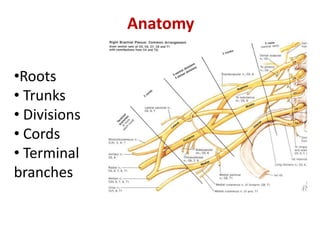
2. Roots
•Ventral rami of
C5-C8
and the greater
part of
T1 form the
roots of the
brachial
plexus
• Variable
contributions from
C4 and T2
3. Trunks
•C5 and C6 nerve
roots take a lateral
course together
and unite to form
the superior trunk
• C7 nerve root
becomes the
middle trunk
• C8 and T1 nerve
roots unite to form
the inferior trunk
4. •At the lateral border of the first rib and behind the
middle third of the clavicle, the trunks divide into
anterior and posterior divisions.
• Anterior division -supply flexors
•Posterior division - supply extensors
• The divisions continue the journey down into the
apex of the axilla where they further reorganize into
cords
Divisions
5. Cords
The cords are named
according to their
relationship to the
axillary artery
• The anterior divisions
of the superior and
middle trunks form the
lateral cord
• The anterior division
of the inferior trunk
forms the medial cord
• The posterior
divisions of all three
trunks forms the
Posterior cord
6.
7. Cords
The cords complete the journey at the lateral
border of the pectoralis minor where they give
rise to the terminal branches of the brachial
plexus
8. Terminal branches
Each cord gives rise to two
major terminal branches
and a variable number of
minor branches.
• Lateral cord
musculocutaneous n.
lateral root of median n.
• Medial cord
ulnar n.
medial root of median n.
• Posterior cord
axillary n.
Radial n.
9. FROM ROOT
• LONG THORACIC NERVE(5,6,7)
INNERVATES: SERRATUS ANTERIOR
• DORSAL SCAPULAR NERVE(C5)
INNERVATES: RHOMBOIDEUS MAJOR
RHOMBOIDEUS MINOR
• A branch to join PHRENIC NERVE(C5)
• Muscular branches to longus colli and scaleni
11. Musculocutaneous
Course: branches to arm, distal to elbow
becomes cutaneous for lateral forearm
skin
Innervates
Biceps brachii, brachialis,
coracobrachialis (motor inn)
Skin distal to elbow (sensory)
Innervation by Lateral Cord
12. Median
Course: middle of brachial plexus, does not
branch in arm, distal to elbow provides many
branches to most forearm flexors, passes through
carpal tunnel to hand to lateral palmar intrinsics
Innervates: most muscles of anterior forearm
(motor inn)
(eg) most flexors, some intrinsics (thumb)
Innervates: skin of lateral 2/3 hand on palm side,
dorsum of fingers 2+3 (sensory inn)
Nerve Damage = “Ape” Hand
Inability to Oppose Thumb
Innervation by both Lateral and Medial Cords
13. Ulnar
Course: runs along medial side of arm, behind
medial epicondyle, superficial to carpal tunnel into
hand, branches to supply intrinsics and skin
Innervates:
FCU and part of FDP, most intrinsics (motor inn)
Skin of medial 2/3 of hand A+P (sensory inn)
Nerve Damage: Clawhand
Inability to extend fingers at interphalangeal
joints, results in permanent flexion = claw
Innervation by Medial Cord
14. Radial Nerve (largest branch)
Course: Through arm, around humerus, around
lateral epicondyle, then divides
Innervates: all posterior muscles of arm and forearm
Triceps brachii, anconeus, supinator,
brachioradialis
Divides in forearm:
Superficial = skin of arm and dorsolateral surface
of hand
Deep = extensor muscles of forearm (eg E. carpi
radialis L + B)
Damage to Radial Nerve = wristdrop
Inability to extend the hand, inability to fully
extend forearm
Innervation by Posterior Cord
15. Axillary Nerve (runs w/ posterior humeral
circumflex a.)
Innervates:
Deltoid and Teres minor (motor inn)
Capsule of shoulder, skin of shoulder (sensory
inn)
INJURY TO AXILLARY NERVE-INABILITY TO ABDUCT ARM
WITH LOSS OF SENSATION OVER LOWER PART OF DELTOID
Subscapular Nerve {branches of C5 + C6 rami}
Innervates: Subscapularis, Teres major
Thoracodorsal Nerve (runs w/thoracodorsal a+v)
Innervates: Latissimus dorsi
17. Upper Brachial Plexus
Injuries
• Increase in angle
between neck
&shoulder
• Traction (stretching
or avulsion) ofupper
ventral rami (e.g.,
C5,C6)
•During anaesthesia
• Produces Erb’s Palsy
18. Lower Brachial
Plexus Injuries
• Excessive
upward pull of
limb
• Traction
(stretching or
avulsion) of lower
ventral rami (e.g.,
C8, T1)
• Produces
Klumpke’s Palsy
HORNER’S
SYNDROME
19. “Obstetrical” or “Birth palsy”
• Becoming increasingly rare
• Categorized on basis of damage
• Upper (C5,6), Erb’s: 60-90%
• All (C5-T1), both palsies: 10%
• Lower (C8, T1), Klumpke’s Palsy1-5%
20. • INJURY TO LONG THORACIC NERVE-(N. OF
BELL) WINGING OF SCAPULA
• INJURY TO LATERAL CORD- DISLOCATION OF
HUMERUS-
• DEFORMITY-MIDPRONE FOREARM
• LOSS OF FLEXION AT WRIST & FOREARM
• SENSORY LOSS ON RADIAL SIDE OF
FOREARM
• VASOMOTOR AND TROPHIC CHANGES
21. • INJURY TO MEDIAL CORD
• CAUSE-SUBCORACOID DISLOCATION
• DEFORMITY -CLAW HAND
• SENSORY LOSS ON ULNAR SIDE OF FOREARM
• VASOMOTOR AND TROPHIC CHANGES