Downloaded 26 times


















The document discusses HIV self-testing among gay and bisexual men in Australia, highlighting testing rates, barriers to testing, and the potential benefits of self-testing. It emphasizes the high acceptability and ease of use of self-testing kits, citing overseas studies, and addresses TGA requirements for approval. Additionally, it outlines current self-testing products, their performance, and the interest among the target population for increased accessibility to self-testing options.
Introduction to HIV self-testing by A/Prof Rebecca Guy from The Kirby Institute, UNSW Australia.
Overview of HIV testing rates among gay and bisexual men, emphasizing guidelines and statistics related to undiagnosed infections.
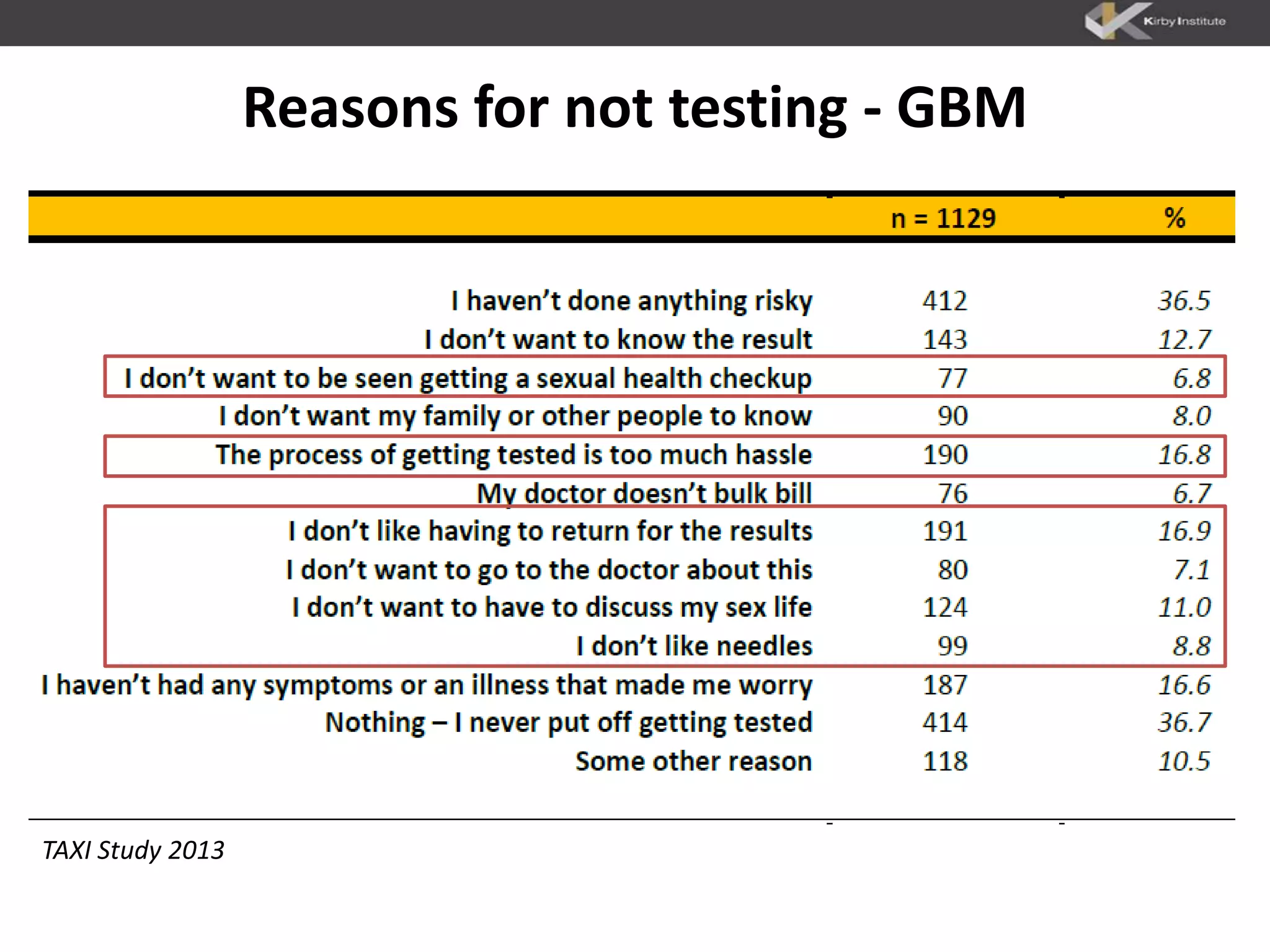
Identifies key reasons why gay and bisexual men and culturally and linguistically diverse groups do not get tested.
Discusses public health benefits and partner testing advantages with HIV self-tests, highlighting high response rates from high-risk groups.
Demographic data on Australian gay and bisexual men's interest in self-testing, with significant percentages showing willingness to test and purchase.
High acceptability of self-testing among users reported, with a focus on ease of use and lack of harm.
Outline of proposed TGA requirements for HIV self-tests, emphasizing sensitivity, ease of use, and important precautions.
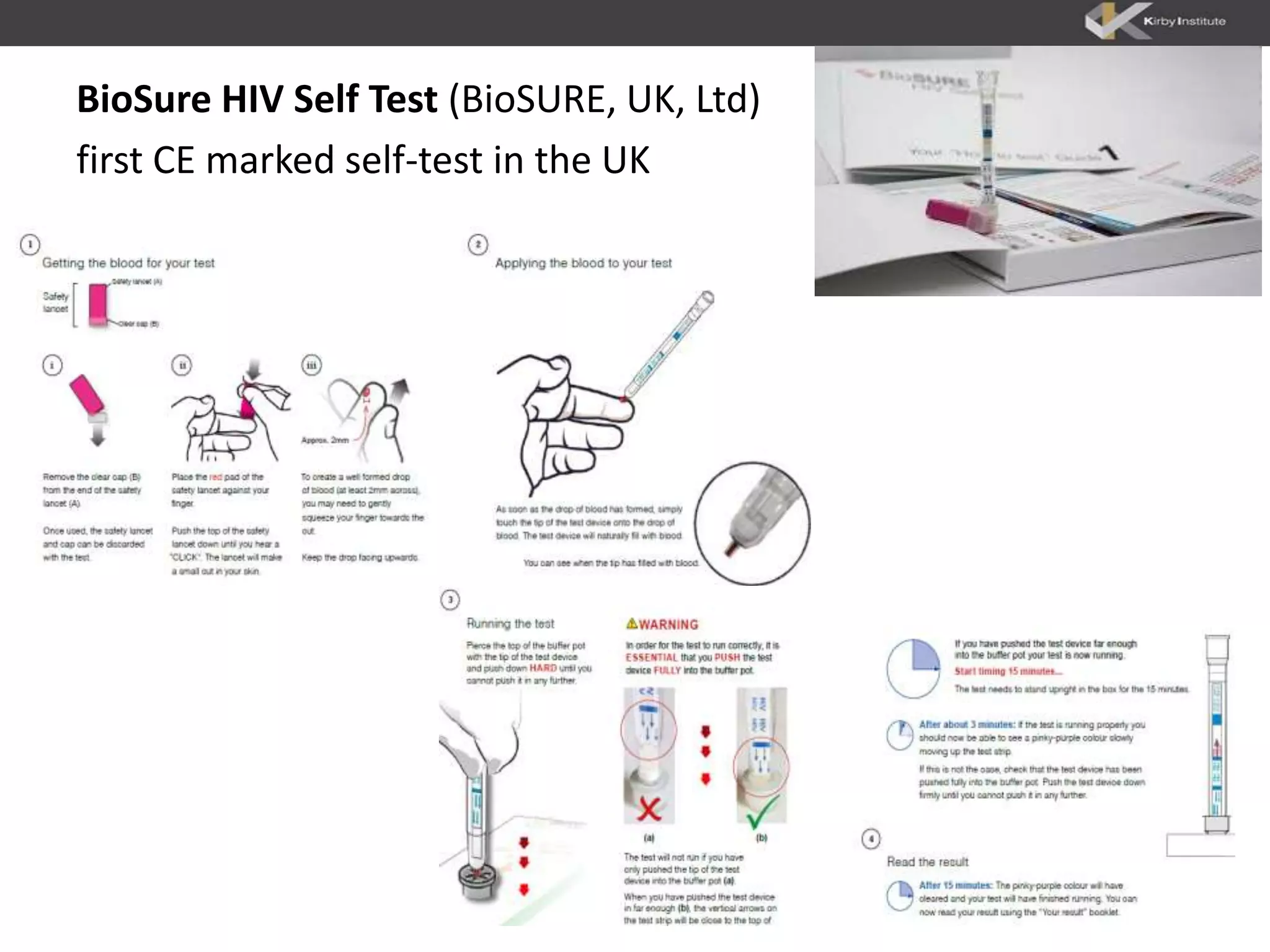
Examples of HIV self-test kits approved in other countries, including OraQuick and BioSure.
Comparison of OraQuick and BioSure details such as sensitivity, specificity, and performance statistics for self-testing.
Findings from an unobserved study indicating willingness of HIV-positive users to seek follow-up care.
Discussion on the role of self-testing as supplementary to existing testing practices among gay and bisexual men.
Analysis of the affordability and willingness to pay for self-tests among gay and bisexual men in different countries.
List of organizations involved in the HIV self-testing research and promotion, showing collaborative efforts.
Description of study design to assess the impact of HIV self-testing on testing frequency and acceptability.
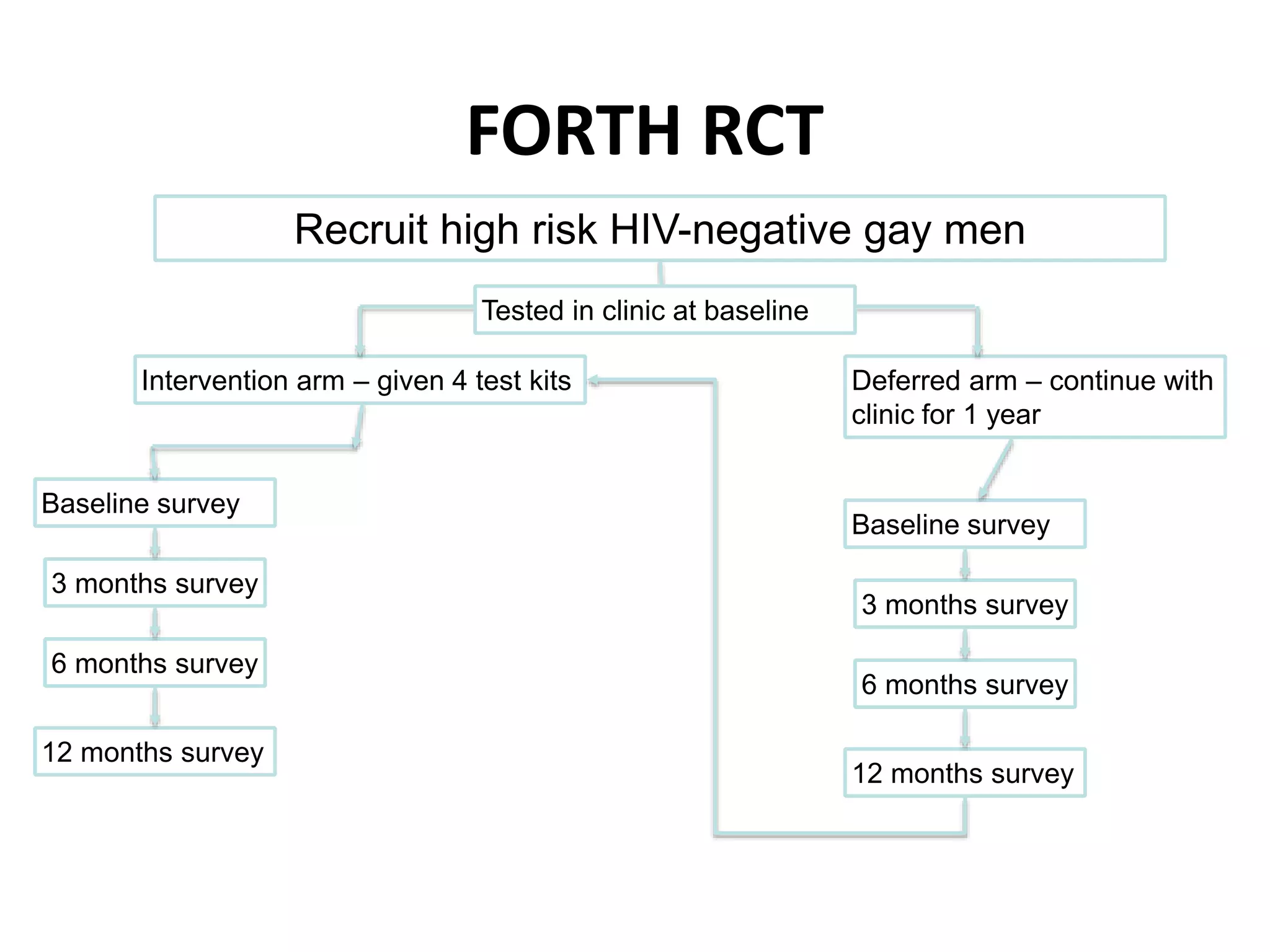
Details on the FORTH randomized control trial's structure, including participant recruitment and survey methods.
Final remarks emphasizing the potential of HIV self-testing in Australia, with a focus on interest and acceptability.



































































