
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Tenon capsule ,Sclera and limbus : subash
Similar to Tenon capsule ,Sclera and limbus : subash (20)
Recently uploaded
Recently uploaded (20)
Tenon capsule ,Sclera and limbus : subash
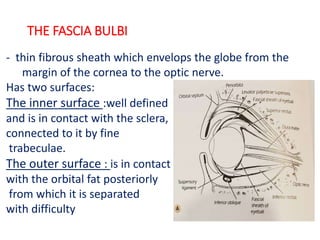
- 1. THE FASCIA BULBI - thin fibrous sheath which envelops the globe from the margin of the cornea to the optic nerve. Has two surfaces: The inner surface :well defined and is in contact with the sclera, connected to it by fine trabeculae. The outer surface : is in contact with the orbital fat posteriorly from which it is separated with difficulty
- 2. • Anteriorly : firmly attached to sclera about 1.5mm posterior to corneoscleral junction • Posteriorly : fuses with the meninges around the optic nerve and with the sclera around the exit of optic nerve • Inferiorly: thickened to form a sling or hammock which supports the globe as the suspensory ligament of Lockwood where it is pierced by the tendons of extra ocular muscles.
- 3. MAIN FUNCTION •To position and support the globe within the orbital cavity •To permit the actions of extrinsic muscles to produce movement of eyeball.
- 4. APPLIED ANATOMY OF FASCIA BULBI •During enucleation of the eyeball the fascial sheath should be preserved to serve as a socket for the prosthesis •Close relationship exists between the suspensory ligament of lockwood and the inferior rectus and the inferior oblique muscle making operations on these muscles very difficult.
- 5. CONTD… •Even after extensive removal of maxilla, eyeball does not sag down because the suspensory ligament is strong enough to provide the eyeball with adequate support from below. •Extension of the fascial sheath through the orbital fat to the bony walls of orbital cavity assists the orbital septum in preventing herniation of fat into the lids.
- 6. EMBRYOLOGY OF SCLERA •The human sclera differentiates from neural crest and mesoderm7 week •The majority of the sclera differentiates from neural crest that surrounds the optic cup of Neuroectoderm • a small temporal portion of the sclera differentiates from mesoderm
- 7. SCLERA •Forms Posterior five-sixth part of eyeball •normally white in adults •visible anterior Portion: white of the eye.
- 8. •consists almost entirely of the collagen( chiefly with type 1 and moderately with type 3) within a lesser amount of the ground substance and scanty fibrocytes. •Viscoelastic •relatively avascular •thicker in males than in females
- 9. •Scleral collagen fibrils are highly variable in their diameter, •lamellae vary in thickness, irregular with respect to neighbouring lamella •water content of the sclera 68%
- 10. DIMENSIONS •roughly spherical. •Coronal diameter: 22-24mm •Antero-posterior diameter: 16-17mm at birth : 22.5mm at 3yrs • Attains the adult size 22-24mm by the age of 13yrs
- 11. THICKNESS
- 12. SPECIAL REGION OF SCLERA •Both the internal and external aspects of sclera at the sclerocorneal junction project more anteriorly than the main body of sclera- concave cirumferential groove - Internal scleral sulcus(occupied by trabecular meshwork) •Just posterior to the limbus and lying within the sclera is circular running canal called the canal of schlemn.
- 13. SCLERAL SPUR •Circular flang of the anterior most part of sclera lies deep to Schlemm’s canal •Meridional fibres of ciliary muscle attached to SS.
- 14. LAMINA CRIBOSA • thin, sieve-like portion of sclera at the base of the optic disc through which optic nerve passes. •Concave at intraocular aspect •Holes in the network remain relatively aligned with each other providing unobstructed passage for bundle of nerve fibers
- 15. MICROSCOPIC STRUCTURE 1. Episcleral tissue 2. Scleral proper 3. Lamina fusca
- 16. INSERTION • The medial rectus: 5.5mm • The inferior rectus: 6.5mm • The lateral rectus: 6.9mm • The superior rectus: 7.7mm • The insertion of the superior and the inferior oblique are posterior to the scleral equator.
- 17. APERTURES •Sclera is pierced by two potential openings •Anterior scleral foramen: where sclera meets and anatomically converges with cornea •Posterior scleral foramen: Provides an exit for the optic nerve
- 18. EMISSERIA Channels through which vessels and nerves pass through the sclera. •Anterior emissaria •Middle emissaria: •Posterior emissaria:
- 19. BLOOD SUPPLY •Anteriorly by the anterior cilliary artery. •Posteriorly by short ciliary artery •Episcleral plexus •Underlying choroid
- 20. NERVE SUPPLY Anterior portion : two long ciliary nerves Posterior portion: many short ciliary nerves
- 21. APPLIED ANATOMY •Profuse sensory innervation of sclera results in dull aching pain associated with inflammations of sclera. The pain is worse during ocular movement •Emissaria provides pathway for extraocular spread of intraocular tumors. Most common site for extension is along optic nerve
- 22. CONT… •Scleral rupture following blunt trauma can occur at a number of sites: -in a circumferential arc parallel to the corneal limbus opposite the site of impact, -at the insertion of rectus muscles or at the equator of the globe. -The most common site is the superonasal quadrant near the limbus.
- 23. CONT… •As the scleral is thin the strabismus and retinal detachment surgery require careful placement of the suture. •In infantile glaucoma, the viscid slow stretch in response to changes in IOP results in buphthalmic globe.
- 24. CONT.. •Progressive Myopia is characterized by scleral thinning and ocular elongation. Defects in scleral ECM remodeling lead to myopia •In glaucoma the raised IOP causes lamina cribrosa to bulge outwards – resultant cupping of disc in chronic glaucoma
- 25. CONT… change in colour of sclera with age and with disease •In elderly - yellowish colour •In jaundice - yellow discolouration •In osteogenesis imperfecta, Ehlers- Danlos syndrome, Pseudoxanthoma elasticum and other collagen diseases thin and blue
- 26. EPISCLERITIS •Immununologically mediated recurrent inflammation of the tissue that lies between the deep conjunctival stroma and superficial scleral lamellae •Presence of deep hyperemia is benign, short-lived not associated with tenderness, ciliary pain or flare and cell in the anterior chamber •Caused by allergy to food, airborne allergen.
- 27. SCLERITIS • Immunologically mediated inflammation of the sclera • always associated with the secondary inflammation of the episclera • deep hyperemia, tenderness, ciliary pain, photophobia and flare and cells in the anterior chamber • Causes: auto-immune collagen vascular disease like SLE, Scleroderma, granulomatous diseases like syphillis, tuberculosis, gout. • 50% is idiopathic
- 28. PIGMENTATIONS •Nerve loop of Axenfeld: branch of long ciliary nerve accompanying the anterior ciliary artery form a loop in the sclera; often carry some pigments producing blue black spot in superficial sclera.
- 29. OCULAR MELANOCYTOSIS •slate gray patches of scleral and episcleral pigmentations, usually associated with nevus of ota/oculodremal melanocytosis (ipsilateral hyperpigmentation of the iris, fundus and periocular skin).
- 30. STAPHYLOMA An ectasia of the outer coats(cornea, or sclera or both) of the eye with an incarceration of the uveal tissue.
- 31. THE LIMBAL TRANSITION ZONE • Junctional zone between the cornea and sclera. • 1.5mm wide in horizontal plane and 2mm wide in vertical plane • Internal edge; corneal limbus • External edge; scleral limbus
- 32. • Scleral limbus Defined by a line perpendicular to the surface passing through the scleral spur. • Corneal Limbus demonstrated by the line joining the termination of Bowman’s layer to the termination of Descemet’s membrane
- 33. AT THE LIMBUS • The corneal epithelium becomes continuous with the epithelium of bulbar conjunctiva • Bowman's membrane becomes continuous with the lamina propria of the conjunctiva and tenon's capsule. • Stroma becomes sclera • Descemet's membrane becomes schwalbe's line. • Endothelium lines the trabecular meshwork and becomes continuous with the anterior surface of the epithelium • Pallisades of Vogt :folds of epithelial cells that run radially into the cornea
- 34. THE ANATOMICAL LIMBUS •The anatomical limbus takes up an arc as it traverses the tissues in an anterior to posterior manner •Schwalbe’s line marks the posterior limit to the anatomical limbus.
- 35. SURGICAL LIMBUS •2mm wide circumcorneal transition zone between the clear cornea and opaque sclera
- 37. THE CATARACT INCISION & THE SURGICAL LIMBUS •Anterior limbal incision - At blue limbal zone -traverses Descemet’s membrane,may cause stripping •Clear corneal incision - infront of the anterior limbal line -chances of induced astigmatism and Descemet’s membrane stripping
- 38. •Scleral incision - posterior to the posterior Limbal border -excessive bleeding and hyphaema •Posterior limbal incision -at white limbal zone -injures trabecular meshwork •Mid-limbal incision -at mid limbal line -corresponds to schwalbe’s line -safest
- 39. REFERENCES • Anthony J Bron, Ramesh C Tripathi, Brenda J Tripathi, Wolff’s Anatomy of the eye and orbit, 8th edition • External Disease and Cornea,Basic and Clinical Science Course, American Academy Of Ophthalmology • Practical Ophtahlmology, A Manual For Beginning Residents, American Academy of Ophthalmology • Snell, Richard s. and Michael A. lemp, Clinical Anatomy of the eye,2nd Edition, India:Blackwell science,1998. • Jack J kanski, Brad Bowling, Clinical Ophthalmology, 7th edition • A.K. Khurana Anatomy and Physiology of eye ( third edition) • Internet Resources: www.oculist.com : www.eophtha .com
Editor's Notes
- EOM have fascial sleeves that are continuous with the sheath of the eyeball, so the socket moves when the muscles contracts
- Human beings are the only primates with white sclera The term sclera is derived from Greek word scleros meaning "hard". opaque, fibrous and protective outer layer of eyeball
- Protects the intraocular contents from injury and displacement, contains the intraocular pressure and prevents deformation of the eyeball. This white appearance is because of the scattering of all wavelengths of light by dense irregular bundles of collagen in sclera Often described as viscoelastic as it exhibits biphasic response when suddenly deformed, elasticrapid but bried lengthening,, viscid slow streching
- Lamellar organization of the human sclera. Scleral fibroblasts (F) can be seen between irregularly arranged collagenous lamella (L). Within each lamella, collagen fibrils are oriented in the same general direction, with some running longitudinally in the plane of section (arrow), and some running perpendicular to the plane of section and seen in cross section (asterisk). The black bar indicates the width of a lamella
- Thickest : 1mm near the optic nerve Thinnest : 0.3mm at the insertion of the recti At equator : 0.6mm From the recti muscles insertions towards limbus there is gradual increase in thickness up to 0.8mm
- Schwalbe's line is the anatomical line found on the interior surface of the eye's cornea, and delineates the outer limit of the corneal endothelium layer. Specifically, it represents the termination of Descemet's membrane.[1] In many cases it can be seen via gonioscopy.
- maintain the pressure gradient between the inside of the eye and the surrounding tissue. Increase in posterior curvature producing glaucomatous cupping disc
- Epi thin,dense vascularized layer of connective tissue. Ant: continuous with tenon’s capsule. Capillary network in ant part of episcera Ciliary flush. Umyelinated nerve fibre, keratocyte, melanocytes.ant: ant ciliary artery post: post ciliary artery Sp:avascular, type I collagen crossing each other in all directionopaque.increasing age increased lipids deposit and sclera becomes yellow LF: Lamina fusca is the innermost layer of sclera. It is characterised by abundance of pigmented cells or melanocytes, mostly migrated from choroid. The connective tissue of this layer is loosely arranged than rest of the sclera. Lamina fusca is separated from choroid by a thin potential space known as suprachoroidal or perichoroidal space.
- All 4 rectus muscle are inserted in sclera at different distance from limbus
- >Ant ciliary arteries-2 in number except in lateral rectus (1 in number) >the largest branch of this vessel also enters the ciliary body to form major arterial aracade >for 1 ant ciliary artery - 2 ciliary veins in the ciliary body and is accompanied by 1 post. Ciliary nerve. (nerve loop of axenfeld) The vortex veins pierce sclera 4 mm posterior to the equator
- Choroidal capillaries are fenestrated and the sclera doesn’t present a major barrier to the diffusion of even a larger molecules like albumin to choroid. Hence, subtenon or subconjunctivally injected drugs can reach the internal tunics of eyeball.
- The termination of Bowman’s layer is indicated on the biomicroscopy by the internal limit of the marginal arcade of the corneal vessels. The termination of Descemet’s membrane is visible on gonioscopy as the most anterior landmark of the drainage angle, Schwalbe’s line ( hypertrophied in the anterior embryotoxon when it is visible as a fine internal ridge.
- Three landmarks Anterior limbal border: overlies the termination of Bowman’s layer. Mid limbal line: overlies the termination of Descemet’s membrane. Posterior limbal border: overlies the scleral spur