
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Pancreas by dr. bijendra mishra
Similar to Pancreas by dr. bijendra mishra (20)
Recently uploaded
Recently uploaded (20)
Pancreas by dr. bijendra mishra
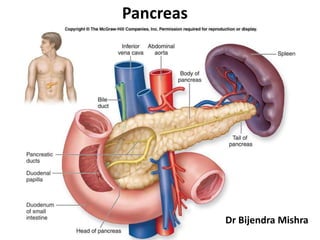
- 2. Surgical Anatomy • Also known as abdominal tiger. • Pan = All, kreas = Flesh. • Elongated retroperitoneal organ; 15-20 cm long; lies against L1-L2 vertebra. • It lies posterior to stomach, separated by lesser sac. • Parts Head lies in the concavity of duodenum and Tail reaches the hilum of spleen. Posterior surface of the neck is related to the terminal part of superior mesenteric vein and beginning of portal vein. • Ducts- Duct of Wirsung – main duct, begins at tail, joins the bile duct in the wall of second part od duodenum to form ampulla of vater and opens on the summit of major duodenal papilla (8-10cm from pylorus). Duct od Santorini – accessory duct, begins in the lower part of head and opens at the minor duodenal papilla(6-8cm from pylorus).
- 4. Acute pancreatitis • Acutenonbacterialinflammatoryconditioncausedby activation,interstitialliberationandauto-digestionof pancreaspresentingas acuteabdominalpain. • Stings like a scorpion (severe pain) • Drinks like a fish (dehydration) • Eats like a wolf (pancreatic necrosis) • Burrows like a rodent (produces fistula) • Kills like a leopard (life-threatening)
- 5. Mechanism
- 6. 6 Pathophysiology • Co-localization theory “Steer & Saluja” 1998 – Most acceptable – Stones pancreatic duct hypertension ductal rupture – Ductal pH = 9 …… parenchymal pH = 7 – trypsinogen + cathepsin B trypsin autodigestion cascade
- 7. Pathogenesis
- 8. 8 Diagnosis “Acute pancreatitis is a diagnosis of exclusion” Schwartz’s • History: – Epigastric pain – Radiating to back – Nausea, vomiting – Precipitating factor? • Physical – V/S variable – Epigastric tenderness – Cullen’s / Grey Turner’s (1%) – Findings of complication(s)
- 9. 9 Diagnosis
- 10. 10 Cullen’s sign bluish discoloration around umbilicus
- 11. 11 Grey Turner’s sign bluish discoloration in flanks
- 12. 12 Diagnosis Serum markers Amylase • Easiest to measure and most widely used • Rises immediately • Peaks in few hours • Remains for 3-5 days • “Three fold rise is diagnostic” • May be normal in severe attacks • May be falsely negative in hyperlipedimic patients • Inverse correlation between severity and serum amylase level • No need to repeat Urine amylase • Remains elevated for a few more days • Increase excretion of amylase with attacks of AP • Of great value when dealing with severe pancreatitis
- 13. 13
- 14. 14 Radiology • Diagnostic role – X-ray – U/S – CE-CT
- 15. 15 Radiology • X-ray – Air in the duodenal C loop – Sentinel loop sign – Colon cutoff sign – All these signs are non specific
- 16. 16 Radiology • CE-CT – Enlargement of the pancreas • (focal/diffuse) – Irregular enhancement – Shaggy Pancreatic contour – Thickening of fascial planes – fluid collections. • Intraperitoneal / retroperitoneal – Retroperitoneal air
- 17. 17 Radiology • U/S – Diagnosis of gallstones – F/U of pseudocysts. – Dx pseudoaneurysms – EAUS vs. EUS
- 18. 18 Course – Mild = edematous pancreatitis – Severe = necrotic pancreatitis – Very severe = infected necrosis – No such thing as moderate pancreatitis
- 19. 19 Prognosis • Serum markers • CT • Systemic complications • Prognostic scores – Ranson – Apache II – Modified Glasgow – Atlanta
- 20. 20 Prognostic scores • Ranson’s – Published in 1974 – Predictor of morbidity/mortality • <2 0% mortality • 3-5 10-20% • >7 >50% mortality • Drawbacks of Ranson’s – 11 parameters – 48 hours – No predictor value beyond 48hrs – Too pessimistic for today’s healthcare system
- 21. 21
- 22. 22 Prognostic scores • APACHE II – Immediate – Acute and chronic parameters – Complicated – >7 = severe pancreatitis
- 23. 23 Prognostic biochemical markers • Biochemical markers of prognosis – Ideally • High sensitivity • High specificity • Discriminate severe from mild • Immediate • Widely available – Amylase & lipase • Highly sens./spec. • Lack prognostic value
- 24. 24 Prognostic biochemical markers • Alternatives • CRP • 2 macroglobulin • PMN elastase • 1 antitrypsin • Phospholipase A2 – “CRP seems to be the marker of choice in these settings” – CRP >150 is diagnostic of severe pancreatitis
- 25. Management - ABCDEF • Aspiration with ryle’s tube • Blood transfusion • Charts- increasing pulse, temp indicates pancreatic abscess • Drugs- IV cefuroxime or imipenem or ciprofloxacin with metronidazole. Low molecular Dextran given to increase renal perfusion • Exploratory laparotomy only when diagnosis in doubt, patient is not improving, or when complications such as pancreatic abscess, fistula, necrosis is present. • Fluids given early. Rapid infusion of 2-3L of RL used to treat hypovolemic shock. Plasma or albumin may also be given.
- 27. Key notes
- 28. Complications
- 29. Chronic Pancreatitis • Diffuseinflammatoryprocessof pancreasinvolvinghead,body andtailresultingin permanent structuralandfunctional damage.
- 30. Causes • Alcohol • Idiopathic- due to malnutrition, a.k.a tropical pancreatitis • Hereditary- transmitted as a mendelian- dominant trait • Cystic fibrosis • Hyperparathyroidism • Autoimmune pancreatitis
- 31. Pathology
- 32. Clinical features • Malabsorption • Obstructive jaundice • Pain abdomen- due to multiple strictures in the pancreatic duct increasing the intraductal pressure. Relieved on stooping forward. • Exploratory laparotomy- diagnosed at laparotomy done for obstructive jaundice. • Diabetes
- 33. Investigations • Plain X-ray • USG • ERCP (chain of lakes) • CT Scan
- 34. Complications • Obstructive jaundice due to a mass lesion in the head region • Carcinoma pancreas • Pseudocyst • Steroids in autoimmune pancreatitis
- 35. Treatment • Analgesics., epidural analgesia, slow release opioid skin patches. • Supplement pancreatic enzymes, diet should be low in fat and vitamin D supplements given. • Surgery- Distal Pancreatectomy (tail involvement) Puestow’s operation (longitudinal pancreaticojejunostomy) Pancreaticoduodenectomy (head involvement) choledochojejunostomy (bile duct obstruction) Hans beger’s procedure- duodenum preserving pancreatic head resection.
- 36. Pseudocyst • Collectionof amylaserichfluidin thelessersac,dueto pancreaticpathology. • Fluid collection in the first 4 weeks is acute fluid collection, after 4 weeks it becomes acute Pseudocyst. • It is called Pseudocyst because it has no epithelial lining. • Fluid is enclosed by a wall of fibrous granulation tissue and is called Pseudocyst.
- 37. sagittal-sectional view of lesser sac
- 38. cross-sectional view of lesser sac
- 39. Aetiology • Following an attack of Acute pancreatitis • Blunt injury causing ductal disruption • Chronic pancreatitis Location- b/w stomach and transverse colon b/w stomach and liver Behind or below transverse colon
- 40. D’EGIDIO Classification • Type 1- after an episode of acute pancreatitis and is associated with normal duct anatomy and rarely communicate with pancreatic duct. • Type 2- after an episode of acute on chronic pancreatitis and have a diseased but not strictured ducts, and there is after communication between duct and Pseudocyst • Type 3- retention cyst, occurs in chronic pancreatitis, uniformly associated with duct stricture and a communication between duct and Pseudocyst.
- 41. Clinical features • Tensely cystic mass feels firm on palpation. • Classically upper border of the mass is not felt. • It is retroperitoneal so does not move with respiration. • May have transverse mobility • It does not fall forward • Resonant note on percussion because of stomach or intestine anterior to it • Transmitted pulsation from aorta can be felt • Baid sign- if ryle’s tube is passed, it is felt above the swelling. • Depending upon the tension within the cyst, it can be tender or non tender
- 42. Investigations • USG/CT- confirm that there is no neoplasm before doing cystogastrostomy. • ERCP- shows communication between duct and cyst
- 43. Treatment • Majority of the cysts following acute pancreatitis resolve spontaneously within 4 weeks, hence regular USG is required. • Increased size, pain, unresolved needs surgery. • Cystogastrostomy is done for cyst arising from head and body of pancreas. Done after 6 weeks because that’s the time required for the wall to become fibrous. Size of the cyst should be at least 6cm, and stoma size should be about 6cm. For reasons not known, the food does not enter the cyst. This procedure can also be done by endoscopic method. • Distal pancreatectomy done for cyst arising from tail of pancreas • Cystojejunostomy done for large cysts.
- 44. Cystogastrostomy
- 45. Insulinoma • Isletcelltumour,involvingtailandbody. • Majority are benign, 1/3rd are malignant and 1/3rd are multiple. • Hypoglycaemia is seen-> hunger pain, mimicking duodenal ulcer • Dizziness, syncopal attack, blurring of vision, epilepsy and coma are later symptoms. • Whipple’s triad of insulinoma- attack of hypoglycaemia in morning hours, relieved on taking glucose and blood sugar in fasting state below 45mg%
- 46. Investigation • Serum insulin • Persistent hypoglycaemia (<50%) • USG- if mass >2cm • Selective angiography- tumour blush
- 47. Treatment • Enucleation is treatment of choice • Resection of the tumour and distal pancreatectomy • Diazoxide given to supress insulin release • Streptozocin is best chemotherapeutic agent for inoperable insulinoma
- 48. Treatment • Duodenoduodenostomy is the treatment of choice. • Duodenojejunostomy can be done otherwise.
- 49. Annular pancreas • Rare anomaly which occurs due to persistence of the ventral pancreatic anlage which fails to rotate. • As a result of this, second part of the duodenum is surrounded by a thin rim of pancreatic tissue. • Associated anomalies- intrinsic duodenal atresia or stenosis
- 50. Embryology • The pancreas develops from one dorsal and two ventral buds. Due to selective expansion of the duodenum, by approximately the seventh week, the ventral bud rotates with the gut, passing behind the duodenum from the right to left and eventually fusing with the dorsal bud. • The ventral bud forms the inferior part of the head of the pancreas and the uncinate process, whereas the dorsal bud becomes the tail and the body. • Fusion of the ductular network of the two buds gives rise to the main pancreatic duct. The accessory pancreatic duct, which often persists, is derived from the dorsal pancreatic duct proximal to the site of fusion • Annular pancreas results from failure of the ventral bud to rotate with the duodenum, causing envelopment of duodenum.
- 51. Clinical features • Neonatal type- early in life. Produces symptoms of acute intestinal obstruction with vomiting and inability to take food. • Adult type- after age 20. vomiting is bile stained. Due to stasis in the antrum, features of duodenal ulcer may present. • Investigation Xray- double bubble sign, due to dilated stomach and dilated proximal duodenum Barium meal- obstruction to 2nd part of duodenum seen.
- 53. Carcinoma pancreas • 70 % occur in head including periampullary region • 70% are Adenocarcinoma of duct cell origin. • Rate of death in male due to cancer:- Lung>Colon>Prostate>Pancreas Periampullary refers to carcinoma arising from ampulla of vater, the duodenal mucosa or the lower end of common bile duct
- 54. Aetiology • Chronic tropical pancreatitis • Hemochromatosis • Diabetes • Alcohol and smoking • Westernization of diet- fatty food, animal proteins • Industrial carcinogens- benzidine, gasoline
- 55. Types- Microscopically • Mucus • Non mucus • Anaplastic • Cyst adenocarcinomas
- 56. Clinical features • Obstructive jaundice – involving head of pancreas or periampullary • Backache (L1-L2) - retroperitoneal, so neural spread is fast • Weight loss • Severe pain • Vomiting- duodenal obstruction • Trousseau’s sign (Thrombophlebitis migrans)- due to sluggish blood flow resulting in thrombus formation, affects long saphenous vein commonly.
- 57. Investigation • USG- Rules out calculus obstruction Detects mass as small as 2cm • CECT • ERCP • Carbohydrate antigen CA19-9
- 58. Treatment • Whipple’s operation for periampullary ca. • Total pancreatectomy with involved lymph nodes if the tumour is very small and diagnosed early. • Many cases are diagnosed late. They are inoperable either due to fixity to portal vein or due to mets. Only palliative treatment is given. Palliative radiotherapy- 4000-6000 cGy units given