1. Peritoneum
General features
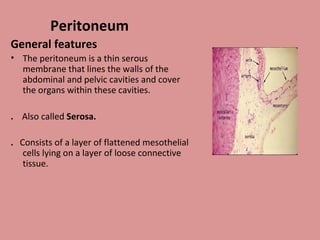
• The peritoneum is a thin serous
membrane that lines the walls of the
abdominal and pelvic cavities and cover
the organs within these cavities.
. Also called Serosa.
. Consists of a layer of flattened mesothelial
cells lying on a layer of loose connective
tissue.
2. LAYERS.
1.Parietal layer
lines the wall of abd. And pelvic cavities.
2.visceral layer
covers the organs
.
Peritoneal cavity
.is a potential space between the two layers of
peritoneum.
. filled with very thin film of serous fluid
secreted by the mesothelial cells.
.In the male, is a closed sac, but in the
female,it is open bcz of uterine tubes, the uterus, and the
vagina.
Extraperitoneal connective tissue.
Present b/w parietal layer and abd. and pelvic
walls.
3. • Peritoneal fluid
• Peritoneal fluid is pale yellow
fluid rich in leukocytes
• Mobile viscera glide easily on one
another.
• Peritoneal fluid moves upward
towards subphrenic spaces-
whatever the position of the
body- by:
• 1- Movements of diaphragm.
• 2- Movements of abdominal
muscles
• 3- Peristaltic movements
5. Divisions of peritoneal
cavity
It is divided into two main sacs:
1- Greater sac.
2- Lesser sac or omental bursa.
These two sacs are
interconnected by a single oval
opening called the epiploic
foramen or opening into lesser sac
or foramen of Winslow
6. The relationship between viscera and peritoneum
• Intraperitoneal viscera -
• viscera completely surrounded by peritoneum
• stomach, superior part of duodenum, jejunum, ileum, cecum, vermiform
appendix, transverse and sigmoid colons, spleen and ovary
• Retroperitoneal viscera
• - some organs lie on the posterior abdominal wall and are covered by peritoneum
on their anterior surfaces only.
Primary retroperitoneal organs
kidney
suprarenal gland
Aorta and ivc
Ureter
Rectum(lower third part)
10. Structures which are formed by peritoneum
.Peritoneal folds.
.Peritoneal ligaments.
. Falciform.
. rt and lt triangular.
.coronary.
.Omentum
stomach
. MESENTRY
Small intestine.
.Mesocolon
Transverse mesocolon
Sigmoid mesocolon
Meso appendix.
11. Peritoneum of liver
• The liver is almost completely
covered in visceral peritoneum, and
only the ‘bare area' is in direct
contact with the right dome of the
diaphragm. Peritoneal folds, the
ligaments of the liver, run from the
liver to the surrounding viscera and
to the abdominal wall
12. Peritoneum of
liver.
• Falciform ligament of
liver
Consists of double peritoneal
layer
– Sickle shape
– Extends from anterior
abdominal wall to liver just
rt to midline.
– Free border of the
ligament contains
Ligamentum teres
(obliterated umbilical vein)
13. Its two peritoneal layers divide to enclose the liver and
are continuous with the visceral peritoneum that is
adherent to the surface of the liver. Superiorly, they
are reflected onto the inferior surface of the diaphragm
and are continuous with the parietal peritoneum over
the right dome. At the posterior limit, or apex, of the
falciform ligament, the two layers are also reflected
vertically left and right, and are continuous with the
anterior layers of the left triangular ligament and the
superior layer of the coronary ligament of the liver.
14. Coronary ligament
• Peritoneum that lines the
under surface of diaphragm
is reflected on to superior
surface of rt lobe of liver
forming the upper layer of
coronary ligament
15. • Then, it descends from sup
surface of liver to ant surface
then inferior surface of liver.
• From post part of inferior
surface peritoneum reflected on
to front of right kidney & rt
suprarenal gland forming the
lower layer of coronary
ligament.
• The lower & upper layers of
coronary ligament bound a large
area on the post surface of the
liver called bare area of the liver
which has no peritoneal
covering.
16.
17.
18. Rt triangular ligament.
.Short v shaped fold.
.Formed by approximation of two
layers of coronary ligament on rt
lateral end.
Left triangular ligament.
.Double layer.
.On upper border of lt lobe.
.Upper layer continues with left
layer of falciform ligament.
.Lower layer with lt layer of lesser
omentum.
22. Greater omentum
- largest peritoneal fold which hangs inferiorly from the greater
curvature of stomach.
-double sheet,each sheet has two layers of peritoneumseparated by
scanty connective tissue.
Anterior sheet
Anterior layer
From ant surface of stomach and duodenum.
Posterior layer
From post surface of stomach and pylorus.
Two layers of anterior sheet decend from greater curvature to
a variable distance in peritoneal cavity
Ascend back on itself to form posterior sheet.
Posterior sheet
Anterior layer forms posterior wall of lesser sac.
Post layer passes infront of transvers colon n mesocolon n
attatched to t.mesocolon at its root to form gastrocolic
ligament.
23.
24. • Lesser Omentum
• Connects liver to stomach.
• attached above to porta
hepatis & fissure for
ligamentum venosum
inferiorly to lesser
curvature of the stomach,&
1st
inch of duodenum.
• Attatchment is L shaped.
• Forms ant wall of lesser
sac
• Its free margin contains:
Portal vein: Posterior
Bile duct : Anterior &
right
Hapatic artery: anterior and
left.
27. Omental bursa or lesse sac
It is a subsection of peritoneal cavity behind the stomach.
Position
- situated behind the lesser omentum and stomach
Walls
• Superior
• - peritoneum which covers the caudate lobe of liver and diaphragm
• Anterior
• - formed by lesser omentum, peritoneum of posterior wall of
stomach, and anterior two layers of greater omentum
• Inferior
• - conjunctive area of anterior and posterior two layers of greater
omentum.bcz of fusion cant extend much below transverse colon.
• Posterior
• - formed by posterior two layers of greater omentum, transverse
colon and transverse mesocolon, peritoneum covering pancreas, left
kidney and suprarenal gland
28. . Left -
formed by the spleen,
gastrosplenic and
splenorenal ligament
• Right -
formed by omental
foramen
The Omental bursa (lesser
sac) communicates with
the greater sac through
the omental foramen.
29.
30.
31. Epiploic Foramen
Boundaries
2.5cm vertical slit.
Anterior: free margin of lesser omentum, containing (hepatic artery, bile duct
and portal vein)
Posterior: peritoneum covering IVC.
Superior: Caudate process of the caudate lobe of the liver.
Inferior: 1st
inch of the1st
part of duodenum.
36. The spleen lies in the
left hypochondrium
between the stomach
and diaphragm.
It has two ends, three
borders and two
surfaces.
37.
38.
39.
40. pe :3 borders, 2 ends, 2
surfaces.
A. Ends
1) lateral end (Broad)
2) medial end (tapering)
B. Borders
Upper(Anterior) border:
Sharp & notched
Lower (Posterior)border:
(Broad)
Intermediate border:
thick, incomplete. Extends
from the medial end till
the hilum).
41.
42. Ligaments of spleen
• Gastrosplenic ligament -
a double layer of peritoneum that connects the
fundus and greater curvature of stomach to hilum of
spleen. Has two layers.ant and post.
• Splenorenal ligament
• - extends between the hilum of spleen and anterior
aspect of left kidney. The splenic vessels lies within this
ligament, as well as the tail of pancreas
• Phrenicosplenic ligament
• Splenocolic ligament
• Phrenicocolic ligament.
43. If the peritoneal attachments of the spleen are not recognized
during surgery, the splenic capsule is at risk of injury and there
may be subsequent serious bleeding. Downward traction on
the phrenicocolic ligament during handling of the descending
colon, especially during mobilization of the splenic flexure, may
cause rupture of the splenic capsule. This is less likely if
traction on the phrenicocolic ligament is made laterally or
medially. The superior border and anterior diaphragmatic
surface of the splenic capsule are often adherent to the
peritoneum of the greater omentum. Medial traction on the
omentum during surgery may cause splenic capsular injury:
such injury is less likely, if any limited traction required is
applied inferiorly
49. Transverse mesocolon - a double fold of peritoneum reflected
from post abd wall and suspends the transverse colon in the
peritoneal cavity.
• Root of t.mesocolon.
• Lies along an oblique line passing from ant aspect of 2nd
part of
duodenum,over the head and neck of pancreas,above the
duodenojejunal junctionn over the upper pole of left kidney to the
splenic flexure.
• Contains middle colic vessels together with the branches of sup
mesenteric plexus,lymphatics and regional lymph nodes.
• Two layers from post abd wall reach on post surface of colon,cover it
then upper layer becomes continues with the post.layer of
g.omentum to which it is adherent.
• Lower layer continues with peritoeum of post.abd wall.
50.
51.
52.
53.
54. Extension of t.mesocolon.
• Duodenocolic ligament
From hepatic flexure to 2nd
part of duodenum.
• Phrenicocolic ligament.
From splenic flexure to diaphragm at level of
11th
rib.
55.
56.
57.
58.
59. Mesentery of small intestine
• Fan shaped with two layers anterosup and
posteroinf separated by c.t. and vessels.
• Root of mesentry.
• A diagonal line from duodenojej flexure on the left
of 2nd
lumber vert body to the rt sacroiliac joint.
• Length is 15cm in adults.n 6 meter when cover
intestineal loops.
• Its two layers contain sup.mesenteric vessels.
60. Mesoappendix
• Triangular mesentery -
extends from terminal
part of ileum to appendix
• Appendicular artery runs
in free margin of the
mesoappendix
61.
62.
63.
64.
65.
66. Divisions of peritoneal cavity
• The greater sac can be divided into two
compartments.
• Supracolic or supramesocolic
• Infracolic or inframesocolic
67.
68. Supramesocolic
The supramesocolic space lies above the transverse
mesocolon between the diaphragm and the transverse
colon.
divided into right and left supramesocolic spaces.
The right supramesocolic space can be divided
into three subspaces;
the right subphrenic space,
the right subhepatic space,
the lesser sac..
69. Right subphrenic space
lies between the diaphragm and the anterior,
superior and right lateral surfaces of the right lobe of the liver
Boudaries
left --------- ( falciform ligament )
behind ---------(upper layer of the coronary
ligament.)
clinical imp
common site for collections of fluid after right sided abdominal
inflammation.
70.
71.
72. The right subhepatic space
lies between the right lobe of the liver and
the right kidney.
Boundaries
--superiorly ( inferior layer of the coronary ligament)
-- laterally ( right lateral abdominal wall,)
--posteriorly ( anterior surface of the upper pole of the
right kidney)
--medially ( second part of the duodenum, hepatic flexure,
transverse mesocolon and part of the head of the pancreas.
Clinical imp.
In the supine position the posterior right subhepatic space is
more dependent than the right paracolic gutter: postoperative
infected fluid collections are common in this location
73.
74.
75.
76.
77. The left supramesocolic space
• can be divided into two subspaces; the left
subphrenic space and the left perihepatic
space
78. Left subphrenic space
lies between the diaphragm, the anterior and superior surfaces of the left lobe of
the liver, the anterosuperior surface of the stomach and the diaphragmatic surface of the
spleen.
boundaries
right by the falciform ligament
behind by the anterior layer of the left triangular ligament.
Clinical imp
---- It is much enlarged in the absence of the spleen and is a common
site for fluid collection particularly after splenectomy.
-----larger than the right and divided into anterior and posterior parts, although
no obvious demarcation exists in the absence of disease.
-----The left posterior subphrenic space is small and lies between the fundus of
the stomach and the diaphragm above the origin of the splenorenal ligament.
------The left anterior subphrenic space is large and lies between the superior
and anterolateral surfaces of the spleen and the left dome of the diaphragm.
Inferiorly and medially, this space is bounded by the splenorenal, gastrosplenic,
and phrenicocolic ligaments which produces a partial barrier to the left
paracolic gutter.
------- This may explain why left subphrenic collections are less frequent than
right subphrenic collections following lower abdominal and pelvic surgery, but
the left subphrenic space is the commonest site of fluid collection after upper
79.
80. Left perihepatic space
• The left perihepatic space is sometimes subdivided into
anterior and posterior spaces.
• The posterior perihepatic space is also known as the left
subhepatic space or gastrohepatic recess.
• The left anterior perihepatic space lies between the
anterosuperior surface of the left lobe of the liver and
diaphragm. The left posterior perihepatic space lies inferior
to the left lobe of the liver, and extends into the fissure for
the ligamentum venosum on the right, anterior to the main
portal vein. Posteriorly, the lesser omentum separates this
space from the superior recess of the lesser sac. On the
left, the space is bounded by the lesser curvature of the
stomach.
81. INFRAMESOCOLIC COMPARTMENT
. lies below the transverse mesocolon and transverse
colon are far as the true pelvis.
.divided in two unequal spaces by the root of the
mesentery of the small intestine.
. contains the right and left paracolic gutters lateral to the
ascending and descending colon. As a consequence of the
mobility of the transverse mesocolon and mesentery of
the small intestine, disease processes are rarely well
contained within these spaces, and fluid within the
infracolic space tends to descend into the pelvis or the
paracolic gutters
82.
83. Right infracolic space
The right infracolic space is a triangular space. It is smaller than
its counterpart on the left, and lies posterior and inferior to the
transverse colon and mesocolon and to the right of the small
intestinal mesentery. The vermiform appendix often lies in the
lower part of the right infracolic space.
Left infracolic space
The left infracolic space is larger than its counterpart on the right
and is in free communication with the pelvis to the right of the
midline. It lies posterior and inferior to the transverse colon and
mesocolon and to the left of the mesentery of the small intestine.
The sigmoid colon and its mesentery may partially restrict the flow
of fluid or blood into the pelvis to the left of the midline
84. Paracolic gutters
..right and left paracolic gutters are peritoneal recesses
on the posterior abdominal wall lying alongside the
ascending and descending colon.
The right (lateral) paracolic gutter runs from the
superolateral aspect of the hepatic flexure of the colon,
down the lateral aspect of the ascending colon, and
around the caecum. It is continuous with the peritoneum
as it descends into the pelvis over the pelvic brim.
Superiorly, it is continuous with the peritoneum which
lines the hepatorenal pouch and, through the epiploic
foramen, the lesser sac.
85. Clinical importance
• Bile, pus or blood released from viscera anywhere along its
length may run along the gutter and collect in sites quite
remote from the organ of origin. In supine patients,
infected fluid from the right iliac fossa may ascend in the
gutter to enter the lesser sac. In patients nursed in a sitting
position, fluid from the stomach, duodenum or gallbladder
may run down the gutter to collect in the right iliac fossa or
pelvis and may mimic acute appendicitis or form a pelvic
abscess. The right paracolic gutter is larger than the left,
which together with the partial barrier provided by the
phrenicocolic ligament, may explain why right subphrenic
collections are more common than left subphrenic
collections
86.
87.
88. Because the peritoneum of the falciform ligament
is continuous with that covering the posterior
abdominal wall and the periumbilical anterior
abdominal wall, blood arising from retroperitoneal
haemorrhage (commonly acute haemorrhagic
pancreatitis) may track between the folds of
peritoneum and appear as haemorrhagic
discolouration around the umbilicus (Cullen's
sign). Inflammatory change from the pancreas
may spread via the gastrohepatic ligament (lesser
omentum) and then via the falciform ligament to
the umbilicus
89. The recess formed between the peritoneum
of the inferior surface of the liver, the
hepatorenal ligament and the peritoneum
over the right kidney is known as the
hepatorenal pouch (of Morison). In the
supine position this is the most dependent
part of the peritoneal cavity in the upper
abdomen, and is a common site of
pathological fluid accumulation.
90. Folds and fossas of anterior abdominal wall
• Medial umbilical fold -
contain the remnant of
urachus (median umbilical
ligaments)
• Medial umbilical fold -
contains remnants of the
umbilical arteries (medial
umbilical ligaments)
• Lateral umbilical fold -
contains the inferior
epigastric vessels
• Supravesical fossa
• Medial inguinal fossa
• Lateral inguinal fossa
91. Folds and fossas of anterior abdominal wall
• Medial umbilical fold -
contain the remnant of
urachus (median umbilical
ligaments)
• Medial umbilical fold -
contains remnants of the
umbilical arteries (medial
umbilical ligaments)
• Lateral umbilical fold -
contains the inferior
epigastric vessels
• Supravesical fossa
• Medial inguinal fossa
• Lateral inguinal fossa