
Recommended
More Related Content
Similar to The endocrine emergencies most commonly discussed by EMS provi.docx
Similar to The endocrine emergencies most commonly discussed by EMS provi.docx (20)
More from todd701
More from todd701 (20)
Recently uploaded
Recently uploaded (20)
The endocrine emergencies most commonly discussed by EMS provi.docx
- 1. The endocrine emergencies most commonly discussed by EMS providers typically deal with diabetes mel-litus, a condition associated with malfunction of the pancreas or its hormones and improper regulation of the blood glucose level. It is important to recognize that there are many other emergencies that may be related to malfunctioning endocrine glands or hormones. These emergencies may produce acute life-threatening conditions that exhibit a wide variety of clinical presentations based on the gland or hormones involved. Some patients may not readily recognize, or may ignore, the slow and progressive clinical changes that are occurring and allow the disease to create an acute life-threatening condition. Since EMS providers may be called upon to manage the patient experiencing this acute and potentially life-threatening condition, it is prudent for them to possess an awareness and understanding of other potential life-threatening endocrine emergencies, such as those involving the thyroid gland and its related hormones. By Joseph J. Mistovich, MEd, NREMT-P, William S. Krost, BSAS, NREMT-P, & Daniel D. Limmer, AS, EMT-P Part 1: Hyperthyroidism and Thyroid Storm This CE activity is approved by EMS Magazine, an
- 2. organization accredited by the Continuing Education Coordinating Board for Emergency Medical Services (CECBEMS), for 1.5 CEUs. OBJECTIVES • Review anatomy of the thyroid gland • Discuss metabolic disturbances • Review emergency management of endocrine emergencies Sponsored by CONTINUING EDUCATION FROM EMS endocrine emergencies This article is the first in a two-part series addressing endocrine emergencies involving thyroid hormone disorders. The second part will follow in next month’s issue and cover conditions related to hypothyroid- ism. The section below on anatomy and physiology of the
- 3. thyroid gland pertains to both articles. It will be important to review this section prior to reading the next article to completely understand the hypothyroid- ism conditions covered in part two. BEYOND THE BASICS:BEYOND THE BASICS: Part 1: Hyperthyroidism and Thyroid Storm This CE activity is approve by EMS Magazine, an organization accredited by the Continuing Education Coordinating Board for Emergency Medical Services (CECBEMS), for 1.5 CEUs. OBJECTIVESJ • Review anatomy of the thyroid gland • Discuss metabolic disturbances • Review emergencyThis article is the first in a two part series addressing endocrine emergencies involving thyroid hormoneThis article is the first in a two part series addressing
- 4. endocrine emergencies involving thyroid hormone ENDOCRINEENDOCRINE EMERGENCIESEMERGENCIES P h o to s b y D an L im m e r www.emsresponder.com ■ EMS ■ OCTOBER 2007 123 123-127 ce article.indd 123123-127 ce article.indd 123 9/18/2007 3:38:33 PM9/18/2007 3:38:33 PM ANATOMY AND PHYSIOLOGY OF THE THYROID GLAND
- 5. The thyroid is a butterfly-shaped endocrine gland located in the ante- rior neck just inferior to the thyroid cartilage (Adam’s apple). It consists of two lateral lobes that are connected anteriorly by a mass of tissue referred to as the isthmus. It can be easily pal- pated just below the cricoid cartilage. The size of the gland varies in indi- viduals depending on many factors. The thyroid gland is the largest pure endocrine gland in the body and has a very rich blood supply. Thus, when performing a needle cricothyrotomy, it is extremely important to ensure that the proper landmarks have been identified to avoid inadvertent lac- eration of the vascular lateral lobes or isthmus of the thyroid gland. If these are lacerated, an excessive amount of bleeding may occur, complicating an already dire airway situation. The gland may also be lacerated and bleed heavily from blunt or penetrat- ing trauma to the anterior neck. The thyroid gland produces and secretes two distinct hormones: thy- roid hormone (TH) and calcitonin. Calcitonin is produced by a differ- ent group of cells within the thyroid gland, and is responsible for lowering the blood levels of calcium and stim- ulation of bone growth and develop- ment in childhood. It may also play a
- 6. role in reducing bone loss associated with starvation and in late stages of pregnancy when the fetus is compet- ing for calcium being absorbed in the digestive tract. Otherwise, the role of calcitonin in the healthy adult is not well understood; it may serve merely as a weak hypocalcemic agent. The thyroid hormone is comprised of two different iodide-attached mol- ecules. Thyroxine, also known as tet- raiodothyronine or T4, makes up the majority of hormone secreted by the thyroid cells. It consists of four iodide ions attached to its molecular struc- ture. Triiodothyronine, also known as T3, is the other hormone secreted by the thyroid gland. It has only three iodide ions attached to it. Although only a small amount of T3 is secreted by the thyroid gland, approximately 10% of the TH secretion, a large amount is formed from the conver- sion of T4 through the removal of one iodine group by enzymes from the liver, kidneys and other tissues. Interestingly, though, T3 is primar- ily responsible for the thyroid hor- mone effect, which is primarily a very strong, immediate and short-acting increase in cellular metabolism. It is important to review the trans- port, binding and concentration of T3 and T4 in the blood in order to
- 7. understand a potential trigger for the disease process involving the thyroid hormone. Approximately 75% of T4 and 70% of T3 hormones attach to thyroid-binding globulins, also known as thyroxine-binding globu- lins (TBGs), upon entering the blood. A majority of the remaining T3 and T4 are attached to the plasma pro- tein albumin or a thyroid-binding prealbumin. Very small amounts of the thyroid hormone, approximately 0.3% of T3 and 0.03% of T4, are left unbound to diffuse into the periph- eral tissue. Thus, the only useable form of thyroid hormone is in an unbound form. Both T3 and T4 bind to target tissue receptors; however, T3 binds much more readily and is about 10 times more active than T4. Equilibrium must be maintained in the blood between the amount of thyroid hor- mones bound to protein carriers and the amount being released into the peripheral tissue. Levels of T4 and the thyroid-stimulating hormone (TSH) play a major role in maintain- ing this blood level equilibrium. It is interesting to note that more than a week’s supply of thyroid hormone is found in the bloodstream. Thyroid hormones affect many of
- 8. the major organ systems and tissues within the body, with the exception of only the adult brain, spleen, testes, uterus and thyroid gland itself. Effects of the thyroid hormones are to: • Maintain normal sensitivity of respiratory centers to changes in oxy- gen and carbon dioxide concentra- tions • Maintain normal cell oxygen use • Maintain a normal basal meta- bolic rate (BMR) • Promote calorigenesis (heat pro- duction) by increasing the metabolic rate of cells • Enhance the effects of the sym- pathetic nervous system • Promote glucose metabolism, fat mobilization and protein synthesis • Maintain normal adult nervous system function • Promote normal cardiac func- tion to include rate and force of contraction • Promote normal muscle devel- opment and function, and skeletal growth and maturation
- 9. endocrine emergencies Patients with hyperthyroidism may experience tachycardia and an elevated systolic pressure. Pulse pressure may also be widened. 124 OCTOBER 2007 ■ EMS ■ www.emsresponder.com 123-127 ce article.indd 124123-127 ce article.indd 124 9/18/2007 3:38:36 PM9/18/2007 3:38:36 PM ce article • Promote normal gastrointestinal (GI) motility and tone, and increase digestive enzyme secretion • Maintain hydration and secre- tory function of the skin. Hypothyroidism, an insufficient number of thyroid hormones, or hyperthyroidism, an excessive num- ber of thyroid hormones, will cause metabolic disturbances that disrupt normal body function and have an impact on most or all of the aforementioned hormone effects. Hypothyroidism results in a decrease in hormonal effects on the body systems; hyperthyroidism increases or accentuates the thyroid hormone effects on body systems. Both condi-
- 10. tions can lead to acute and poten- tially lethal emergencies. PATHOPHYSIOLOGY Hyperthyroidism describes a con- dition of excessive secretion of thy- roid hormone resulting from elevated and inappropriate thyroid function. Thyrotoxicosis, also associated with an excessive amount of circulating thyroid hormone, results from the patient taking too much thyroid hor- mone (an exogenous source), or from an inflamed thyroid gland releasing too much stored thyroid hormone. Although these terms are often used interchangeably to describe an elevat- ed thyroid hormone level, they have different etiologies that affect long- term treatment. Hyperthyroidism and thyrotoxicosis typically describe the milder form of the disease process. Graves’ disease, also known as diffuse toxic goiter, is the most com- mon form of hyperthyroidism. It is typically more common in women and usually occurs between the ages of 20 and 40. Graves’ results from an autoimmune condition that affects the function of the thyroid-stimulat- ing hormone, causing the thyroid gland to increase its production and
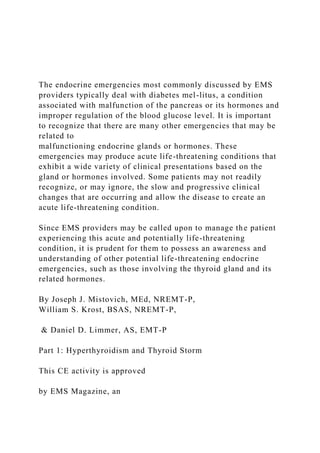
- 11. P h o to c o u rt e sy B e ch ar a Y. G h o ra ye b , M D The enlarged thyroid gland in
- 12. Graves’ is typically diffuse and nontender to palpation. This woman also shows signs of exop- thalmos, which occurs when the tissue behind the eyes becomes edematous and fibrous and the extraocular muscles degenerate. For More Information Circle 105 on Reader Service Card For More Information Circle 106 on Reader Service Card www.emsresponder.com ■ EMS ■ OCTOBER 2007 125 123-127 ce article.indd 125123-127 ce article.indd 125 9/18/2007 3:38:36 PM9/18/2007 3:38:36 PM secretion of thyroid hormone and leading to hyperthyroidism. Thyroid storm, also referred to as thyrotoxic crisis, represents a severe and potentially life-threatening con- dition. Although it is a relatively rare condition, occurring in only 1% to 2% of patients with hyperthyroid- ism, if left untreated, thyroid storm can be fatal, sometimes within days. It carries an adult mortality rate of 10%–20%. The pathophysiology of thyroid storm is not completely understood; however, it is thought that the excessive levels of thyroid hormone are not necessarily from the thyroid gland but from the conver-
- 13. sion of bound-thyroid hormone in the blood to an unbound form. The unbound form becomes active and can easily enter peripheral tissue, producing a dangerous and possibly life-threatening hypermetabolic state and increased sympathetic nervous system activity. The patient may pres- ent with an excessively high fever (106°F), tachycardia, nausea, vomit- ing, diarrhea and hypotension. Graves’ disease is the most com- mon underlying cause of thyroid storm. Other causes include taking an excessive amount of thyroid hor- mone (factitious hyperthyroidism) and administration of amiodarone, a rich iodine-containing antidysrhyth- mic agent that can have complex effects on the thyroid gland and hor- mone function. Other conditions that may precipitate thyroid storm in the patient with hyperthyroidism include: infection, surgery, burns, trauma, cardiovascular events, preeclampsia or eclampsia, diabetic ketoacidosis, hyperglycemic hyperosmolar non- ketotic syndrome, insulin-induced hypoglycemia, pulmonary embolism, ingestion of thyroid hormone and drug reactions (Mellaril, Itrumil). ASSESSMENT It is important to understand the
- 14. history and physical exam findings in a patient with hyperthyroidism. A patient who presents with life- threatening thyroid storm may have an undiagnosed history of hyper- thyroidism. Although hyperthyroid- ism and thyroid storm may present with a wide clinical array of signs and symptoms, clinical features of a hypermetabolic state and increased sympathetic activity are the most common. Key findings include agita- tion, weight loss, nervousness and palpitations. History findings include: • Weight loss of approximately 15% of prior weight (often greater than 40 pounds) • Cardiac palpitations • Nervousness • Anxiety, agitation, restlessness • Wide mood swings • Tremors • Chest pain in the absence of cardiovascular disease • Dyspnea • Edema • Disorientation • Psychosis • Weakness • Diarrhea and increased bowel movements
- 15. • Increased perspiration • Fatigue • Intolerance to heat from the hypermetabolic state • Abdominal pain. Physical exam findings include: • Fever (excessively high in thy- roid storm) • Tachycardia (often 100–170 bpm) that is out of proportion to the fever • Wide pulse pressure (40–100 mmHg) due to the increase in cardiac contractility (inotrope) with an eleva- tion in systolic blood pressure • Warm skin • Diaphoresis • Dehydration (may be secondary to diaphoresis and diarrhea) • Congestive heart failure • Thyromegaly (enlarged thyroid gland) • Exopthalmos (protruded eye- balls) • Stare with eyelid retraction • Atrial fibrillation, atrial flutter, or premature atrial contractions • Tremors
- 16. • Tender liver • Shock • Jaundice • Coma or obtunded mental state. The enlarged thyroid gland in Graves’ is typically diffuse and non- tender to palpation. If there is infec- tion or inflammation, the gland will present with diffuse enlargement and pain on palpation. Exopthalmos occurs when the tis- sue behind the eyes becomes edem- atous and fibrous and the extraocular muscles degenerate. This is thought to result from the autoimmune dis- order associated with hyperthyroid- ism. In some cases, the protrusion is so severe that the optic nerve is stretched and vision is impaired. Severe eyeball protrusion may cause the eyelids to stretch and not close completely when the patient blinks or sleeps. This may lead to drying and irritation of the outer eye tissue, causing corneal ulcerations. It is important for EMS providers to recognize not only the patient experiencing a thyroid storm, but also one who is exhibiting an array of signs and symptoms that are char- acteristic of hyperthyroidism. The
- 17. hyperthyroid condition may progress rapidly to thyroid storm or conges- tive heart failure if not treated. MANAGEMENT Thyroid storm is a life-threaten- ing condition that requires immedi- ate emergency care and transport. Severe hyperthyroidism may also require supportive emergency care. Consider the following when man- endocrine emergencies Photo courtesy Bechara Y. Ghorayeb, MD Surgery to remove an enlarged thyroid gland. The thyroid is normally a butterfly-shaped gland that lies in the anterior neck inferior to the thyroid cartilage. 126 OCTOBER 2007 ■ EMS ■ www.emsresponder.com 123-127 ce article.indd 126123-127 ce article.indd 126 9/18/2007 3:38:38 PM9/18/2007 3:38:38 PM ce article aging a patient with an acute and severe hyperthyroid condition: • Establish and maintain a pat-
- 18. ent airway. If the patient presents with an altered mental status or is comatose, it may be necessary to establish an airway by a manual maneuver, and potentially with a mechanical device, including endo- tracheal intubation, in severely altered mental states. • Establish and maintain an adequate ventilation status. If the patient’s respiratory rate or tidal vol- ume is inadequate, it is necessary to provide positive pressure ventilation. • Establish and maintain ade- quate oxygenation. Assess the patient for evidence of hypoxia. Apply a pulse oximeter and deter- mine the SpO 2 reading. If there is either clinical evidence of hypoxia or a SpO 2 reading of less than 95% on room air, administer a high concentration of oxygen via a non- rebreather mask. If the patient is exhibiting no signs of hypoxia or the SpO
- 19. 2 reading is greater than 95%, supplemental oxygen may be applied via a nasal cannula at 2–4 lpm, especially if any dyspnea, chest pain or congestive heart fail- ure is exhibited during the history or physical exam. • Provide continuous ECG moni- toring. Patients experiencing hyper- thyroidism or thyroid storm may present with cardiac dysrhythmias. Atrial fibrillation is common, espe- cially in the elderly. Patients may also experience atrial flutter and prema- ture atrial contractions. Traditional management of the ventricular rate control in atrial fibrillation or conver- sion to a sinus rhythm may not be effective until the thyroid levels have been managed. • Initiate an intravenous line of normal saline. Patients may lose significant amounts of fluid from excessive sweating and diarrhea. Aggressive fluid resuscitation may be necessary in severe cases. • Initiate cooling measures if high fever is present. Remove the patient’s clothing, mist the body with water
- 20. and fan aggressively. If antipyretic therapy is considered, avoid the use of aspirin. Aspirin may decrease pro- tein binding of thyroid hormones and increase the levels of unbound T3 and T4, thereby increasing the tissue uptake of thyroid hormone. Acetaminophen would be preferred over aspirin since it does not have this effect. • Expeditious transport. If the patient is experiencing a thyroid storm or a severe hyperthyroid con- dition, consider rapid transport to an appropriate medical facility that can initiate definitive therapy to decrease the thyroid hormone levels. • Consider medications. Blockading the peripheral adrener- gic hyperactivity with beta blockers could be a critical factor in man- aging the thyroid storm patient. Propranolol (Inderal), the current beta blocker agent of choice, can reduce tachydysrhythmias, high body core temperature, tremors, restlessness, anxiety and palpitations. Another major indication for the specific use of propranolol is its ability to inhibit the conversion of T4 to T3 in the peripheral tissue. Keep in mind that T3 is responsible for the majority of thyroid hormone activity in the
- 21. peripheral tissue. Contraindications to propranolol’s use include reac- tive airway disease, atrioventricular blocks, bradydysrhythmias, cardio- genic shock, hypersensitivity to the drug and congestive heart failure. It is important to note that heart failure in hyperthyroidism and thyroid storm is typically a high-output CHF, or heart failure due to tachydysrhyth- mias that may respond well to the beta blocker therapy. However, use beta blockers with extreme caution if heart failure is suspected. The dose of propranolol is 1–2 mg intra- venously, repeated every 10 to 15 minutes until the symptoms are con- trolled. Be sure to follow your local protocol in managing the thyroid storm patient. Another medication to consider is dexamethasone (Decadron), which also blocks the conversion of T4 to T3 in the peripheral tissue. Administer 2 mg intravenously. Again, it is impor- tant to follow local protocol when managing the patient. CONCLUSION Even though the chance of responding to a patient experiencing a thyroid storm or thyrotoxic crisis is rare, be prepared to quickly identify
- 22. the severity of the condition and initi- ate rapid supportive emergency care and transport. Possessing a funda- mental understanding of the disease process will better prepare the EMS provider to rapidly recognize and manage this potentially acute life- threatening condition. Bibliography Bledsoe BE, Porter RS, Cherry RA. Paramedic Care: Principles and Practice, Medical Emergencies, 2nd ed. Upper Saddle River, NJ: Prentice Hall Health, 2006. Guyton AC, Hall JE. Textbook of Medical Physiology, 10th ed. Philadelphia: W.B. Saunders, 2001. Marieb EN. Anatomy and Physiology, 2nd ed. San Francisco: Pearson Education, 2005. Martini FH. Anatomy and Physiology. San Francisco: Pearson Education, 2005. Marx JA, Hockberger RS, Walls RM. Rosen’s Emergency Medicine: Concepts and Clinical Practice, 5th ed. St. Louis: Mosby, Inc., 2002. Schraga ED. Hyperthyroidism, Thyroid Storm, and Graves Disease. www.emedicine.com/emerg/ topic269.htm. Joseph J. Mistovich, MEd, NREMT-P, is a professor and chair of the Department of Health Professions at Youngstown (OH) State University, author of several EMS textbooks and a nationally recognized lecturer. William S. Krost, BSAS, NREMT-P, is an operations manager and flight paramedic with the St. Vincent/Medical University of Ohio/St. Rita’s Critical Care Transport Network
- 23. (Life Flight) in Toledo, OH, and a nationally recognized lecturer. Daniel D. Limmer, AS, EMT-P, is a paramedic with Kennebunk Fire-Rescue in Kennebunk, ME. He is the author of several EMS textbooks and a nationally recognized lecturer. Th yroid storm is a life-threatening condition that requires immediate emergency care and transport. www.emsresponder.com ■ EMS ■ OCTOBER 2007 127 123-127 ce article.indd 127123-127 ce article.indd 127 9/18/2007 3:38:38 PM9/18/2007 3:38:38 PM ce reviewce review ENDOCRINE EMERGENCIES 1. The “Adam’s apple” is a commonly used name for the _____. A. Thyroid gland B. Thyroid cartilage C. Cricoid cartilage D. Isthmus 2. The hormone secreted by the thyroid cells is made up mostly of _____.
- 24. A. Calcitonin B. Triiodothyronine C. Thyroxine D. Albumin 3. More than _____ supply of thyroid hormone can be found in the bloodstream. A. One week’s B. Two weeks C. One day’s D. One month’s 4. Thyroid hormones affect many of the body’s major organ systems and tissues, with the exception of the _____. A. Adult brain B. Spleen C. Uterus D. All of the above 5. The effects of thyroid hormone on body systems are accentuated by _____. A. Calorigenesis B. Thyrotoxicosis C. Hypothyroidism D. Hyperthyroidism 6. According to the article, _____ is the most common underlying cause of thyroid storm—a potentially
- 25. life-threatening condition. A. Thyrotoxicosis B. Graves’ disease C. Hypothyroidism D. Excessive levels of T3 7. A patient who is suspected of having thyroid storm may exhibit all of the following signs, with the exception of _____. A. Low-grade fever B. Congestive heart failure C. Tremors D. Atrial fi brillation 8. When examining the patient with suspected hyperthyroidism, the EMS provider would not fi nd _____ in the patient’s history. A. Wide mood swings B. Edema C. Signifi cant weight gain D. Chest pain in the absence of cardiovascular disease 9. _____ is a condition that occurs when tissue behind the patient’s eyes becomes edamatous and the extraocular muscles degenerate. A. Thyromegaly B. Inotrope
- 26. C. Exopthalmos D. Graves’ disease 10. Blockading the peripheral adrenergic hyperactivity with beta blockers can be a critical factor in managing the thyroid storm patient. According to the article, _____ is the current beta blocker of choice for treating hyperthyroidism. A. Atenolol B. Propranolol C. Labetalol D. Betaxolol 11.The thyroid gland consists of two lateral lobes that are connected anteriorly by a mass of tissue, which is called the ____. A. Thyroid cartilage B. Cricoid cartilage C. Fibrous tissue D. Isthmus 12. Concerning management of the patient with thyroid storm, which one of the following statements is not correct? A. It is important to provide continuous ECG monitoring to assess for cardiac dysrhythmias. B. If the patient’s respiratory rate is
- 27. inadequate, provide positive pressure ventilation. C. If fever is excessive, initiate cooling measures and administer aspirin to the patient until the fever subsides. D. Assess the patient for hypoxia and administer oxygen as needed. Sponsored by The following questions are based on Beyond the Basics: Endocrine Emergencies, beginning on page 123. EMS Magazine’s CE Review offers affordable continuing education credits. Simply read the CE article beginning on page 123, then answer the test questions below, marking your answers in the answer strip on the opposite page. The test is worth 1.5 hours of credit approved by the Continuing Education Coordinating Board for EMS (CECBEMS). Upon receiving a grade of 80% or better, participants will be issued a CE certificate that attests to a passing score. The cost per test is $5, or $4 each when you purchase CEU vouchers in advance. You must purchase a minimum of five vouchers in order to qualify for the discount. You can include a completed test when purchasing vouchers. Check the correct answers and mail this entire page, along with your payment of $5, or one CE voucher, and a self-addressed stamped envelope, to: EMS Magazine, CE Review, P.O. Box 7248, Mission Hills, CA 91346-7248. Please allow eight weeks
- 28. for test processing. Photocopies are acceptable. The test must be postmarked by December 3, 2007. Tests postmarked after the expiration date will be returned. Payment can be made by cash, check or credit card. There will be a charge for returned checks. Please complete the appropriate method of payment information on the test. Questions? Call Maribel Lopez at 800/547-7377, ext. 1107. 128 OCTOBER 2007 ■ EMS ■ www.emsresponder.com 128-129 CE test Oct.indd 128128-129 CE test Oct.indd 128 9/18/2007 3:41:20 PM9/18/2007 3:41:20 PM RESEARCH AND REPORTS Salivary Cortisol Levels in Students Challenged with a Testing Stressor KATHLEEN KENWRIGHT, PATTY W LIDDELL, LEONARD BLOOM, AUDREY ZUCKER-LEVIN, ANN H NOLEN, LAWRENCE W FAULKNER, ROSEMARY E BATORSKI OBJECTIVE: The objective was twofold. The focus of the study was primarily to determine if the stress of a particularly difficult exam could cause students to lose the normal diurnal variation seen in human cortisol levels and secondarily, to validate the use of a competitive enzyme immunoassay for salivary cortisol.
- 29. i nDESIGN: Physical therapy students enrolled Research Design were asked to participate in the study by collecting baseline evening and morning salivary Cortisols during what was regarded as a relatively stress free time in the Fall of 2009. The following spring, the same students were asked for samples the evening before and morning of their first Kinesiology test, traditionally a stressful time. Method validation was accomplished using instrumentation owned by the Medical Laboratory Science (MLS) Program and analysis was performed by MLS faculty and a second year MLS student. SETTING: Participants were enrolled in the College of Health Sciences at the University of Tennessee in Memphis. Sample collection and testing was performed in the student laboratory of the Medical Laboratory Science Program. PARTICIPANTS: Physical therapy students in their first year of a three-year entry level doctorate program, DPT. RESULTS: This group of students did not lose their diurnal variation of cortisol. However, an unexpected finding was noted: the students' salivary cortisol specimen collected in the morning of the fall semester was significantly higher than the salivary cortisol specimen collected the morning of the test in the spring semester (p = .019). Method validation was successful demonstrating a strong correlation ( r = 0.915) when compared to the reference laboratory. C O N C L U S I O N S : Cortisol diurnal variation was not lost in the study participants, but further studies should
- 30. be performed due to the low percentage of students completing the study and the lack of demographic diversity. Even though the method validation in the student laboratory setting demonstrates that it is indeed possible to obtain the same excellent correlation as is seen in a clinical setting, the student laboratory is not CLIA certified, so assays can be performed for research use only. ABBREVLTIONS: ACTH-adrenocorticotropic hor- mone, CRH-corticotrophin-releasing hormone, D P T - Doctorate in Physical Therapy, BS-Baccalaureate of Science, BA-Baccalaureate of Arts, IRB-Internal Review Board, GPA-Grade Point Average, EIA-Enzyme Immunoassay, BMI-Basic Metabolic Index, CLIA- Clinical Laboratory Improvement Amendments, N D - none detected INDEX TERMS: stress, cortisol, exams, students Clin Lab Sei 2011;24(4):221 Kathleen Kenwright, MS, MT,(ASCP)SL,MB"^, University of Tennessee Health Science Center, Memphis, TN38163. Patty W. LiddellMS, MT(ASCP)SH, Baptist College of Health Sciences, Memphis, TN 38163 Leonard Bloom MPH, CT(ASCP), The University of Tennessee Health Science Center, College of Allied Health Sciences, Memphis, TN. Audrey Zucker-Levin PT, PhD, MBA, GCS, The University of Tennessee Health Science Center, College of
- 31. Allied Health Sciences, Memphis, TN. VOL 24. NO 4 FALL 2011 CLINICAL LABORATORY SCIENCE 221 RESEARCH A N D REPORTS Ann H. Nolen, Psy.D., OTR, FAOTA, The University of Tennessee Health Science Center, College o/^Allied Health Sciences, Memphis, T N . Lawrence W. Faulkner, Ph.D. OTIL, The University of Tennessee Health Science Center, College of Allied Health Sciences, Memphis, TN. Rosemary E. Batorski, MEd, MOT, OTR, The University of Tennessee Health Science Center, College of Allied Health Sciences, Memphis, TN Address for Correspondence: Kathleen Kenwright, MS, MT,(ASCP)SI,MB^^, University of Tennessee Health Science Center, 930 Madison Avenue, Suite 672, Memphis, TN 38163, 901-448-6338, [email protected] edu I N T R O D U C T I O N Cortisol is a steroid hormone produced by the adrenal glands in response to adrenocorticotropic hormone (ACTH) secreted by the pituitary.' The typical ditirnal
- 32. variation of cortisoi secretion has been well established. Cortisol shows an increase in the early morning hours, peaking at or slightly before the time of waking, and decreases in the evening.' This hormone plays an important role in maintaining homeostasis by affecting multiple organ systems and processes. Under stressful situations, the body responds by increasing the production of cortisoi by initiating a series of events involving the hypothalamus, pituitary and adrenal cortex called the H PA axis. Specifically, corticotrophin- releasing hormone (CRH) released by the hypothalamus triggers release of adrenocorticotropic hormone (ACTH) from the pituitary which in turn causes the secretion of glucocorticoids from the adrenal cortex.' The strength of the stimulus causes some variation in circadian peak levels and the normal variation has been shown to be disrupted during times of stress.^ Effect on memory Though elevated cortisoi in response to stress is a natural response, it is sometimes detrimental for students in that some forms of memory are impaired. There is abundant evidence that the secretion of glticocorticoid stress hormones may modulate memory functioning.'* The frontal lobe and hippocampus in humans contain a high density of glucocorticoid receptors and are areas for cognition and emotion. During times of stress there may be a pronounced deficit in working memory but at the same time, enhancements may be seen associated with other forms of memory.' MATERIAL AND M E T H O D S Multidisciplinary Project
- 33. Four departments within the College of Allied Health at the University of Tennessee Health Science Center participated in various aspects of this project. The following outlines some goals anticipated by the faculty of the departments involved in the study. The purposes of this multidisciplinary project were to: r- Validate salivary cortisoi in our Clinical Laboratory Science (MLS) student laboratory. " Determine if the stress of an exam would cause students to lose their normal diurnal variation of cortisoi. '- Determine if there is a correlation between cortisoi concentration and a test grade. Determine if there is a correlation between students' perceived stress and the biological marker of stress-cortisol. To serve as a working example of research design to physical therapy students starting a research course. -- Provide opportunities for multi-disciplinary scholarly activity to tenured and non-tenured faculty. This paper will focus on only two aspects of the study: the method validation and whether or not the students lose their diurnal variation when challenged with a Stressor. Participants After IRB approval was obtained, the entire student body, of the first year physical therapy class, was
- 34. approached at the beginning of a structured lecture to ask for their participation in the project. These students were in their fourth month (4''') of a thirty three (33) month entry-level Doctor of Physical Therapy (DPT) program. All students had a BA or BS degree prior to admission to the program. The study was explained in detail and informed consent was obtained from 50 students. Of these 50 students, 23 completed the research protocol. The students who completed the study were on average 23 (± 1.21) years old; 18 female. 222 VOL 24, NO 4 FALL 2011 CLINICAL LABORATORY SCIENCE RESEARCH A N D REPORTS 5 male; 22 Caucasian, 1 Asian, 1 Hispanic with an average undergraduate GPA of 3.54 (±.27) and an average GRE score of 1025 (±92.7). Design Salivary rather than serum or plasma samples were obtained because levels measured in saliva agree very well with the amount of free cortisol in blood.** Studies have shown that the rate of saliva production does not affect the level of cortisol present.^ Using saliva also eliminated the possibility of falsely increased cortisol due to anxiety associated with venipunctures. Baseline salivary cortisol samples were obtained during the beginning of the first semester at a time that was deemed less academically stressful. Test samples were collected the second semester, one in which they take
- 35. 36 credits. This heavy course load makes this semester particularly difficult for the students and an ideal time to test how stress influences performance. Students were given specific instructions to follow (Table 1) for all collections and asked to refrigerate the specimens collected in the evening and bring them to campus the following day. For the baseline samples collected in November 2009, participants were asked to collect 1 mL of saliva at home between 7:30 and 8:30 pm. The subjects collected their saliva samples by drooling, through a straw, into a 2 mL polypropylene screwcap tube. The specimens were refrigerated overnight and brought to campus the next morning. Participants collected a morning sample the day after their evening collection between 7:30 and 8:00 am. Table 1. Instructions for students Sample collection instructions: Do not collect a sample if you have a fever. Avoid alcohol for 12 hours before sample collection. Do not eat a major meal within 60 minutes of sample collection. Avoid dairy products for 20 minutes before sample collection. Avoid foods with high sugar or acidity or high caffeine content immediately before sample collection. Rinse mouth with water to remove food residue before sample collection. Please refrigerate samples overnight. In February of 2010, the second semester, the same participants were again asked to collect an evening saliva sample at home between 7:30 and 8:30 pm the evening before their 8:00 am kinesiology exam. Many students
- 36. also collected their morning sample at home and brought it in with them. Specimens were collected Sunday night and Monday morning before the test. Exclusion criteria Students previously diagnosed with a condition related to variation in cortisol such as Cushing s syndrome or Addison's disease' were excluded from the study. In addition, students taking steroid medication either oral, nasal or topical were not enrolled. Students were asked to avoid the following situations that have been shown to affect cortisol levels: excessive exercise, smoking, and food or alcohol intake immediately prior to obtaining a sample.'* Salivary cortisol determination An enzyme immunoassay method purchased from Salimetrics* was used to determine the salivary cortisol levels. This method was chosen because it used a matrix which accommodated the use of saliva." Other methods available are designed for serum/plasma but are not validated for saliva. After samples were brought to campus, they were stored at -20°C until assayed. Saliva was thawed, vortexed, and centrifuged at 1500 x g for 15 minutes to spin down any mucus in the sample. The assay was performed by following the package insert from Salimetrics" (State College, PA).« A BIO-TEK, Inc. ELx800 Absorbance Microplate Reader, set at 450 nm wavelength, was used to perform the cortisol assays in the MLS student chemistry laboratory. Raw data (absorbance values) was sent to Salimetrics for interpretation using Gen5™ data analysis software, a program that was not installed on our instrument at the time.
- 37. Method Verification Ninety-one salivary cortisol samples from participants were assayed in-house as previously described. Aliquots of these samples were also sent, on dry-ice, to Salimetrics for correlation. Statistical analysis was performed using SPSS 18.0 PASW Statistics. A paired sample t-test and Pearson correlation was performed (n=91) on the split samples performed in the student lab and sent to Salimetrics. The paired sample correlation r =.915 and p < .001 VOL 24, NO 4 FALL 2011 CLINICAL LABORATORY SCIENCE 223 RESEARCH A N D REPORTS showed a very strong correlation between the two methods (Figure 1). An intra-assay coefficient of variation was 5.5%. Cortisol Test Comparison u T H S C L A B
- 38. 1.6 1.4 1.2 1 0.8 0.6 0.4 0.2 0 Salimetrics Figure 1. Method Verification - Ninety-one salivary eortisol samples were assayed at U T H S C and at Salimetrics. A laboratory offering the salivary eortisol testing for clinical purposes would be required to perform a more in-depth verification protocol. Sensitivity, specificity and lower limit of detection assays were not performed. RESULTS Interpretation of the students' eortisol values (n=23) showed a mean fall evening value of .075 ug/dL, a mean fall morning value of 0.63 ug/dL, a mean test evening value of 0.08 ug/dL, and a mean test morning value of 0.41 Ug/dL (Table 2). Ranges are shown on Table 3. The normal diurnal variation between evening and morning samples did occur with evening samples reading lower than morning samples. A paired samples t-test comparing the difference between the evening and morning values collected in the fall (baseline), compared with the difference
- 39. between the evening and morning values collected in February (test) showed a statistically significant difference (p =.028). There was a greater difference in the evening and morning values during the non-stressful Table 2. Salivary eortisol values* Baseline Fall eveninj; Ba.seline Fall morning Test Spring evening Test Spring morning N 23 23 23 23 •"All vaiues are reporrcd in iig/dL. Table 3. Salivary eortisol ranges* Range Minimum Maximum Fall evening .19
- 40. .01 .20 Mean 0.075 0.6300 0.0809 0.4117 Fall - - Std. deviation 0.05955 0.033694 0.11955 0.26819 Morning 1.47 .19 1.65 Expected value males age 21-308
- 41. ND-.308 0.112-0.743 ND-.308 0.112-0.743 Test Evening .47 .02 .49 Expected value females age 21-308 ND-0.7403 0.272-1.348 ND-0.7403 0.272-1.348 Test Morning .95 .04 .99 *Ali values are reported ¡n ug/dl..
- 42. semester (mean = .5557), than the difference in the evening and morning values during the test semester (mean = .3291). Cohen's d effect size = .4. Interestingly, this difference was due to lower eortisol values on the morning of the test than on the morning they were collected in the fall. A paired samples t-test comparing the difference in the baseline morning eortisol value (mean = 0.6300) and test morning eortisol (mean = 0.4117) showed a statistically significant difference p = .019. Results for the paired samples t-tests are shown in Table 4. Power analysis was not performed with this pilot study because estimates of effect size and sample variance must be known before conducting a power analysis.''"' When larger studies are performed, researchers can 224 VOL 24, NO 4 FALL 2011 CLINICAL LABORATORY SCIENCE RESEARCH A N D REPORTS utilize effect size estimates from pilot data such as the current study. Cohen's d effect size was calculated by subtracting baseline diurnal differences from test diurnal differences and dividing by the pooled estimate of variance. Table 4. Paired samples t-test her fall evening value was abnormally high and inconsistent with the rest of her results. This may have been due to a collection error, medication, or a personal
- 43. issue. Pair 1 Pair 2 Pair 3 fall difference- test difference fall evening-test evening fall morning-test morning df 22 22 22 S ig. (2-tailed) .028* .826 .019* 'denotes statistical significance, p < ,05 DISCUSSION People are able to maintain relative homeostasis because the human body naturally responds to stressful situations in ways that allow us to react appropriately. Dealing with stress for prolonged periods of time will eventually affect us adversely." Students deal with the stress of school individually with some thriving but others struggling to cope. Helping students learn how to cope with academic pressures benefits all involved. In this group of students, the cortisol level prior to the stressful event did not increase as expected. This may be due to the fact that the students had an additional day
- 44. to study due to weather related closing of the campus. Another explanation might be that these students have been coping with this type of Stressor for the last four or five years resulting in desensitization. Repeated exposure to the same Stressor can result in desensitization or failure to respond. This is called adaptation or habituation." Another explanation could be that these students as a group have developed skills that allow them to manage test related stress. The students are selected through a competitive process using criteria that would exclude students who succumb easily to the stress of an exam. This initial small sample study made the researchers aware of problems that should be addressed before a larger study is designed. When participants bring in specimens collected at home, investigators need to make sure the specimen is properly labeled before the participant leaves. Several participants were dropped from the study because the collection tubes were not labeled. One sample was lost because the cap was not tightened properly and the specimen leaked. One participant's data was deleted from the study because Cortisol diurnal variation was not lost in the study participants, but further studies should be performed due to the low percentage of students completing the study and the lack of demographic diversity. The weekend immediately before the test, the students had an unexpected 3-day weekend due to a weather- related closure of the university. It is possible that this extra day to study decreased the stress the students would have otherwise felt. Also, these physical therapy students tend to be more physically active, compared to a more generalized adult population, which could affect the results.
- 45. C O N C L U S I O N S Diurnal variation of cortisol was not lost in the study participants but further studies need to be performed due to the low number of participants completing the study and the lack of demographic diversity. Other variables that should be controlled, in future studies, include: physical activity level, grade point average, and body mass index (BMI). Even though the method validation performed in the student laboratory setting demonstrates that it is indeed possible to obtain the same excellent correlation as is seen in a clinical setting, the student laboratory is not CLIA certified so assays can be performed for research use only. The fact that the students' cortisol levels were significantly higher in the fall semester than the spring semester has raised some interesting questions that will be investigated in the future. One such question is, "Does the stress of life events, including moving to a new location, affect students more than academic Stressors"? A C K N O W L E D G E M E N T S The authors would like to thank Thomas A. Hughes M.D. at the University of Tennessee Health Science Center for his advice on this project. Kametricia N. Derricks is gratefully acknowledged for her contributions. This project was supported with a seed grant from the College of Allied VOL 24, NO 4 FALL 2011 CLINICAL LABORATORY SCIENCE 225
- 46. RESEARCH A N D REPORTS Health Sciences at the University of Tennessee Health Science Center. REFERENCES 1. Burtis CA, Ashwood, E.R., Bruns. D.E. Tietz Textbook of Clinical Chemistry and Molecular Diagnostics, 4th ed. St. Louis: Elsevier Saunders; 2006. 2. Kaiman B, Grahn R. Measuring Salivary Cortisol in the Behavioral Neuroscience Laboratory. The Journal of Undergraduate Neuroscience 2004;2:A41-9. 3. Kudielka B, Kirschbam C. Sex differences in HPA axis responses to stress: a review. Biological Psychology 2005:69:113-32. 4. Smeets T, Dziobek I, Wolf O. Social cognition under stress: Differential effects of stress-induced cortisol elevations in healthy young men and women. Hormones and Behavior 2OO9;55:5O7-13. 5. Luethi M, Meier B, Sandi C. Stress effects on working memory, explicit memory, and implicit memory for neutral and emotional stimuli in healthy men. Frontiers in Behavioral Neuroscience. Available from: http://www.frontiersin.org/ behavioral_neuroscience/10.3389/neuro.08.005.2008/full. Jan, 2009 [cited Jan 14, 2011]. 6. Arafah B, Nishiyama F, Tlygeh H, Hejal R. Measurement of Salivary Cortisol Concentration in the Assessment of Adrenal Function in Critically III Subjects: A Surrogate marker of the
- 47. Circulating Free Cortisol. J Clin Endocrinol Metab 2007;92:2965-71 7. Vining R, McGinley R. The measurement of hormones in saliva: Possibilities and pitfalls. J Steroid Biochem. 1987;27:81- 94. 8. Salimetrics'". High Sensitivity Salivary Cortisol Enzyme Immunoassay Kit. July 2009. State College, PA. 9. Statistical Computing Seminars: Introduction to Power Analysis. Available from: http://www.ats.ucla.edu/stat/ seminars/intro_power/default.htm [cited March 30, 2011]. 10. Lenth, R.V., Statistical Power Calculations, J. Anim. Sei. 2007;85:E24-9. 11. Miller D, O'Callaghan J. Neuroendocrine Aspects of the Response to Stress. Metabolism 2OO2;51:5-1O. ASCLS Certification Maintenance Membership Eosily earn CE credit • Certification Maintenance Mem- bership (CMM) - Renewing or joining mcmbcrs can select the CMM option to automatically subscribe to 12 hours of P.A.C.E.*approved online continuing edu- cation credit for only $55 plus national and state dues - C^A^A is a 1 year subscription with MediaLab, Inc.
- 48. - the 12 courses cover designated disci- IIB. he. • Certification Maintenance Membership Plus (CMMP) - upgrade to unlimited hours of pline areas for the Board of Certifica- CE and select the courses you want for $95 tion (BOC) Certification Maintenance plus national and state dues; 1 year subscrip- Program tion For more information, visit www.0scls.0r9/cmm or emoil [email protected] V American Society for Clinical Loborotory Science, 2025 M Street NW, Suite 800, Washington, DC 20036 i 226 VOL 24. NO 4 FALL 2011 CLINICAL LABORATORY SCIENCE Copyright of Clinical Laboratory Science is the property of American Society for Clinical Laboratory Science and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use.