
Recommended
Recommended
More Related Content
Similar to 5 annotated bibliographies #1 As much as we try to preve.docx
Similar to 5 annotated bibliographies #1 As much as we try to preve.docx (16)
More from troutmanboris
More from troutmanboris (20)
Recently uploaded
Recently uploaded (20)
5 annotated bibliographies #1 As much as we try to preve.docx
- 1. 5 annotated bibliographies #1 As much as we try to prevent them, medication errors happen everyday. It is especially common in skilled nursing facilities because many of them still use paper charts for medication administration or documentation and do not have access to the newer technology that other medical facilities do. According to a study performed in 2014, medication distribution technology has been proven to be effective in automatically detecting medication errors so that nurses can have more of an opportunity to focus on their patients. Working on a long-term care unit, most of my time is spent passing medications and doing treatments since I have 19 residents to tend to. Depending on how “smooth” the night goes, I sometimes do not get a chance to spend that extra time with my residents as I would like to. This medication distribution technology includes a mobile medication dispensing cart for long-term care units. The medications would be pre-packed for each patient by the pharmacy and able to be dispensed when needed. This would allow nurses to provide more one-on-one time with their patients while also increasing the prevention of medication errors. It also will help to lighten the nurses’ workload. Research shows that
- 2. these mobile medication cart have been successful. Medication error rates decreased from 2.9% to 0.6% (Baril, Gascon & Brouillette, 2014). Reference Baril, C., Gascon, V., & Brouillette, C. (2014). Impact of technological innovation on a nursing home performance and on the medication-use process safety. Journal of Medical Systems, 38(3), 1–12. https://library.neit.edu:2404/10.1007/s10916-014-0022-4 #2 Adverse drug effects due to medication errors are estimated to cost the United States $2 billion every year. After reviewing patient reports and reviewing charts, it was discovered that 44% of these occur after the prescription was written. These errors were found to be from registered nurses, licensed practical nurses and pharmacy technicians. Therefore, the problem comes from administration of the medication. However, these numbers only account for the errors that are actually reported. It is the more serious and harmful errors that are recorded, probably because they are harder to hide. The Health Care Finance Administration of the United States made it
- 3. standard for hospitals and skilled nursing facilities to have no more than 5% of medication error rates a year. In a study conducted in 2014, researchers decided to put a hold on reviewing incident reports and patient charts. Instead, they decided to directly observe medication administration over 20 different hospitals or skilled nursing facilities. Other methods included: attending medical rounds to see if a medication error had occurred, interviewing health care workers to see if they would report anything, testing patients urine to see if they had any unauthorized medications in their system, and comparing medication administration records with the physician’s order (Flynn, Barker, Pepper, Bates & Mikeal, 2014). I think these methods are effective in detecting medication errors as well as having the healthcare workers realize how often these errors actually do occur and that they should always perform their tasks as if they are always being directly observed. Reference Flynn, E.A., Barker, K.N., Pepper, G.A., Bates, D.W., & Mikeal, R.L., (2014). Comparison of methods for detecting medication errors in 36 hospitals and skilled-nursing facilities. American Journal of Health-System Pharmacy, 59(5), 436–446. Retrieved from
- 4. http://library.neit.edu:2084/login.aspx?direct=true&db=ccm&A N=106538546&site=ehost -live #3 Medical errors are a result of a few different causes. We have learned in this week’s reading that these can be caused by technical errors, organizational errors and human errors. Technical errors are caused by an error in the computer system or a malfunction in equipment being used. Organizational error is when an intervention is not thoroughly planned, or not planned at all. It can also be caused by poor communication within the treatment team. Human errors occur when a person carries out an intervention without double checking if it is appropriate for the patient or if they are even using the proper intervention. It is vital to catch the medical error before or as soon as it happens, so that the steps can be taken to avoid adverse effects from occurring, or if they already have, from getting worse. In a 2015 study, a design was produced to report medical errors through an online system. Once the medical error is reported, the online system identifies the cause and the damage resulting from the medical error. It is completely anonymous so healthcare
- 5. providers do not have to be hesitant to use the system. After identifying the cause and damage of the medical error, the system provides feedback. The system recommends ways to prevent the error from reoccurring as well as providing guidelines on how to prevent them (Jeddi & Atoof, 2015). This will be a great asset if introduced in all medical facilities. Reference Jeddi, F. R., & Atoof, F. (2015). Improving patients’ care through electronic medical error reporting system. Health, Spirituality & Medical Ethics Journal, 2(2), 22–29. Retrieved from http://library.neit.edu:2084/login.aspx?direct=true&db=ccm&A N=108335172&site=ehost -live #4 When a person hears that a medical error has occurred, they automatically think of the worst case scenario. They are concerned for the patient’s safety and they begin to think of the quality of healthcare of the facility that they chose. Between 1985 and 2005, over 21,000 medical errors were reported in the United States and 3% of them were pediatric cases. In a 2018 study, the target participants were parents with children between the ages 3 to 6. The objective was to determine how parents felt
- 6. about medical errors and if they have every experienced one when it came to their child. More than half of those surveyed stated that the medical errors were caused by physicians. 21% reported that nurses made the medical error, 6% stated it was both the physicians and the nurses, and 21% blamed other members of the healthcare team. As far as the source of the issues, participants reported that they were related to a shortage of nurses, exhaustion from working long hours, physicians not making enough time for their patients, and lack of teamwork and communication. More than half of the parents involved in the study believed that they were also responsible for the errors that occurred. They believe they should be aware of what is going on so that they can identify if something is going wrong (Bektas & Yardimci, 2018). Involvement of patients and their friends or family in medical treatment is helpful in preventing medical errors. Reference Bektas, I., & Yardimci, F. (2018). What do parents think of medical errors? International Journal of Caring Sciences, 379–385. Retrieved from http://library.neit.edu:2084/login.aspx?direct=true&db=ccm&A N=129399275&site=ehost -live
- 7. #5 Medical errors have been ranked third on the Center for Disease Control’s (CDC) list of common causes of death, following heart disease and cancer. Patient safety is always the ultimate goal but it can also be a major challenge for healthcare systems across the world. One factor that has been found to contribute to these errors are poor communications systems. Electronic medical records (EMR) were developed to make it easier for healthcare providers to communicate, but they have not been perfected to solve these communication issues. It is believed that better data collection systems would help to measure each problem contributing to medical errors so that data can be collected in order to detect a pattern. In a 2014 study, data was collected from eleven countries, regarding patient-reported medical errors. However, it is important to keep in mind that many patients suffer from adverse effects after they are already discharged so it is hard to include them in the data. Many patients see more than one physician in different facilities so the risks of medical errors increase because not all specialists communicate effectively regarding their patient’s plan of care (Schwappach, 2014) . Patients along with their family members, or whoever else accompanies them to their appointments, are the only ones actually present during every appointment, treatment and consultation, etcetera. It is not
- 8. always guaranteed that they can remember everything that they are told or that goes on within an appointment. Better communication techniques should be placed so that each healthcare provider a patient sees is on the same page. Reference Schwappach, D. L. B. (2014). Risk factors for patient-reported medical errors in eleven countries. Health Expectations, 17(3), 321–331. https://library.neit.edu:2404/10.1111/j.1369-7625.2011.00755.x Risk factors for patient-reported medical errors in eleven countries David L. B. Schwappach MPH PhD*� *Scientific Head, Swiss Patient Safety Foundation, Zuerich, Switzerland and �Institute of Social and Preventive Medicine (ISPM), Senior lecturer, University of Bern, Bern, Switzerland Correspondence David L. B. Schwappach MPH, PhD Swiss Patient Safety Foundation Asylstr. 77, 8032 Zuerich Switzerland
- 9. E-mail: [email protected] patientensicherheit.ch Accepted for publication 12 October 2011 Keywords: medical errors, patient-reported outcomes, safety, survey Abstract Objectives The aim of this study was to identify common risk factors for patient-reported medical errors across countries. In country-level analyses, differences in risks associated with error between health care systems were investigated. The joint effects of risks on error-reporting probability were modelled for hypothetical patients with different health care utilization patterns. Design Data from the Commonwealth Fund�s 2010 lnternational Survey of the General Public�s Views of their Health Care System�s Performance in 11 Countries. Setting Representative population samples of 11 countries were
- 10. surveyed (total sample = 19 738 adults). Utilization of health care, coordination of care problems and reported errors were assessed. Regression analyses were conducted to identify risk factors for patients� reports of medical, medication and laboratory errors across countries and in country-specific models. Results Error was reported by 11.2% of patients but with marked differences between countries (range: 5.4–17.0%). Poor coordination of care was reported by 27.3%. The risk of patient-reported error was determined mainly by health care utilization: Emergency care (OR = 1.7, P < 0.001), hospitalization (OR = 1.6, P < 0.001) and the number of providers involved (OR three doctors = 2.0, P < 0.001) are important predictors. Poor care coordination is the single most important risk factor for reporting error (OR = 3.9, P < 0.001). Country-specific models yielded common and country-
- 11. specific predictors for self-reported error. For high utilizers of care, the probability that errors are reported rises up to P = 0.68. Conclusions Safety remains a global challenge affecting many patients throughout the world. Large variability exists in the frequency of patient-reported error across countries. To learn from others� errors is not only essential within countries but may also prove a promising strategy internationally. doi: 10.1111/j.1369-7625.2011.00755.x � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 321 Introduction Patient safety remains a major challenge for health care systems worldwide. 1 A recent chart review study conducted in the Netherlands reports the incidence of one or more adverse
- 12. events as 5.7% of all hospital admissions of which 40% were deemed preventable. 2 In Swe- den, the incidence of adverse events was 12.3% of hospital admissions with 70% being judged as preventable. 3 Similar data have been reported for several countries recently, including the United States, New Zealand, Canada and oth- ers. 4–7 On the basis of these studies, it can be concluded that approximately one of thousand hospital patients dies as a result from prevent- able adverse events. Many patients suffer from adverse events after discharge and are therefore not identified in record-based studies. 8 Less research has been conducted in the out-
- 13. patient care setting but the available studies suggest that patients are at considerable risk as well. In particular, preventable adverse drug events are frequent among patients in outpatient care. 9,10 Gurwitz et al. 11 report an overall rate of adverse drug events among older patients in the ambulatory setting of 50.1 ⁄ 1000 person-years, of which 28% were considered preventable. Studies based on staff members� incident reports in the United Kingdom yielded an error report rate of 75 ⁄ 1000 patient contacts in outpatient care. 12 In a similar study in the United States, errors and preventable adverse events were reported after 24% of outpatient visits. 13 In
- 14. Australia, the incidence of error reported to an anonymous reporting system by general practi- tioners was 0.24% per patient seen per year. 14 These setting-specific studies are valuable and important to identify and understand specific threats, e.g. hospital care or outpatient drug therapy. However, the frequency and harm of error is then investigated in isolation for specific health care sectors, settings or even therapies or treatments (e.g. medical errors in in-patient cancer treatment). But many patients utilize several types of health care in different settings, and the associated risks accumulate or even exponentiate because of coordination and com- munication failures among different providers. To assess patients� total risk, longitudinal observation of patient cohorts would be possible in theory but is methodologically challenging
- 15. and has not yet been undertaken to the author�s knowledge. Another methodological approach to the accumulated likelihood of error is the survey of citizens or patients. As patients are the only individuals physically present during every treatment and consultation, they carry with them important contextualized information in particular with relation to transition between different settings. 15,16 Surveying patients about their experience of medical error across specific types of health care consumed, e.g. hospital care, can help to identify risk factors for error along the care continuum and relative to specific patient-level factors and the amount and type of health care utilized. In addition, such patient surveys of error experience conducted in a multinational design
- 16. can inform health policy about common risk factors across countries and those specific to different health care systems. For example, some countries may perform better in ensuring safe transition and coordination of inpatient and outpatient care than others. The main aim of this analysis was the identification of risk factors for patient-reported medical errors across sev- eral countries. Country-level analyses were conducted to investigate differences in risks associated with error between different health care systems. To evaluate the joint effects of the identified risk factors, the probability that hypothetical patients with different personal and health-related profiles and health care utilization patterns would report error in their care was modelled. Methods
- 17. Design This analysis is based on data from �The Com- monwealth Fund�s 2010 lnternational Survey of the General Public�s Views of their Health Care System�s Performance in 11 Countries�, which was conducted in Australia, Canada, France, Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 322 Germany, the Netherlands, New Zealand, Nor- way, Sweden, Switzerland, the United Kingdom and the United States in 2010 [details are avail- able at http://www.commonwealthfund.org/ Content/Surveys/2010/Nov/2010-International- Survey.aspx]. Computer-assisted telephone interviews were conducted with nationally rep- resentative samples of adults aged 18 and above in each of these countries. Samples were drawn
- 18. from residential phone number lists, random number lists or random digit dialing. National samples differ in the extent to which cell lines were included. The interviewee in each house- hold was selected at random based on the most recent birthday in most countries. All sample records were called eight times or more before being abandoned as unusable. The interviews were conducted by professional interviewing staff and took on average 18–21 min across countries. Response rates varied from 13% in Norway to 54% in Switzerland. Survey The Commonwealth Fund�s 2010 lnternational Survey assessed public confidence in the health care system including access to care, cost and quality of care. Methods and results of earlier versions of the survey have been published pre- viously.
- 19. 17–19 For the purpose of this analysis, the following items relating to medical error experience are of particular relevance: whether respondents were ever been given the wrong medication or wrong dose by a doctor, nurse, hospital or pharmacist in the past 2 years (referred to as �medication error� hereinafter); whether there was a time in the past 2 years the responder thought a medical mistake was made in her treatment or care (referred to as �medical error� hereinafter); whether the responder has been given incorrect results for a diagnostic or laboratory test in the past 2 years (referred to as �lab error� hereinafter). The response categories were yes, no, not sure and decline to answer. Participants that reported any of the above errors were also asked whether the error occurred while they were hospitalized (yes, in the hospital, no, not sure, decline to answer). Participants were also asked several questions
- 20. related to demographics, their health and utili- zation of health care services. Responses to three items that asked for experience of poor coordi- nation of care in the past 2 years were also included in the analysis: whether subjects reported (i) test results or medical records were unavailable at the time of a scheduled appoint- ment; (ii) receiving conflicting information from different providers; (iii) doctors ordered medical tests that had already been performed. Data analysis Raw survey data were weighted for age, sex, education and region according to the most recent national census to reflect demographic distributions. To dichotomize data for analysis, �not sure� and �decline to answer� responses were recoded to missing. An aggregate measure was computed that
- 21. captures experience of any of the specific error items. We report descriptive analysis for all individual error items and the aggregate measure per country. To identify potential predictors, several demographic, health-related and heath care utilization variables were tested for their individual association with error experience in bivariate analyses: age, gender, education, income (relative to national averages), general health status, presence of chronic conditions (out of a specified list of conditions), having a regular doctor, number of doctors seen in the past 12 months, specialist care in the past 2 years, elective surgery in the past 2 years, hospital stay in the past 2 years, emergency care use in the past 2 years, medical tests (laboratory, X-ray, etc.) in the past 2 years and current reg- ular use of prescription drugs. Responses to
- 22. three coordination of care items were used to compute an indicator variable indicating expe- rience of none vs. any of these three events. All individual variables that were significantly associated with error experience in bivariate analyses at the 0.1 level were entered into the logistic regression model. Logistic regression was conducted for the aggregate measure, i.e. report of �any error�, and for each of the Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 323 individual error items as dependent variables. Multicollinearity of the predictor variables was assessed using the variance inflation factor (VIF). VIFs > 10 were inspected, and multi-
- 23. collinear variables were omitted from the mod- els. Model fit was assessed using the Archer– Lemeshow goodness-of-fit statistic, a F-adjusted mean residual goodness-of-fit test under com- plex sampling. 20 To evaluate the joint effects of the identified risk factors across all countries, we predicted the probability that hypothetical sub- jects (patients A–F) with different personal and health-related profiles and health care utilization patterns would report any error in their care. We also conducted country-specific analyses for three countries (United States, United Kingdom and Germany) that represent prototypes of health care system organization, i.e. market- driven, public and social insurance-based health care systems. Country-specific analyses were conducted using logistic hierarchical backward
- 24. selection with the aggregate measure as outcome variable. This approach was selected because of the limited size of the country-specific samples. Hierarchical stepwise regression differs to com- mon stepwise regression in that potential pre- dictors are grouped and ordered based on theory. The sequence in which groups are tested is not arbitrary. Guided by theoretical consid- erations, predictors were tested in the following blocks and sequences for each of the three country-specific models: (gender) (age) (income, education) (poor health, number of chronic conditions) (specialist care, number of doctors seen) (number of prescriptions drugs) (emer- gency care) (surgery, hospital) (coordination of care). Beginning with the first grouping (i.e. gender), the effect of each block was tested backwards and the entire block discarded if non-
- 25. significant. Significant blocks were included as a whole. Data were analysed using the software package STATASTATA v11.2. 21 Results Interviews were completed with 19 738 adults aged 18 and above. Sample characteristics are provided in Table 1. Self-reported error in health care was common in all countries but with marked differences even within European countries (Table 2). For example, only 2.2% of responders in the United Kingdom but 8.6% of French participants reported a medication error in the past 2 years. Overall, one of ten citizens self-reported a medical or medication error during the last 2 years. 18.8% of responders across countries reported that the last error in their care occurred in hospital, but this fraction
- 26. varied considerably between countries and ranged from 12.3% in Sweden to 31.3% in Switzerland (P < 0.001). Across countries, the Table 1 Sample characteristics, weighted data (n = 19 738) Characteristic n (%) of participants Country Australia 3552 (18.0) Canada 3302 (16.7) France 1402 (7.1) Germany 1005 (5.1) Netherlands 1001 (5.1) Norway 1058 (5.4) New Zealand 1000 (5.1) Sweden 2100 (10.6) Switzerland 1306 (6.6) United Kingdom 1511 (7.7) United States 2501 (12.7) Female gender 11 537 (51.5)
- 27. Age, mean 48.4 years 18–29 years 2212 (17.6) 30–49 years 6467 (36.9) 50–64 years 5632 (24.6) 65 years and above 5427 (20.9) Education (recoded from nation-specific response codes) High school or less 9984 (58.4) Some college 4266 (21.4) College graduate or higher 5150 (20.3) Income (relative to national averages) Much below average 3275 (17.1) Somewhat below average 3412 (18.9) Average 4854 (26.9) Somewhat above average 4441 (24.6) Much above average 2365 (12.5) Self-rated health Excellent ⁄ very good 10 522 (53.9) Good 6262 (31.5) Fair ⁄ poor 2876 (14.6)
- 28. Chronic conditions None 7429 (42.0) 1 condition 5137 (26.0) 2 or more conditions 7119 (32.0) Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 324 fraction of respondents that reported experience of two different types of error was 2.5%, and 0.5% reported all three types of errors. Poor coordination of care was also common in all countries: 10.9% reported that test results or medical records were not available, 19.6% per- ceived to have received conflicting information by care providers and 10.5% reported that tests were ordered although they had been performed
- 29. before. A quarter of citizens (27.3%) reported any of these coordination problems in the past 2 years. A number of variables were associated with patient-reported error in bivariate analysis (Fig. 1). Across all countries, health status and health care utilization variables were associated with all three types of self-reported errors (and the aggregate measure) with different levels of strength. Associations between demographic variables and errors were less systematic: Higher age was inversely related to all types of reported errors, except medication errors. Female gender was associated with medical error, medication error and the aggregate measure, but not the Table 2 Frequency of self-reported errors by country, weighted data Country Medical error
- 30. n (%) Medication error n (%) Either medical or medication error n (%) Laboratory error* n (%) Either medical, medication or laboratory error (aggregate measure) n (%) Australia 282 (8.3) 155 (4.5) 350 (10.1) 69 (2.4) 395 (11.4) Canada 212 (7.7) 179 (6.0) 322 (10.9) 106 (4.1) 372 (12.2) France 87 (5.9) 110 (8.6) 157 (11.6) 39 (2.8) 178 (12.5) Germany 54 (5.9) 20 (2.2) 64 (7.0) 12 (1.7) 73 (7.8) Netherlands 52 (4.8) 45 (4.5) 82 (7.8) 25 (3.0) 97 (9.3)
- 31. Norway 101 (10.8) 79 (8.1) 147 (15.7) 29 (3.4) 161 (17.0) New Zealand 59 (5.6) 39 (4.6) 82 (8.3) 19 (2.4) 92 (9.0) Sweden 118 (6.1) 92 (4.9) 173 (8.9) 26 (1.9) 184 (9.5) Switzerland 81 (8.0) 61 (5.3) 123 (11.4) 31 (3.2) 136 (11.9) United Kingdom 39 (3.2) 25 (2.2) 55 (4.7) 21 (2.6) 66 (5.4) United States 204 (9.7) 150 (6.4) 295 (12.9) 83 (5.0) 331 (14.3) *Based on those that reported blood test, X-rays or other tests in the past 2 years. *** ** *** *** *** *** *** *** *** ***
- 32. *** *** *** *** *** Age > 65 years Female gender Education, high school or less Income much below average Poor self−rated health 1 chronic cond. 2 or more chronic cond. Regular doctor Specialist care 1−2 doctors 3 or more doctors Elective surgery Inpatient stay Emergency care 1 prescription drug 2 or more prescription drugs Poor care coordination 0 1 2 3 4 5 6 7 8
- 33. Odds ratio Figure 1 Bivariate (unadjusted) asso- ciations between demographic, health and health care utilization variables and experience of any error (aggregate measure), weighted data. Stars indi- cate significant associations (*P < 0.05; **P < 0.01; ***P < 0.01). Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 325 subset of laboratory errors. Low income was associated with all types of reported errors, again except laboratory errors. Education was only weakly associated with reporting medical
- 34. error. Results of the regression model for all 11 countries and three country-specific models are presented in Table 3. All VIFs were <2.0 indi- cating no substantial multicollinearity. The Archer–Lemeshow goodness-of-fit statistic did not indicate any overall model departure from the observed data. Across countries, the risk of patient-reported error is determined mainly by health care utilization. Emergency care, hospi- talization and the number of providers involved are among the most important predictors. Having seen three or more doctors doubles the risk for reporting any error when other factors are controlled for, e.g. health status and use of prescription drugs. Experience of poor care coordination is the single most important risk factor, associated with a four-fold increase in
- 35. reporting error. Responders with chronic con- ditions and poor health are at considerably higher risk for reporting errors in their care, even after adjusting for a large variety of health care utilization. After controlling for health and health care utilization, patients younger than 65 years were nearly twice as likely to report any medical error. The joint influence of the risk factors on the probability that patients report error in their care is substantial (illustrated in Fig. 2). For example, the differences between hypothetical patients B and F (chronic conditions, emergency care, prescription drugs, number of doctors seen, specialist care and coordination of care prob- lems) account for a 14-fold increase in proba- bility of reporting error, keeping younger age, low income, poor self-reported health, hospital
- 36. stay and surgery constant (pB = 0.049, pF = 0.679, P < 0.001). Three country-specific models yield common and country-specific predictors for self-reported error. Poor coordination of care experiences was the strongest predictor for patient-reported error in all three countries. Hospital care in the past 2 years was associated with reporting error in the United Kingdom and Germany, but not in the United States. On the contrary, poor health, specialist care and emergency care increase the likelihood of self-reported error in the United States, but not in the United Kingdom and Germany. Use of prescription drugs was a sig- nificant predictor only in the United Kingdom. Having a much below average income was a strong predictor for reporting error experience in Germany.
- 37. Discussion This study reports new data on patients� per- ceptions of error in 11 countries and identified a number of important risk factors. Overall, one of ten surveyed patients reported either medical, medication or laboratory errors in their care but this risk varies markedly by a factor of 3 across countries (5.4% in the United Kingdom and 17.0% in Norway). Several factors may help to explain this finding: Different health care sys- tems may in fact perform better in preventing errors and can thus deem to be safer. However, observed differences between countries may also stem from differences in patients� likelihood to identify and report error, rather than differences in true incidences. While evidence shows that patients� reports of adverse events are often in well concordance with other detection methods, e.g. record review, it is unclear whether this degree of concordance is similar across coun-
- 38. tries. 22–25 For example, safety in health care may be an issue of high public awareness in some countries and largely unrecognized in others. As a result, patients may be more or less vigilant and educated about safety and have different abilities or motivation to detect errors. �Medical error� may also be defined differently in diverse cultural contexts. In addition, patients� reports of errors are likely to be affected by official standards and cultural norms among health care workers on how openly to communicate errors towards patients. Thus, patients� reports of error do not only reflect incidence of error but are also �contaminated� by identification and reporting biases. Reporting effects rather than differences in frequency may also help to explain why Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331
- 88. .9 9 7 Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 327 younger patients were systematically more likely to report errors compared to respondents aged 65 and above, a finding that has been reported in the previous studies. For example, in a recent survey study among Swiss hospital patients, the likelihood for reporting adverse events during hospital stay decreased significantly with higher age by a comparable magnitude. 26 Younger patients may be more aware of safety problems
- 89. and less reluctant to report these. Across 11 countries, our data clearly show that risk of self-reported error increases steadily with the amount and categories of health care consumed. However, across countries, patients with poor health and low income are at increased risk even after adjusting for various health care utilization-related variables. It is not surprising that poor care coordination experi- ence is the most important single risk factor for reporting errors across countries and in our country-specific analyses. Unavailable records, conflicting information and repetition of tests can signal, cause or coincide with safety events and can themselves be regarded as �error�, even if they may not cause harm. Thus, it seems likely that an unknown fraction of responders had the same event in mind when reporting coordination of care problems and error. This would lead to
- 90. an overestimation of the association of coordi- nation of care problems with error. Indeed, Rathert et al. 27 recently reported from a quali- tative study that patients seem to share a broader interpretation of safety compared with health professionals and often include commu- nication and coordination failures. Our country- level analyses reveal that the risk associated with different health care services varies considerably between countries. This strengthens the assumption that systems differ in their abilities to manage specific threats for patient safety. This view is also supported by the large variance observed in reported occurrence of error. Hos- pital-associated error was much more frequent in some countries (e.g. Switzerland) compared to
- 91. the cross-national average. These results may reflect differences between countries in how care is organized. For example, access to specialist outpatient care is far more restrictive in some countries compared to others. While our results clearly indicate that various types of health care consumed increase the risk of error, the relative magnitude of predictor variables should be compared with care. As with all surveys, health care utilization had to be operationalized for measurement and this oper- ationalization may interact with specific forms of care organizations and is thus important for interpretation: For example, a single hospital stay is longer and patients are exposed to risk (and error identification) simply for a longer 0 .0 0
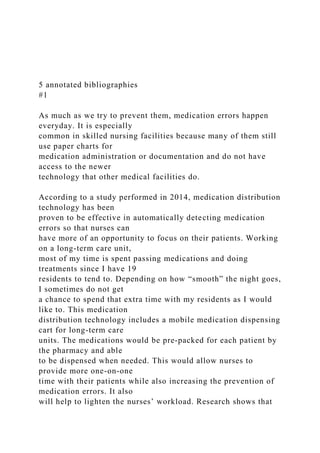
- 93. p o rt e d e rr o r A B C D E F Hypothetical patients Figure 2 Predicted probability for patient-reported error (aggregate measure) across 11 countries for six hypothetical patients (A–F), weighted data. Six hypothetical patients (A–F) were modelled with the following characteristics: Patient A: Aged >65 years, average income, good self-reported health, two or more chronic conditions, emergency care, no hospital or surgery, two or more prescription drugs, one or two doctors, no specialist, no coordination of care problems. Patient B: Aged <65 years, much below average income,
- 94. poor self-reported health, no chronic conditions, no emer- gency care, hospital stay and surgery, no prescription drugs, no doctors seen, no specialist, no coordination of care problems. Patient C: Aged <65 years, average income, poor self-reported health, one chronic condition, no emergency care, hospital stay, no surgery, one prescription drug, one or two doctors, specialist, no coordination of care problems. Patient D: Aged >65 years, much below average income, poor self-reported health, no chronic conditions, emergency care, hospital stay and surgery, no prescription drugs, one or two doctors, no specialist, poor coordination of care. Patient E: Aged <65 years, average income, good self-reported health, one chronic condition, no emergency care, no hospital stay or surgery, two or more prescription drugs, three or more doctors, specialist, poor coordination of care. Patient F: Aged <65 years, much below average income, poor self- reported health, two or more chronic conditions, emergency care, hospital stay and surgery, two or more prescription
- 95. drugs, three or more doctors, specialist, poor coordination of care. Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 328 duration as compared to a short outpatient consultation. The number of doctors seen does reflect the increasing need for coordination, but not necessarily treatment intensity. Thus, for countries that restrict access to the number of providers involved, treatment intensity per pro- vider may be more important. This study has some limitations: First, the samples for each of 11 countries have been drawn and weighted to be representative for each individual country.
- 96. The sample sizes did not allow more extensive analyses of country-level data, e.g. selection of predictors based on bivariate analyses or including the same predictors in all country- specific models irrespective of their significance. In addition, the reasons for and potential effects of the very different survey response rates remain unclear. For example, Norway had the lowest response rate (13%) and the highest fraction of patients that reported any error in their care (17%). It seems likely that individuals that experienced error were more likely to par- ticipate than others. Second, we used an aggre- gate measure of error as outcome variable in regression analyses. Distinct associations with specific types of errors, i.e. medication or labo- ratory errors, may thus have gone undetected. Finally, owing to the nature of the data, we
- 97. cannot demonstrate causal or temporal rela- tionship between health care utilization and error. While responders were asked to consider the past 2 years in most of the questions, we do not know whether health care was utilized before or after the reported events occurred and how they are connected. Despite these limitations, the results of this study are alarming. Our modelling of hypo- thetical patients shows that for high utilizers of health care that unify multiple risk factors it is nearly rule rather than exception that errors occur. Patients who utilize various types of health care in different settings accumulate a high risk of errors, which is largely underesti- mated in isolated setting-specific adverse event studies. Despite the associated health-related harm, the common experience of error in these
- 98. populations may also cause considerable loss of trust in the health care system as a whole. Medical error is communized with poor coor- dination of care experiences, and obviously, health care systems fail to overcome risks asso- ciated with the segmentation of health care. This is also indicated by the fact that having a regular doctor had no substantial protecting effects on patient safety. These results emphasize that patient safety remains a global challenge affect- ing many patients throughout the world. How- ever, large variability exists in the frequency of patient-reported error across countries. Taking the opportunity to learn from others� errors is not only essential within individual institutions or systems but may also prove a promising strategy internationally. Ethics approval Ethics approval was not necessary for this study.
- 99. Acknowledgements The author thanks the Commonwealth Fund for permission to analyse the data. The support by Markus Weber (Swiss Federal Office of Public Health, BAG) is highly appreciated. Three anonymous referees are acknowledged for their thorough comments on an earlier draft. The contents are the sole responsibility of the author and do not represent the views of the Com- monwealth Fund or local agencies of the par- ticipating countries. Competing interests None. Funding The author obtained no funding for this partic- ular research. Core funding for the �Common- wealth Fund�s 2010 lnternational Survey of the General Public�s Views of their Health Care System�s Performance in Eleven Countries� was by the Commonwealth Fund with co-funding
- 100. from the following organizations: the Australian Commission on Safety and Quality in Health Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 329 Care; the Ontario Health Quality Council; the Health Council of Canada; the Quebec Health Commission; La Haute Autorité de Santé; the Caisse Nationale d�Assurance Maladie Ces Travailleurs Salaries; the German lnstitute for Quality and Efficiency in Health Care; the Dutch Ministry of Health, Welfare and Sport; the Sci- entific lnstitute for Quality of Healthcare, Rad- boud University Nijmegen; the Norwegian Knowledge Centre for the Health Services; the Health Foundation; the Swedish Ministry of
- 101. Health and Social Affairs; the Swiss Federal Office of Public Health. References 1 von Laue NC, Schwappach DL, Koeck CM. The epidemiology of medical errors: a review of the liter- ature. Wiener Klinische Wochenschrift, 2003; 115: 318–325. 2 Zegers M, de Bruijne MC, Wagner C et al. Adverse events and potentially preventable deaths in Dutch hospitals: results of a retrospective patient record re- view study. Quality and Safety in Health Care, 2009; 18: 297–302. 3 Soop M, Fryksmark U, Koster M, Haglund B. The incidence of adverse events in Swedish hospitals: a retrospective medical record review study. Interna- tional Journal for Quality in Health Care, 2009; 21: 285–291. 4 Baker GR, Norton PG, Flintoft V et al. The Cana-
- 102. dian Adverse Events Study: the incidence of adverse events among hospital patients in Canada. CMAJ, 2004; 170: 1678–1686. 5 Davis P, Lay-Yee R, Briant R, Ali W, Scott A, Schug S. Adverse events in New Zealand public hospitals 1: occurrence and impact. New Zealand Medical Jour- nal, 2002; 115: U271. 6 Thomas EJ, Studdert DM, Burstin HR et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Medical Care, 2000; 38: 261–271. 7 Vincent C, Neale G, Woloshynowych M. Adverse events in British hospitals: preliminary retrospective record review. BMJ, 2001; 322: 517–519. 8 Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Annals of Internal Medicine, 2003; 138: 161–167. 9 Thomsen LA, Winterstein AG, Sondergaard B,
- 103. Haugbolle LS, Melander A. Systematic review of the incidence and characteristics of preventable adverse drug events in ambulatory care. Annals of Pharma- cotherapy, 2007; 41: 1411–1426. 10 Miller GC, Britth HC, Valenti L. Adverse drug events in general practice patients in Australia. Medical Journal of Australia, 2006; 184: 321–324. 11 Gurwitz JH, Field TS, Harrold LR et al. Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA, 2003; 289: 1107–1116. 12 Rubin G, George A, Chinn DJ, Richardson C. Errors in general practice: development of an error classifi- cation and pilot study of a method for detecting errors. Quality and Safety in Health Care, 2003; 12: 443–447. 13 Elder NC, Meulen MV, Cassedy A. The identification of medical errors by family physicians during outpa-
- 104. tient visits. Annals of Family Medicine, 2004; 2: 125– 129. 14 Makeham MA, Kidd MR, Saltman DC et al. The threats to australian patient safety (TAPS) study: incidence of reported errors in general practice. Medical Journal of Australia, 2006; 185: 95–98. 15 Unruh KT, Pratt W. Patients as actors: the patient�s role in detecting, preventing, and recovering from medical errors. International Journal of Medical Informatics, 2007; 76 (Suppl 1): S236–S244. 16 Schwappach DL. Engaging patients as vigilant part- ners in safety: a systematic review. Medical Care Research and Review, 2010; 67: 119–148. 17 Schoen C, Osborn R, Huynh PT et al. Taking the pulse of health care systems: experiences of patients with health problems in six countries. Health Affairs 2005;Suppl Web Exclusives(W5):509–525. 18 Schoen C, Osborn R, How SKH, Doty MM, Peugh J. In chronic condition: experiences of patients with
- 105. complex health care needs, in eight countries, 2008. Health Affairs, 2009; 28: w1–w16. 19 Scobie A. Self-reported medical, medication and laboratory error in eight countries: risk factors for chronically ill adults. International Journal for Quality in Health Care, 2011; 23: 182–186. 20 Archer KJ, Lemeshow S, Hosmer DW. Goodness-of- fit tests for logistic regression models when data are collected using a complex sampling design. Compu- tational Statistics and Data Analysis, 2007; 51: 4450– 4464. 21 StataCorp. Stata Statistical Software: Release 11.2. College Station, TX: Stata Corporation, 2010. 22 Fowler FJ, Epstein A, Weingart SN et al. Adverse events during hospitalization: results of a patient survey. Joint Commission Journal on Quality and Safety, 2008; 34: 583–590. 23 Weingart SN, Pagovich O, Sands DZ et al. What can
- 106. hospitalized patients tell us about adverse events? Learning from patient-reported incidents. Journal of General Internal Medicine, 2005; 20: 830–836. 24 King A, Daniels J, Lim J, Cochrane DD, Taylor A, Ansermino JM. Time to listen: a review of methods Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 330 to solicit patient reports of adverse events. Quality and Safety in Health Care, 2010; 19: 148–157. 25 Massó Guijarro P, Aranaz Andres JM, Mira JJ, Perdiguero E, Aibar C. Adverse events in hospitals: the patient�s point of view. Quality and Safety in Health Care, 2010; 19: 144–147. 26 Schwappach DLB, Frank O, Hochreutener MA. �New perspectives on well-known issues�: Patients�
- 107. experiences and perceptions of safety in Swiss hospitals. Zeitschrift für Evidenz, Fortbildung und Qualität im Gesundheitswesen, 2011; 105: 542–548. 27 Rathert C, Brandt J, Williams ES. Putting the ‘‘patient’’ in patient safety: a qualitative study of consumer experiences. Health Expectations 2011; doi: 10.1111/j.1369-7625.2011.00685.x. Risk factors for patient-reported medical errors, D L B Schwappach � 2012 John Wiley & Sons Ltd Health Expectations, 17, pp.321–331 331 Copyright of Health Expectations is the property of Wiley- Blackwell and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. International Journal of Caring Sciences
- 108. January-April 2018 Volume 11 | Issue 1| Page 379 www.internationaljournalofcaringsciences.org Original Article What Do Parents Think of Medical Errors? Ilknur Bektas Dokuz Eylul University, Faculty of Nursing, Department of Pediatric Nursing , Izmir, Turkey Figen Yardimci Ege University, Faculty of Nursing, Department of Pediatric Nursing, Izmir, Turkey Correspondence: Ilknur Bektas, Dokuz Eylul University, Faculty of Nursing, Department of Pediatric Nursing, Inciralti, Izmir, Turkey E-mail: [email protected] Abstract Background: In its reports on “medical errors” and “patient safety and health care quality”, the Institute of Medicine dealt with two significant problems in health care environments. Objective or Aims: The purpose of study is to identify the views of parents with children aged three to six years old concerning medical errors. Methodology: The sample was comprised of 301 parents. 9.3% of parent encountered a medical error. The data for the study were collected through “the Descriptive Form for Parents” and “The Parents’ Perceptions of Medical Errors Form.” The scenarios for the study were
- 109. prepared in reference to the medical errors on which the Third Specialized Board of the Council of Forensic Science had expressed an opinion and to other scenarios whose validity had already been tested in other similar studies. Results: Case 1 was viewed as an example of a medical error by 91.7% of the parents. Out of these parents, 77.9% considered it as a severe/serious error. As for Case 2, 95% of the participants viewed it as an example of a medical error. Conclusions: Parents who considered a case as an example of a medical error were more likely to desire disclosure and reporting. Keywords: Medical errors; parents; perceptions. Introduction In its reports on “medical errors” and “patient safety and health care quality”, the Institute of Medicine dealt with two significant problems in health care environments. According to the reports, 98.000 people die of medical errors in the USA every year (IOM, 1999). It is essential to ensure patient safety in health care systems, which are becoming increasingly complicated and equipped with technological devices. Individuals are under greater threat in such health care systems. Accordingly, greater and greater importance is attached to patient safety (Cirpi et al., 2009; Gokdogan and Yorgun, 2010; Hakverdioglu Yont, 2011). The Physician Insurers Association reported that
- 110. there were 214226 reports of medical errors in the USA between 1985 and 2005, and 2.97% of these reports were pediatric cases (as cited in Carroll et al., 2006). The rate of medical errors among discharged children was discovered to range from 1.81% to 2.96% in the USA (Slomin, LaFleur, Ahmed and Joseph, 2003). In Turkey, a total of 1458 files were submitted to the High Council of Health between 2000 and 2006, and 378 of them (25%) were pediatric cases (Ozkaya, 2008). All these suggest that children constitute an important group to be taken into consideration in terms of medical errors and patient safety both in Turkey and other nations. Programs on patient safety in health care services often neglect the patient perspective. This is in sharp contrast to the fact that active roles of patients in health care services should be recognized and supported. The reason for this is that patients play a key role in achieving accurate diagnosis, deciding on the treatment, choosing a safe and experienced service provider, providing and monitoring accurate treatment, identifying negative occurrences, and taking necessary actions. The “To Err is Human” report by the International Journal of Caring Sciences January-April 2018 Volume 11 | Issue 1| Page 380 www.internationaljournalofcaringsciences.org Institute of Medicine (IOM, 1999) suggests that
- 111. patients should be acknowledged as active participants of medical care processes and a member of the health care team (IOM, 1999). The identification of parental views of medical errors will hopefully be useful for ensuring cooperation with patients, something that we have to do, and enabling patients, who are often neglected, to participate in the process. Methodology Population and sample The study was designed as a descriptive and cross-sectional one. The sample was comprised of 301 parents whose children attended four different kindergartens run by the District Directorate for National Education. Sample size was calculated according to pilot study. By the pilot study, the sample size needed was at least 84 student/parent for power analysis with a Type II error 0.20 and 0.01 level of significance. Instruments The data for the study were collected through “the Descriptive Form for Parents” and “The Parents’ Perceptions of Medical Errors Form.” The former was focused on identifying certain socio-demographics for the participants, namely age, occupation, social security, number of children, previous hospitalization record, and previous medical error record). The latter was composed in reference to the literature in order to reveal parents’ views of medical errors. The form contained two cases, which were followed by 14
- 112. questions. It was translated from English to Turkish by two language experts, and the Turkish version of the form was revised by the researchers. Before it was finalized, the Turkish version was submitted to a Turkish language expert. To make the form more reliable, the Turkish version was submitted to another language expert, who had never seen the form previously, to be translated again. The scenarios for the study were prepared in reference to the medical errors on which the Third Specialized Board of the Council of Forensic Science had expressed an opinion and to other scenarios whose validity had already been tested in other similar studies. The level of severity was not specified by the researchers; instead, the participants were presented with cases that might involve medical errors so as to identify whether they considered them as medical errors and how severe they thought they were. Expert judgment was received before the form that contained the cases and relevant questions was administered to the participants. The content validity of the form was assessed by eight experts. According to Lawshe’s table, minimum fit criterion is 0.78 for eight reviewers. The instrument had a content validity ratio (CVR) of 0.91, a value higher than the one specified in Lawshe’s table, which suggested that
- 113. there was advanced fit among the experts (Alpar, 2010; Sencan, 2005). Pilot Test The form was administered to 20 randomly chosen parents, who were from the schools included in the present study but not in its sample. Positive feedback by these parents suggested that the form could be administered to the sample. The Parents’ Perceptions of Medical Errors Form : The form contained two scenarios and 14 questions. The first three questions were as to whether the participants viewed the case as a medical error, how severe they thought the medical error was, and by whom they would like to be informed about the error. The remaining questions were grouped under three headings, namely disclosure, reporting, and legal actions. Each question could be answered by one of the three following options: I agree (3), neutral (2), and I disagree (1). Cronbach’s alpha values were 0.79 and 0.86 for the first and second scenarios respectively. Ethics The permission for the study was granted by the Scientific Ethics Committee. In addition, written consent was obtained from the Provincial Directorate for National Education while verbal consent was obtained from school principals and parents.
- 114. Statistical Analysis The data were analyzed through percentages, Mann-Whitney U test, Kruskal Wallis Analysis, Mann-Whitney U test with Bonferroni correction, independent samples t-test with Bonferroni correction, and Multiple Regression analysis. International Journal of Caring Sciences January-April 2018 Volume 11 | Issue 1| Page 381 www.internationaljournalofcaringsciences.org Results Slightly more than half of the participants (52.4%) reported that medical errors were mostly committed by physicians, 20.8% by nurses, 5.6% by both physicians and nurses, and 21.2% by other members of health care staff. As for the cause of the medical error, 9.7% of the participants noted that medical errors resulted from the inadequate number of nurses, 15.9% from exhaustion and stress caused by long working hours, 21.6% from communication disorders, 13.6% from lack of team work, 15.9% from the complicated nature of health care services, and 23.3% from the inability of physicians to allocate enough time to patients. More than a quarter of the participants (27.2%)
- 115. reported that parents should file a lawsuit against the member of the health care staff responsible for the medical error whereas 19.6% of them said that the health care institution should be taken to the court. Another 10% believed that other actions should be taken. Whereas 35.2% of the participants believed that those subject to the medical error should file a lawsuit against both the member of the health care staff and the health care institution, 2.3% of them noted that they should not only file a lawsuit against the member of the health care staff and the health care institution but also take other actions. As for what patients could do in terms of safety, 5.6% of the parents reported that patients could absolutely protect themselves against medical errors while 36.2% thought that they could slightly protect themselves against such errors. In addition, 17.9% of the participants believed that parents could protect themselves against medical errors. Whereas 31.9% of the participants reported that parents could not protect themselves against medical errors, 8.3% of them believed that parents could definitely not protect themselves. Twenty-nine percent of the parents reported that they much relied on their own knowledge and awareness to get protected from medical errors whereas 67.4% reported their slight reliance on their knowledge and awareness in this respect. On the other hand, 10.6% of them did not rely on their own knowledge and awareness to get protected against medical errors.
- 116. Findings on Case 1 Table 1. The Results of the Multiple Regression Analysis of the Variables in the Parents’ Viewing Case 1 as an Example of a Medical Error B Standard Error Standard Beta (β) t p Constant 0.963 0.384 2.509 0.017 Parental Role 0.294 0.093 0.575 3.178 0.003 Age 0.018 0.005 0.539 3.600 0.001 Educational Status 0.030 0.032 0.149 0.949 0.349 Occupational Status 0.135 0.072 0.323 1.863 0.071 Social Security 0.060 0.078 0.111 0.770 0.446 Number of Children 0.016 0.052 0.042 0.304 0.763 Length of Hospitalization for Child 0.032 0.038 0.140 0.852 0.400 Number of Times of Hospitalization
- 117. 0.013 0.042 0.050 0.318 0.753 Type of Hospital 0.003 0.037 0.014 0.092 0.927 Previous Medical Error Record 0.078 0.097 0.108 0.810 0.423 R=0.661 R2=0.437 F= 2.540 p= 0.017 DW Coefficient= 2.5 (1.5-2.5) International Journal of Caring Sciences January-April 2018 Volume 11 | Issue 1| Page 382 www.internationaljournalofcaringsciences.org While 91.7% of the participants viewed the scenario in Case 1 as an example of a medical error, the remaining 8.3% did not. Whereas the mean score of the former group in the desire for disclosure was 14.33 ± 1.17, the latter group had a mean score of 13.08 ± 3.26. The discrepancy between the former and latter groups in their mean scores was not statistically significant (p=0.079). As for the desire for reporting, the mean score of the former group was 5.91 ± 0.44 whereas the latter group had a mean score of 5.28 ± 1.48. The discrepancy between the former and latter groups in terms of their mean scores in the desire for reporting was statistically highly
- 118. significant (p=0.000). Regarding the desire for legal actions, the mean score of the former group was 12.70 ± 2.01whereas the latter group had a mean score of 10.12 ± 3.16. The discrepancy between the former and latter groups in terms of their mean scores in the desire for reporting was statistically highly significant (p=0.000). The results of the regression analysis indicated that the variables involved in the study were (R2=0.437) in an intermediately significant interaction with viewing Case 1 as an example of a medical error (F= 2.540, p= 0.017). These variables could account for only 43.7% of viewing Case 1 as an example of a medical error. According to the standardized regression coefficient (β), the independent variables had an influence on viewing Case 1 as an example of a medical error in the following order of importance: the parental role of the respondent (i.e. mother or father), the age of the respondent, the occupational status of the respondent, the educational status of the respondent, the length of hospitalization for the child, social security, previous medical error record for the parent, the number of times of hospitalization, the number of children, and the type of hospital. On the other hand, the results of the t-test demonstrated that the parental role of the respondent (i.e. mother or father) (p=0.003) and the age of the respondent (p=0.001) had a significant influence on viewing Case 1 as an example of a medical error. Table 2. The Results of the Multiple Regression Analysis of the
- 119. Variables in Parents’ Viewing Case 2 as an Example of a Medical Error B Standard Error Standard Beta (β) t p Constant 0.519 0.431 1.205 0.236 Parental Role (i.e. mother or father) 0.006 0.104 0.011 0.057 0.955 Age 0.003 0.006 0.088 0.524 0.604 Educational Status 0.042 0.035 0.210 1.193 0.241 Occupational Status 0.086 0.081 0.206 1.057 0.298 Social Security 0.038 0.088 0.069 0.429 0.671 Number of Children 0.046 0.058 0.122 0.789 0.435 Length of Hospitalization for Child 0.05 .043 0.231 1.253 0.218 Number of Times of Hospitalization
- 120. 0.051 0.047 0.192 1.085 0.285 Type of Hospital 0.058 0.041 0.243 1.421 0.164 Previous Medical Error Record 0.014 0.109 0.020 0.131 0.896 R=0.539 R2=0.29 F= 1.337 p= 0.245 DW Coefficient= 1.913 (1.5-2.5) Findings on Case 2 While 95% of the participants viewed the scenario in Case 2 as an example of a medical error, 3.7% did not. The remaining 1.3% left the question unanswered. Whereas the mean score of the former group in the desire for disclosure was 14.54 ± 1.08, the latter group had a mean score of 13.27 ± 3.03. The discrepancy between the former and latter groups in their mean scores was International Journal of Caring Sciences January-April 2018 Volume 11 | Issue 1| Page 383 www.internationaljournalofcaringsciences.org statistically significant (p=0.019). As for the desire for reporting, the mean score of the former group was 5.92 ± 0.49 whereas the latter group had a mean score of 5.36 ± 1.28. The
- 121. discrepancy between the former and latter groups in terms of their mean scores in the desire for reporting was statistically highly significant (p=0.000). As for the desire for legal actions, the mean score of the former group was 13.45 ± 1.82 whereas the latter group had a mean score of 12.00 ± 3.77. The discrepancy between the former and latter groups in terms of their mean scores in the desire for legal actions was not statistically significant (p=0.316). The results of the regression analysis indicated that the variables involved in the study were (R2=0.29) in a low and insignificant interaction with viewing Case 2 as an example of a medical error (F= 1.337, p= 0.245). These variables could account for only 29% of viewing Case 2 as an example of a medical error. According to the standardized regression coefficient (β), the independent variables had an influence on viewing Case 2 as an example of a medical error in the following order of importance: the type of hospital, the length of hospitalization for the child, the educational status of the respondent, the occupational status of the respondent, the number of times of hospitalization, the number of children, the age of the respondent, social security, previous medical error record for the parent, and the parental role of the respondent (i.e. mother or father). On the other hand, the results of the t-test demonstrated that none of the variables had a significant influence on viewing Case 2 as an example of a medical error. Discussion
- 122. In the present study, only a small percentage of the parents (9.3%) reported encountering medical errors in the clinic. When compared to other similar studies (Hobgood et al., 2005; Mazor et al., 2010; Matlow et al., 2010), the ratio is smaller, which might be attributed to the fact that the sample for the present study was from outside hospitals and that the parents stayed at hospitals for a relatively shorter time. According to the parents, medical errors were mostly committed by physicians (52.4%), nurses (20.8%), and other health care staff (21.2%) respectively. Ozkaya (2008) reported that nearly half of the files submitted to the Third Specialized Board of the Council of Forensic Science were about medical errors committed by physicians and that nurses were responsible for only 6.7% of these errors. The reason for the discrepancy might be that the public views physicians as the person with sole responsibility for treatment and nurses as only the implementer of commands given by physicians. The participants attributed medical errors to different causes, namely the inadequate number of nurses (9.7%), exhaustion and stress caused by long working hours (15.9%), communication disorders (21.6%), lack of team work (13.6%), the complicated nature of health care services (15.9%), and the inability of physicians to allocate enough time to patients (23.3%). The finding is quite similar to those of other similar studies (Hogbood et al., 2005; Mazor et al., 2010; and Matlow et al., 2010).
- 123. Almost all of the parents (96%) believed that parents/patients should be informed about and apologized for medical errors. Similarly, studies in the literature have revealed that parents are of the opinion that they should be informed about and apologized for medical errors (Hobgood et al., 2005; Mazor et al., 2010; Matlow et al., 2010). The great majority of the participants in the present study stressed that in case of medical errors parents should file a lawsuit against both the person committing the error and the institution, and they demanded that institutions should take legal actions. The finding is supported by the 10% increase in the number of lawsuits against nurses in recent years (Zincirci, 2010). More than half of the parents (56.5%) believed that parents were also responsible for preventing medical errors. A review of literature suggests parents think that parents, along with children, are also responsible for the prevention of medical errors (Hobgood et al., 2005; Mazor et al., 2010; Matlow et al., 2010). In the present study, 89.3% of the parents relied on their own knowledge and awareness to prevent medical errors. Similarly, Clarke et al. (2005) concluded from their study that parents believe they can prevent medical errors by being careful with the treatment of their children. Likewise, the IOM (2003) stresses that involvement of patients and their
- 124. friends/relatives in treatment and care is a significant step in the prevention of medical errors. International Journal of Caring Sciences January-April 2018 Volume 11 | Issue 1| Page 384 www.internationaljournalofcaringsciences.org Case 1 and Case 2 were considered as an example of a medical error by 91.7% and 95% of the participants respectively. Actually, both cases were an example of a medical error, though at different levels of severity, and almost all of the participants viewed the cases as an example of a medical error. The finding is similar to that of Hobgood et al. (2005), who observed that 99% of parents accurately viewed the scenarios they were presented with as examples of medical errors. The finding of the present study suggests that parents are knowledgeable about medical errors, though at varying degrees; therefore, a significant decrease is likely to be achieved in the number of medical errors if parents are informed about and enabled to participate in the treatment and care of their children, as recommended by the IOM (2003). The results of the regression analysis indicated that the variables involved in the study were (R2=0.437) in an intermediately significant interaction with viewing Case 1 as an example of a medical error (F= 2.540, p= 0.017). These variables could account for only 43.7% of
- 125. viewing Case 1 as an example of a medical error. According to the standardized regression coefficient (β), the independent variables had an influence on viewing Case 1 as an example of a medical error in the following order of importance: the parental role of the respondent (i.e. mother or father), the age of the respondent, the occupational status of the respondent, the educational status of the respondent, the length of hospitalization for the child, social security, previous medical error record for the parent, the number of times of hospitalization, the number of children, and the type of hospital. On the other hand, the results of the t-test demonstrated that only the parental role of the respondent (i.e. mother or father) (p=0.003) and the age of the respondent (p=0.001) had a significant influence on viewing Case 1 as an example of a medical error. As for Case 2, the results of the regression analysis indicated that the variables involved in the study were (R2=0.29) in a low and insignificant interaction with viewing Case 2 as an example of a medical error (F= 1.337, p= 0.245) (Table 2). These variables could account for only 29% of viewing Case 2 as an example of a medical error. On the other hand, the results of the t-test demonstrated that none of the variables had a significant influence on viewing Case 2 as an example of a medical error. Several studies have found, unlike the present study, that the parental role and age of the parent do not affect the way medical errors are perceived (Hobgood et al., 2005; Mazor et al., 2010; Matlow et al., 2010). The reason for the contradiction between the findings might be that it is often mothers who
- 126. are responsible for child care in the Turkish culture and fathers exhibit an insufficient level of interest in their children. For both of the cases, the parents had considerably high scores in the desire for disclosure, legal actions, and reporting. Likewise, it is reported in the literature that parents have a high desire especially for disclosure, punishment for the person or institution committing the error, and reporting with the purpose of preventing the error from being committed again (Hogbood et al., 2005; Mazor et al., 2010; Matlow et al., 2010). Whereas there was not a significant difference (p=0.079) in the mean scores concerning the desire for disclosure between the parents who viewed Case 1 as an example of a medical error and those who did not, there was a significant difference (p=0.019) in this respect between the parents who viewed Case 2 as an example of a medical error and those who did not. In similar other studies, parents who considered a case as not an example of a medical error or an example of a slight medical error were observed to tend to have lower levels of desire for disclosure whereas those who considered a case as an example of a medical error had higher levels of desire for disclosure (Hobgood et al., 2005; Mazor et al., 2010; Matlow et al., 2010). Just as there was not a significant difference (p=0.000) in the mean scores concerning the desire for reporting between the parents who viewed Case 1 as an example of a medical error and those who did not, there was not a significant difference (p=0.000) in this respect between the
- 127. parents who viewed Case 2 as an example of a medical error (5.92±0.49) and those who did not. Similarly, Hobgood et al. (2005), Mazor et al. (2010) and Matlow et al. (2010) observed that parents who considered a case as an example of a medical error had a higher level of desire for reporting. Whereas there was a statistically highly significant difference (p=0.000) in the mean scores concerning the desire for legal actions in case of medical errors between the parents who viewed Case 1 as an example of a medical error and those who did not, there was not a statistically significant difference (p=0.316) in International Journal of Caring Sciences January-April 2018 Volume 11 | Issue 1| Page 385 www.internationaljournalofcaringsciences.org this respect between the parents who viewed Case 2 as an example of a medical error and those who did not. Likewise, other similar studies in the literature have found that parents who view a case as an example of a medical error tend to have higher levels of desire for legal actions (Hobgood et al., 2005; Mazor et al., 2010; Matlow et al., 2010). In other words, the finding on Case 2 is different from those in the literature. The discrepancy might be owing to two reasons. Firstly, there were a small number of parents who did not consider the case as an example of a medical error. Secondly, even those
- 128. parents who did not consider the case as an example of a medical error might have thought that legal actions should be taken in case of medical errors. Conclusion and implications Half of parents hold physicians responsible for medical errors, and almost all of them are of the opinion that patients should be informed about and apologized for medical errors. The great majority of parents accurately view cases as examples of medical errors. Considering that the present study is the first in Turkey to attempt to measure parents’ perceptions of medical errors, it is recommended that the study should be replicated in different regions and on different samples. In addition, further studies could attempt to replicate the present study on parents staying at hospitals so that factors in parents’ perceptions of medical errors can be fully identified. References Alpar R. (2010). Applied Statistics and Validity- Reliability. First Edition, Detay Publishing, Ankara. Altindis S. (2009). The Role of the Patient in Testing Patient Safety. http:/www.sdplatform.com Publishing Date 08.06.2009, Access Date March 2012. Carroll EA. & Buddenbaum JL. (2007). Malpractice Claims Involving Pediatricians: Epidemiology and
- 129. Etiology. Pediatrics, 120:10-17 Clarke JN. & Fletcher P. (2005). Parents as advocates: stories of surplus suffering when a child is diagnosed and treated for cancer. Soc Work Health Care, 39:107-127. Cirpi F., Merih YD. & Kocabey MY. (2009). Identification of Nursing Practices for Patient Safety and Nurses’ Views of Such Practices. Maltepe University Journal of Nursing Science and Art, 2 (3): 26-34. Gokdogan F. & Yorgun S. (2010). Patient Safety and Nurses in Health Services. Journal of Anatolia Nursing and Health Sciences, 13(2): 53-59. Hakverdi YG. (2011). Patient Safety Culture. Journal of Ege University School of Nursing, 27(1): 77- 82. Harris L. (1997). Public opinion of patient safety issues. National Patient Safety Foundation. Hobgood C., Tamayo-Sarver JH., Elms A. & Weiner B. (2005). Parental preferences for error disclosure, reporting, and legal action after medical error in the care of their children. Pediatrics, 116:1276-1286. IOM (1999). Institute of Medicine: To Err is Human: Buılding a Safer Health System. IOM (2003). (Institute of Medicine). IOM: Patient safety: achieving a new standard for care.
- 130. Washington, DC: National Academies Press, Washington. Matlow AG., Moody L., Laxer R., Stevens P., Goia C. & Friedman, JN. (2010). Disclosure of medical error to parents and pediatric patients: assessment of parents' attitudes and influencing factors. Arch Dis Child, 95(4):286-90 Mazor KM., Goff SL., Dodd KS., Velten SJ. & Walsh, KE. (2010). Parents' perceptions of medical errors. J Patient Saf., 6: 102-107. Ozkaya N. (2008). Between 2002-2006 by the Council of Forensic Medicine 3rd Specialization Reported Opinions Pediatric Malpractice Medical Malpractice Claims Involving Investigation and Identification of Decision. Istanbul University Institute of Forensic Medicine, Department of Social Sciences Degree Thesis, Istanbul. Slomin AD., LaFleur BJ., Ahmed W. & Joseph JG. (2003). Hospital-Reported Medical Errors in Children. Pediatrics. 111(1), 617-621. Copyright of International Journal of Caring Sciences is the property of International Journal of Caring Sciences and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.
- 131. Health, Spirituality and Medical Ethics - Vol.2, No.2, Summer 2015 Improving Patients' Care through Electronic Medical Error Reporting System Fatemeh Rangraz Jeddi1*, Fatemeh Atoof2 1 Associate professor of Health Information Management. Kashan University of Medical Sciences, Kashan, Iran 2 PhD Student. Tehran University of Medical Sciences. Tehran, Iran [email protected] mail:-E. Fatemeh Rangraz Jeddihould be addressed SCorrespondence: *
- 132. Abstract Background and Objectives: Medical errors are unintentional acts that take place due to the negligence or lead to undesirable consequences in medical practice. The purpose of this study was to design a conceptual model for medical error reporting system. Methods: This applied descriptive cross-sectional research employed Delphi method carried out from 2012 to 2013. The study population was medical and paramedical personnel of health workers and paramedical personnel of hospitals, deputy of treatment, faculty members of Kashan University of Medical Sciences in addition to the internet and library resources. Sample size included 30 expert individuals in the field of medical errors. The one-stage stratified sampling procedure was used. The items with opposition ranging 0 to 25 were confirmed and those exceeding 50 were rejected whereas the items with the opposition 25 to 50 were reevaluated in the second session. This process continued for three times and the items that failed to be approved were eliminated in the model.
- 133. Results: Based on the results of this research, repeated informing about and reporting operation at on-line bases that have access to the incidence of error detected on time, identifying cause and damage due to the incidence reported confidential and anonymously immediately after the occurrence is necessary. Analysis of data quantitatively and qualitatively by using computer software is needed. Classifying the errors reports based on feedback provision according to the cause of error is needed. In addition, confidential report and possible manual retrieval were suggested Conclusion: It is essential to determine the means of reporting and items in the reporting form including time, cause and damage of medical error, media of reporting and method of recording and analysis. Keywords: design, informing, medical error, reporting,system. Original Article Health, Spirituality and Medical Ethics. 2015;2(2):22-29 Please Cite This Article As: Rangraz Jeddi F, Atoof F. Improving Patients' Care through
- 134. Electronic Medical Error Reporting System. Health, Spirituality and Medical Ethics. 2015;2(2):22- 29. Health standards are a set of procedures and acts to ensure the regaining of patient's health. They are logical acts and well-defined goals that are mandatory to be followed by the practitioners based on the condition and the accessible facilities (1). The occurrence of medical errors in extensive professions such as medical settings is not unusual and the medical professionals are always seeking means by which to avoid Introduction edical errors are unintentional acts that occur due to the negligence or carelessness which fail to lead to a desirable consequence in medical practice. A medical error is defined as the action made or decision taken in a health-
- 135. care setting that does not conform to the health standards set in the field. M Improving Patients' Care through Electronic Medical Error Health, Spirituality and Medical Ethics - Vol.2, No.2, Summer 2015 or reduce them. Since many cases of medical errors are not reported, estimating an approximate rate is very difficult (2). According to the results of a research, 195000 deaths take place every year due to medical errors (3). The main cause of many medical errors is the insufficient access to information at the time of decision making and poor communication among the caring team that usually work in
- 136. manually operating systems. Sedghiani has indicated that one of the items in regard to the evaluation of hospital is the inclusion of error report form, its analysis and the result of such report on the delivery of services (4). There are many ways for reducing medical errors and increasing the safety of patients (5). One of them is discovering the errors through employing a reporting system (6). A health care system will benefit from discovering a medical error only when there is a comprehensive program and proper mechanism for analyzing the condition under which the error took place and then implement appropriate measure to prevent its recurrence (7). Such a management system requires understanding of the causes of errors and introducing plans to prevent them before they lead to harmful occurrences; a
- 137. system that will propose strategies and guidelines to avoid the likely errors and dangers that may occur in future. Error reporting systems employ efficient methods for eliminating errors in a health care system. Error reporting may be committed voluntarily or involuntarily. The voluntary method of error reporting is done by physicians and personnel within the medical centers who are directly in contact with patients either para- clinically or clinically. The involuntary reporting is carried out according to the assignment and duties defined by the health care and medical service system (8). The result of researches have indicated that systems that employ voluntary and involuntary error reporting method are more efficient and more errors are reported by physicians so that that the
- 138. rate of reporting increases 20 times (10). The importance of error reporting system is such that many medical centers conduct error reporting through their computer systems (11, 12). A successful error reporting system must be confidential and non-punitive. The analysis of errors and reporting their explanation must be performed by expert personnel who understand the clinical cares and causes of error systems. The report must be available on time. It must rely on and emphasize the processes instead of individuals; it must be capable of responding appropriately to the needs of the system; employ proper media and be accessible to the public. In designing the medical error reporting system, it is important to focus on systems, processes and services instead of individuals. The system must be able to provide the appropriate responses to
- 139. the beneficiary organization; it must be easy to learn and use and release its result in a suitable medium and be accessible to the public. The design of medical error reporting system must focus on important issues such as the reporting of events, ease of using computer technology and even web, evaluation of effectiveness, and capability of executive system review of goals, and obstacles in the use of reporting system, procedures for classification and reporting errors (8, 13. 14). The purpose of this research was to design a conceptual model for medical error reporting system that has the capability of reducing the medical errors and facilitating management affairs. Methods: This applied descriptive cross-sectional
- 140. research employed Delphi technique between 2012 to 2013. The study population was medical and paramedical personnel. Sample size included 30 expert individuals in the field of medical errors. The means of determining sample size was the one- stage stratified sampling procedure. The experts were selected from 5 categories including 3 physicians (faculty members), 17 nurses, 2 midwifes, 7 paramedics and one manager. The selection was based on the proportion of every profession. The inclusion-exclusion criteria were based on the involvement of the experts in the occurrence of medical errors, who were working in the offices of clinical governance or members of the committees’ accreditation assessment of the hospitals. The questionnaire was based on the
- 141. Rangraz Jeddi F, et al Health, Spirituality and Medical Ethics - Vol.2, No.2, Summer 2015 library resources aligned with the research objectives. The validity of the questionnaire was confirmed through face and content validity and question items were corrected based upon opinions of 3 experts. To calculate the reliability of the questionnaire, split-half method was used and alpha level equal to 0.76 was calculated. The first draft of the questionnaire was presented to the experts. The item with opposition ranging 0 to 25 was confirmed and those exceeding 50 were rejected whereas the items with the opposition between 25 to 50 were put forward to the next step and reevaluated in the second session. This process continued for three times and the
- 142. items that failed to be approved were eliminated in the model. Results The result of analysis of data indicated that informing the personnel about the reporting medical error is a necessity. The main components of the system are: a) recording the event, b) analyzing and c) feedback and reporting the result (figure 1). In regard to the informing of reporting medical error, the results showed that the highest frequency of agreement among the expert in the first stage of reporting was the written informing form 29 (96.7%). In addition, written informing method by matrons and educational supervisor was deemed necessary while the use of poster and brusher was suggested (table 1). Data analysis also showed that implementing an
- 143. involuntary rule for recording the medical error Table 1. Frequency Distribution of Expert Opinion regarding the Informing System Opinion Item agree Frequency (percent) disagree frequency (percent) No opinion frequency (percent) First stage result Second stage result
- 144. Third stage result method verbal 10 (33.3) 9 (30) 11 (36.7) reassessment remove * written 24 (80) 1 (3.3) 5 (16.7) confirm * * Person in charge matron 15 (50) 5 (16.7) 10 (33.3) reassessment confirm * Educational supervisor 18 (60) 2 (6.7) 10 (33.3) confirm * * media Internet 9 (30) 12 (40) 9 (30) reassessment remove * journal 10 (33.3) 10 (33.3) 10 (33.3) reassessment reassessment remove booklet 12 (40) 8 (26.7) 10 (33.3) reassessment reassessment remove brochure 15 (50) 7 (23.3) 8 (26.7) confirm * * poster 14 (46.7) 11 (36.7) 5 (16.7) reassessment confirm *
- 145. television 8 (26.7) 13 (43.3) 9 (30) remove * * satellite 2 (6.7) 16 (50.3) 12 (40) remove * * characteristics Repeated informing 22 (73.3) 6 (20) 2 (6.7) confirm * * Overall reporting in hospital 29 (96.7) 1 (3.3) 0 (0) confirm * * * did not enter at this stage Improving Patients' Care through Electronic Medical Error Health, Spirituality and Medical Ethics - Vol.2, No.2, Summer 2015 while keeping the reporter animosity and the report confidentially immediately after the incidence is desirable. In addition, rewarding
- 146. the reporter in addition to having a simple and comprehensible method appropriate for the objectives to improve the care and services of health care were confirmed. Moreover, recording the time of incidence, cause and harm inflicted and the title of the person committing the error were also suggested. The result of analysis showed that using electronic and on- line media was necessary. According to experts' beliefs, the medical errors must be analyzed and the cause be identified. In their opinion, quantitative and qualitative analysis using software, statisticians' and experts' views on medical errors is indispensable. All the experts (30, 100%) in the first stage suggested the need to analyze the medical errors. The lowest frequency of agreement was about the necessity to perform
- 147. analysis by the medical record expert (14, 46.7%). The highest frequency of agreement among experts in the first stage was verbal feedback (29, 96.7%) (table 3). With regard to the feedback provision and effectiveness of reporting the result of analysis of medical errors for reducing the errors, the need for classification based on the type of error and maintaining the confidentiality was emphasized by the experts (table 4). Discussion: A medical system of reporting the medical errors demonstrates the performance and capability of the hospitals or other health care centers for presenting the cares based on the safety standards (15-18). Despite the fact that voluntary reporting of medical errors leads to under reporting of the real cases of errors which
- 148. in turn is considered as weakness in the system (19), nowadays such an act plays an important role in reporting the errors and increasing the safety of patient on one hand and on the other hand leads to the development and improvement of the system to reduce medical errors. For these purposes, different methods of medical error reporting are used in many countries (20-21). The results of the present research showed that repeated error reporting, particularly, written Table 2. Frequency Distribution of Expert Opinions about the Recording of the Events Third stage result Second stage result First stage
- 149. result No opinion frequency (percent) Disagree Frequency (percent) Agree frequency (percent) Opinion Item * * remove 4 (13.3) 14 (46.7) 12 (40) Arbitrary recording the error R eco rd in g M
- 150. eth o d confirm reassessment reassessment 9 (30) 5 (16.7) 16 (50.3) Compulsory reporting the error * confirm reassessment 9 (30) 6 (20) 5 (16.7) Animosity of the reporter of error * * remove 9 (30) 13 (43.3) 8 (26.7) Known reporter of error * confirm reassessment 5 (16.7) 3 (10) 22 (73.3) Confidentiality of the error recorded confirm reassessm ent reassessment 5 (16.7) 7 (23.3) 18 (60) Recording the error by the committer * * confirm 4 (13.3) 0 (0) 26 (86.7) Recording immediately after the incidence confirm reassessment reassessment 11(36.7) 2 (6.7) 17 (56.7) Rewarding the error recorder C h
- 151. aracteristic o f reco rd in g th e ev en ts * * remove 9 (30) 18 (60) 3 (10) Punishing the error recorder * * confirm 1 (3.3) 1 (3.3) 28 (93.3) Plain design * * confirm 1 (3.3) 1 (3.3) 28 (93.3) Clear design * * confirm 0(0) 0 (0) 30 (100) Comprehendible design * * confirm 0 (0) 0 (0) 30 (100) In line with the goals of care and control * * confirm 0 (0) 2 (6.7) 28 (93.3) Recording the time of error A t least o f
- 152. elem en ts * reassessm ent reassessment 4 (13.3) 4 (13.3) 22 (73.3) Recording the responsibility of the reported * * confirm 0 (0) 0 (0) 30 (100) Recording the cause * * Confirm 0 (0) 1 (3.3) 29 (96.7) Recording the damage due to error * confirm Reassessment 3 (10) 6 (20) 21 (70) Internet m ed ia * * confirm 4 (13.3) 10 (33.3) 16 (50.3) electronic * * confirm 2 (6.7) 5 (16.7) 23 (76.7) Hospital information system Rangraz Jeddi F, et al
- 153. Health, Spirituality and Medical Ethics - Vol.2, No.2, Summer 2015 ones by the matrons and educational supervisors is necessary. While the use of posters and brochures are also suggested for this purpose . Jerico suggested the use of educational intervention program to increase the incidence of medical error reports (22). The result of a study conducted in an educational hospital indicated that 54.8 percent of the physicians knew the method of reporting medical errors and only 39.5 percent of them were familiar with what errors need to be reported (23). In another study, 98 percent of the health workers were aware of the reporting system while 25 percent knew how to use these reports (24). Mcneil et al. reported that 71 percent of the medical workers were familiar with the system
- 154. of error reporting (25). White et al. indicated that only 31 percent of the intern and resident students received instruction about how to complete an error reporting form (26). All these evidence show that reporting the medical errors is necessary and must be consistently performed. The present research emphasized that recording the errors has to be obligatory, anonymous and confidential. It should also be done immediately after the incidence along with rewarding the reporter. Simple and comprehensible design, recording the time and cause of the harm in addition to the status of person committing the error were confirmed as the minimum measures of recording . This is similar to the results of investigators that claimed the medical error reports must be
- 155. confidential with no punishment consequences and unrelated to the authorities exercising punishing act in addition to being simple and comprehensible and provide the opportunity to report the incidence (7, 8, 17, 27, 28). These systems need to be designed in a way that maintains the identity of the reporter anonymously and keeps the records confidentially (27, 29). In addition, the information related to the incident should include the cause of error, the harm inflicted and the reason for the occurrence (8, 27). Some of studies in this regard suggest other information such as the date of incidence and reception of report, ward of the hospital where the event took place and the severity of incident is recorded Table 3. Frequency Distribution of Expert Opinion about the Analysis of Medical Errors
- 156. Opinion Item Agree Number (%) Disagree Number (%) No opinion Number (%) Result of first stage Need to analyze 29 (96.7) 1 (3.3) 0 (0) confirm Cases examined cause 30 (100) 0 (0) 0 (0) confirm Reason of recurrence 29 (96.7) 0 (0) 1 (3.3) confirm Type of analysis quantitative 19 (63.3) 4 (13.3) 7 (23.3) confirm qualitative 26 (86.7) 1 (3.3) 3 (10) confirm analyzer Statistical software 21 (70) 3 (10) 6 (20) confirm statistician 17 (56.7) 4 (13.3) 9 (30) confirm Medical record expert 14 (46.7) 6 (20) 10 (33.3) remove Hospital's matron 16 (53.3) 5 (16.7) 9 (30) confirm
- 157. Expert of medical error 29 (96.7) 0 (0) 1 (3.3) confirm * did not have second and third stage Table 4. Frequency Distribution of Expert Opinion about the Feedback and Reporting the Result of Analysis of Medical Errors Opinion Item Agree Number (%) Disagree Number (%) No opinion Number (%) Result of first stage Goal Error reduction 27 (90) 2 (6.7) 1 (3.3) confirm Classifying errors 27 (90) 0 (0) 3 (10) confirm Method of maintaining confidential 24 (80) 1 (3.3) 5 (16.7) confirm Non-confidential 4 (13.3) 18 (60) 8 (26.7) remove Retrieval method