls Tamil Actress sex service 7877702510
Krishnagiri call girls Tamil Actress sex service 7877702510
(Deeksha) 💓 9920725232 💓High Profile Call Girls Navi Mumbai You Can Get The S...
(Deeksha) 💓 9920725232 💓High Profile Call Girls Navi Mumbai You Can Get The S...
Kolkata Call Girls Miss Inaaya ❤️ at @30% discount Everyday Call girl
Kolkata Call Girls Miss Inaaya ❤️ at @30% discount Everyday Call girl
Deceleration form related to travel history & health condition in view of outbreak of COVID - 19
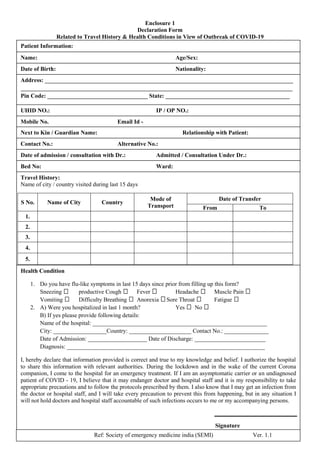
- 1. Enclosure 1 Declaration Form Related to Travel History & Health Conditions in View of Outbreak of COVID-19 Ref: Society of emergency medicine india (SEMI) Ver. 1.1 Patient Information: Name: Age/Sex: UHID NO.: IP / OP NO.: Date of admission / consultation with Dr.: Admitted / Consultation Under Dr.: Bed No: Ward: Date of Birth: Nationality: Mobile No. Email Id - Next to Kin / Guardian Name: Relationship with Patient: Contact No.: Alternative No.: Travel History: Name of city / country visited during last 15 days S No. Name of City Country Mode of Transport Date of Transfer From To 1. 2. 3. 4. 5. Health Condition 1. Do you have flu-like symptoms in last 15 days since prior from filling up this form? Sneezing productive Cough Fever Headache Muscle Pain Vomiting Difficulty Breathing Anorexia Sore Throat Fatigue 2. A) Were you hospitalized in last 1 month? Yes No B) If yes please provide following details: Name of the hospital: ___________________________________________________________ City: __________________Country: _____________________ Contact No.: _______________ Date of Admission: ____________________ Date of Discharge: ________________________ Diagnosis: ___________________________________________________________________ I, hereby declare that information provided is correct and true to my knowledge and belief. I authorize the hospital to share this information with relevant authorities. During the lockdown and in the wake of the current Corona companion, I come to the hospital for an emergency treatment. If I am an asymptomatic carrier or an undiagnosed patient of COVID - 19, I believe that it may endanger doctor and hospital staff and it is my responsibility to take appropriate precautions and to follow the protocols prescribed by them. I also know that I may get an infection from the doctor or hospital staff, and I will take every precaution to prevent this from happening, but in any situation I will not hold doctors and hospital staff accountable of such infections occurs to me or my accompanying persons. Address: ____________________________________________________________________________________ ____________________________________________________________________________________________ Pin Code: __________________________________ State: __________________________________________ Signature