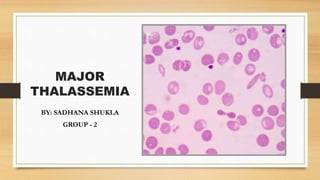
2. INTRODUCTION
•Thalassemias are hereditary hemoglobin (Hb) disorders of α-
or β-globin genes.
Defects in these genes lead to abnormal hemoglobin and RBC
structure and function.
•Presents as microcytic hypochromic anemia
Mild cases can be asymptomatic.
6. What Is Alpha Thalassemia?
• Patients have a decrease in α chain production,
leading to a decrease in hemoglobin.
• The problem in alpha thalassemia is deletion of one
or more genes (unlike beta thalassemia, in which the
problem is mutation of genes).
• The α globin gene actually has four alleles, two on
each chromosome 16.
• 4 types of disease variations:
• Minima: deletion of 1 α gene
• Minor: deletion of 2 α genes (same chromosome
= cis, opposite chromosomes = trans)
• HbH disease: deletion of 3 α genes
• Hb Barts: deletion of 4 α genes
7. alpha thalassemia major
• Deletion of four α chain genes is usually incompatible with life.
• Fetuses with this genotype have an extremely severe anemia (since they cannot
produce α chains at all).
• In the fetus, the tetramers consist of γ chains, and they are called Hb Barts.
• Red cells containing these tetramers have a shorter lifespan than normal red cells for a
couple reasons: they are more fragile (they can burst open, or hemolyze, when
squeezing through tiny spaces) and they are more likely to be removed from the
circulation by splenic macrophages.
• The heart attempts to compensate by beating faster and more forcefully—but
eventually it fails, and the fetus develops severe, diffuse edema (a condition known
as hydrops fetalis).
8. Clinical
Features
Silent carrier: asymptomatic
Alpha thalassemia trait: : mild hemolytic anemia with
normal BC and RDW
Hemoglobin H disease
oJaundice and anemia at birth
o Chronic hemolytic anemia that may require transfusions -
secondary iron overload due to hemolysis, transfusion, or
hemochromatosis
o Hepatosplenomegaly
oSkeletal deformities (less common)
oCompared to thalassemia beta, symptoms in adults are
generally less severe.
• Hb-Bart's hydrops fetalis syndrome (most severe variant
of alpha thalassemia)
o• Intrauterine ascites and hydrops fetalis, severe
hepatosplenomegaly, and often cardiac and skeletal
anomalies
o• Incompatible with life (death in utero or shortly after
birth)
9. What is beta thalassemia?
• Patients have a decrease in β chain production, leading to a decrease in hemoglobin
production.
• The problem in beta thalassemia is mutation of one or more genes (unlike alpha
thalassemia, in which the problem is deletion of genes).
• The beta chain gene has two alleles, one on each chromosome 11.
• 2 types of disease variations:
• Thalassemia minor: heterozygous, approximately 50% decreased synthesis
• Thalassemia major: homozygous, no production of β globulin, increase in
HbA₂(α₂δ₂) and HbF(α₂γ₂), no HbA
•
10. Beta thalassemia major
OR
Cooley’s Anemia
• •Significantly reduced or no production
of β-globin causes a life threat :
• •Poor oxygen –carrying capacity of
RBCs :faliure to thrive , poor brain
development.
• I. Increased alpha globin production
and pricepitation
• II. Increased splenic destructon of
dysfuctional RBC’S.
• III. Hyperplastic bone marrow
• IV. increased in
extramedully eyrthropoisis
11. Clinical
Presentation
• severe anemia (approximately 6 months of
age)
• Jaundice
• Hepatoslenomagaly , which is massive.
• Bone marrow expansion
• Frontal bossing (hydrocephalous in children )
• Chipmunk facies
• Fragility fractures
• Depression of bridge of nose and exposure
of upper central teeth.
• Skull shows hair on end apperance due to
widening of diploic spaces.
• Generalised skeleton osteoporosis.
• Growth retardation
• delayed puberty, primary amenorrhea in
females
• Leg ulcers
• Skin bronzing
• transfusion dependent: leads to iron overload
12. Diagnosis
• Take a full medical and family history (screen in high-risk areas).
• Order CBC with erythrocyte indices and peripheral blood smear.
• On CBC:
• Hb → usually < 11 g/dL or < 6 g/dL in Cooley’s anemia
• MCV → microcytic (< 70 fL) in thalassemias
• MCH → low in thalassemias
• Red-cell distribution width → not very useful in thalassemias
(can be normal or elevated)
• On peripheral blood smear:
• Target cells (most common)
• Howell-Jolly body: blue spot in RBC (DNA remnant)
• Anisocytosis: RBCs of unequal size
• Inclusion bodies: seen only in hemoglobin H (HbH)
disease (4 β aggregation)
• Heinz bodies: red spot at the periphery
of RBCs (denatured Hb)
• Basophilic stippling
13.
14. β-thalassemia α-thalassemia:
• Major:
• No HbA
• ↑ HbF (90%)
• ↑ HbA₂ (10%)
Minor:
↓ HbA (93%)
↑ HbA₂ (5%)
↑ HbF (2%)
Hb Barts: γ-tetrad (Hb electrophoresis will show
only a γ band).
Minima: normal percentage of HbA and HbA2
Minor (trait): normal percentage of HbA and
HbA2, but CBC shows anemia
HbH disease: β-tetrad
(i.e., Hb electrophoresis will show only a β band)
• If iron studies are normal, order Hb electrophoresis.
•Normal Hb electrophoresis studies show:
•HbA: 95%
•HbA2: 3%–5%
•HbF: minimal amount
•No HbH or Hb Barts with normal Hb electrophoresis
Confirmatory studies
15. MANAGEMENT Transfusions:
• Patients are transfusion dependent.
• Target Hb level > 10 g/dL
• Iron chelation:
• Reduces serum iron levels
• Deferoxamine (IV)
• Deferiprone/deferasirox (oral formulations)
• Folate supplementation, if not transfused
• Splenectomy and cholecystectomy:
• Splenectomies reduce transfusion requirements.
• Post-splenectomy vaccinations
(encapsulated organisms)
• Pneumococcal polyvalent
• Cholecystectomy to prevent recurrent gallstones
• Definitive therapy: allogeneic stem cell transplantation
• Genetic counseling