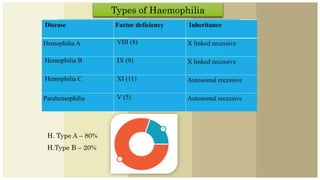
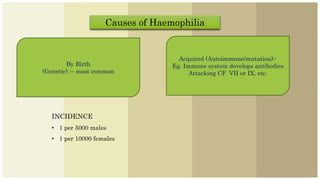
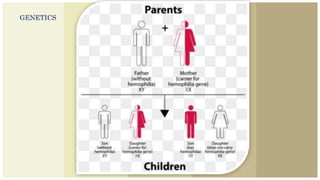
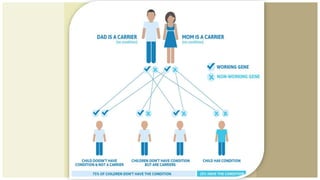
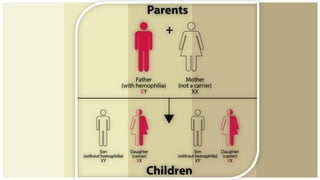
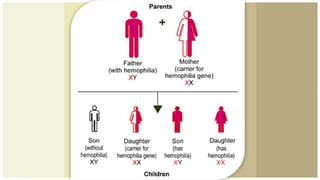
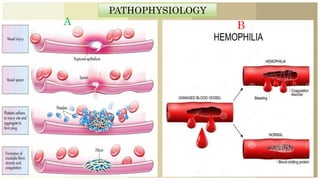
Haemophilia is an X-linked recessive bleeding disorder primarily affecting males, often referred to as 'royal's disease' due to its historical prevalence in European royal families. The condition results from a hereditary deficiency of clotting factors, leading to prolonged bleeding, with severe cases causing spontaneous bleeding in joints and muscles. Management includes prevention strategies, replacement therapy, gene therapy, and treatment to control bleeding episodes.





































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




