Pelvic inflammatory disease (pid)
Pathophysiology Acute inflammation of the upper genital tract – the uterus or adnexa – from an ascending infection – usually chlamydia or gonorrhea (25%). May lead to epithelial damage thus allowing further pathogen entry. Involves any combination of endometritis, salpingitis, tubo-ovarian abscess, or pelvic peritonitis. Rarer causes: Gardnerella vaginalis, H. influenzae, Strep agalactiae (Group B Strep), CMV. Often no pathogen is found. Signs and symptoms Symptoms: Varies from asymptomatic to severe. Pain: lower abdominal (often bilateral), lower back, and deep dyspareunia. Systemic: fever, nausea and vomiting. Discharge and bleeding: cervical or vaginal mucopurulent discharge, postcoital or intermenstrual bleeding. On bimanual examination, tenderness in the uterus, adnexa, and cervix ('cervical excitation').

Recommended
More Related Content
Similar to Pelvic inflammatory disease (pid)
Similar to Pelvic inflammatory disease (pid) (20)
More from AayushPokharel10
More from AayushPokharel10 (20)
Recently uploaded
Recently uploaded (20)
Pelvic inflammatory disease (pid)
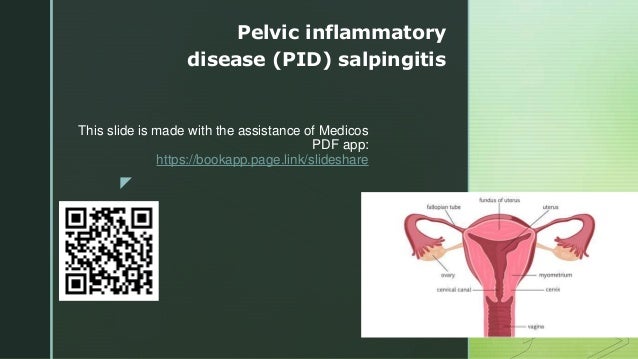
- 1. z This slide is made with the assistance of Medicos PDF app: https://bookapp.page.link/slideshare Pelvic inflammatory disease (PID) salpingitis
- 2. z Pathophysiology • Acute inflammation of the upper genital tract – the uterus or adnexa – from an ascending infection – usually chlamydia or gonorrhea (25%). May lead to epithelial damage thus allowing further pathogen entry. • Involves any combination of endometritis, salpingitis, tubo-ovarian abscess, or pelvic peritonitis. • Rarer causes: Gardnerella vaginalis, H. influenzae, Strep agalactiae (Group B Strep), CMV. • Often no pathogen is found.
- 4. z Signs and symptoms Symptoms: • Varies from asymptomatic to severe. • Pain: lower abdominal (often bilateral), lower back, and deep dyspareunia. • Systemic: fever, nausea and vomiting. • Discharge and bleeding: cervical or vaginal mucopurulent discharge, postcoital or intermenstrual bleeding. On bimanual examination, tenderness in the uterus, adnexa, and cervix ('cervical excitation').
- 5. z Risk factors • Sexually active, especially if unprotected. • History of STIs. • Age 18-25. • IUCD
- 6. z Investigations Initial tests: • Bloods: ↑WBC, ↑ESR/CRP. • Vaginal or endocervical swabs: send for chlamydia and gonorrhea nucleic acid amplification test. • Urine: rule out UTI, and pregnancy test to rule out ectopic.
- 7. z Investigations Optional further tests: • Transvaginal US may show fluid-filled fallopian tubes, endometrial thickening, or tubo-ovarian abscess. Also helps rule out other conditions. • Screen for other STIs. • Consider pelvic CT or MRI if severe. • Laparoscopy can help make the diagnosis and rule out alternative causes, but is invasive and not routinely used.
- 8. z Investigations Diagnosis: • Can often be made clinically, especially as swabs may be negative even if PID present. • However, PID is unlikely if WBC, ESR, and swabs are normal.
- 10. z Management Antibiotics: • Ceftriaxone IM once, then doxycycline PO ± metronidazole PO for 2 weeks. • If severe – >38°C, peritonitis, or abscess – give ceftriaxone IV + metronidazole IV + doxycycline PO, then switch to metronidazole PO + doxycycline PO. • Screen and treat sexual contacts. Also: • Analgesia • Consider removing IUCD, but balance against risks of pregnancy. • Repeat testing 3-6 months later to ensure no recurrence.
- 11. z Complications • Scarring and adhesions to nearby tissue or organs, causing chronic pain. • Tubo-ovarian abscess. • Fitz-Hugh Curtis syndrome (10%): RUQ pain due to perihepatitis. • Obstetric: infertility, ectopic pregnancy.
- 12. z Thank You Keep supporting Medicos PDF app. To find hundreds of books, slides and news visit the app. https://bookapp.page.link/slideshare