
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Fracture neck femur
Similar to Fracture neck femur (20)
Recently uploaded
Recently uploaded (20)
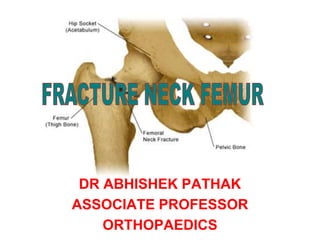
Fracture neck femur
- 1. DR ABHISHEK PATHAK ASSOCIATE PROFESSOR ORTHOPAEDICS
- 2. ANATOMY NORMAL NECK SHAFT ANGLE IS 135 DEGREE
- 3. ANTEVERSION = 10 ± 7º
- 4. CALCAR FEMORALE • Calcar femorale is a Condensed plate of bone extending from lesser trochanter to greater trochanter posteromedially
- 6. Figure 2 Computer-generated image demonstrates the orientation of the load-bearing trabeculae of the proximal femur, including the vertically oriented primary compressive trabeculae (red lines), the more horizontally oriented primary tensile trabeculae (black lines), and obliquely oriented secondary compressive trabeculae (yellow lines). The intervening trabecular bone between the medially converging compressive trabeculae is known as the Ward triangle (yellow triangle), a site of relative weakness. Sheehan SE. Published Online: July 17, 2015 https://doi.org/10.1148/rg.2015140301
- 7. FRACTURE NECK OF FEMUR Variously called as • The unsolved fracture • Fracture of necessity WHY
- 8. • EVEN WITH A GOOD REDUCTION AND FIXATION ABOUT 30% GO INTO NON-UNION / AVN • SURGEON HAS SOME CONTROL OVER NON-UNION BUT NOT OVER AVN • INCIDENCE OF NON-UNION CAN BE GREATLY REDUCED BY EARLY REDUCTION AND INTERNAL FIXATION • AVN DEPENDS ON THE INITIAL TRAUMA AND DISPLACEMENT OF THE FRACTURE
- 9. REASONS FOR NON UNION 1. INTRA-ARTICULAR FRACTURE THUS SYNOVIAL FLUID A DETERRENT TO # UNION 2. VASCULARITY PRECARIOUS 3. PERIOSTEUM IS LACKING THUS THE UNION IS ENDOSTEAL 4. # SUBJECTED TO HIGH SHEARING FORCES 5. BONE QUALITY MAY NOT BE GOOD
- 10. BLOOD SUPPLY • Lateral epiphysel artery – terminal branch MFC artery – predominant blood supply to weight bearing dome of head • Artery of ligamentum teres – from obturator artery – supplies anteroinferior head • Lateral femoral circumflex a. – less contribution than MFC
- 11. Figure 3 Computer-generated image demonstrates the vascular anatomy of the proximal femur. Blood flow to the proximal femur is supplied primarily by the branches of the medial and lateral circumflex femoral arteries. Supplemental flow to the femoral head is supplied by the artery of the ligamentum teres, a branch of the obturator artery. Green oval = transition point between the extracapsular and intracapsular portions of the ascending cervical retinacular arteries; yellow circle = lateral aspect of the femoral head-neck junction, a vulnerable zone where injury poses a substantial risk of clinically significant vascular compromise.
- 13. • Three ligaments in this region 1) Ileofemoral 2) Pubofemoral 3) Ischiofemoral
- 16. • 1575- Ambroise Pare described I/C # neck femur • 1850- Lagenbeck nails a hip • 1904- Whitman’s reduction and spica cast • 1931- Smith-Peterson used his triflanged nail • 1936- Moore’s pin and Knowle’s pin • 1943- Moore’s prosthesis • 1952- Thompson’s prosthesis • 1960- Charnley’s Total Hip Arthroplasty
- 17. EPIDEMOLOGY • Common fracture to occur in old female usually due to post menopausal osteoporosis • Average year of occurrence is 60-70 • Young adults are involved in high energy trauma
- 18. Risk factors include 1. Female sex 2. Alcohol and tobacco use 3. Previous # 4. Low estrogen level
- 19. MECHANISM • Low energy trauma in elderly patients –Direct: Fall on GT or forced ext. Rotation –Indirect : Muscle forces overwhelming bone strength • High energy trauma : RTA, Fall from height • Cyclical loading can cause stress fractures
- 20. Clinical evaluation • H/o trivial trauma after which the patient is non ambulatory • Pt. with impacted fracture may bear weight • ½ to 1 cm of shortening • Limb in mild ext. rotation as compared to normal limb • Pain in groin • Tenderness at the base of Scarpa’s Triangle • Pain on hip movt. • Axial tenderness
- 21. Inguinal Ligament Medial border of adductor longus Medial border of sartorius
- 22. IMAGING • X-ray pelvis with both hips AP view • X-ray of affected hip AP and Lateral view • Internal rotation AP views • Tech. Bone Scan • MRI
- 24. PAUWELS CLASSIFICATION • ANGLE THAT FRACTURE LINE SUBSTANDS WITH THE HORIZONTAL
- 25. Garden Classification I - Incomplete or Impacted II - Complete no displacement III - Complete with partial displacement IV- Complete with total displacement
- 26. GARDENS CLASSIFICATION • GARDEN’S TYPE I
- 27. • GARDEN’S TYPE II
- 28. • GARDEN’S TYPE III
- 29. • GARDEN’S TYPE IV
- 31. SHENTON’S LINE
- 32. SHENTON’S LINE
- 34. • Minimize patient’s discomfort • Restore hip function • Allow rapid mobilization by early reduction and internal fixation so as to avoid problems of long term recumbency
- 35. NON OPERATIVE TREATMENT • No place in todays time • Recommended only for patients who are at extreme medical risk, moribund or demented nonambulators
- 37. DISPLACED FRACTURE IN YOUNG ADULTS • # LESS THAN 3 WEEKS OLD • OPEN OR CLOSED ANATOMIC REDUCTION WITH STABLE INTERNAL FIXATION WITH a) 6.5 mm CCS, optimum 3 in number b) DHS with a derotation screw
- 38. DHS with a derotation screw
- 39. 6.5 mm CCS, optimum 3 in number
- 40. FRACTURES IN CHILDREN • Closed reduction and internal fixation with a) Moore’s pin b) Knowles pin Followed by spica cast immobilization
- 42. CRITERIA FOR ANATOMIC REDUCTION • Garden’s criteria : Trebacular angle on AP and Lat. view should be within the range of 160-180 deg. • Lovetts “LAZY S” criteria
- 44. FRACTURE > 3 WK. OLD • OSTEOTOMIES: McMurray’s Valgus angulation Provide arm chair effect
- 45. 1. MUSCLE PEDICLE GRAFT 1. Meyer’s quadratus femoris pedicle 2. Bakshi’s TFL pedicle graft 2. GIRDLESTONE EXCISION ARTHROPLASTY 3. ARTHRODESIS 4. ORIF WITH FIBULAR GRAFT
- 46. # N/F IN ELDERLY > 60 YRS • Physiological age is important. • HEMIARTHROPLASTY UNIPOLAR : 1) Austin Moore prosthesis 2) Thompson prosthesis BIPOLAR PROSTHESIS • THR- when acetabular erosion is present
- 49. THR
- 50. STRESS FRACTURE
- 51. COMPLICATIONS • Non union • AVN • Limb length dicrepency