2002 Multimodal strategies to improve surgical outcome
UROP Poster
1. Predictors of 30-Day Readmission in Gynecologic Oncology
Sahar Gowani; Shitanshu Uppal, MD
Background:
The Centers for Medicare and Medicaid Services (CMS)
plans to include surgical procedures as it expands its
Readmission Penalty Program.
The Readmission Penalty Program requires CMS to
reduce payments to hospitals with exceptionally high
readmission rates
Hospital readmission is a persistent and costly
occurrence. A study of Medicare beneficiaries hospitalized
in 2009 reported a 30-day readmission rate of 12.7% for
surgical patients and 16.1% for medical patients and
unplanned hospital readmissions were estimated to cost
Medicare $17.4 billion in 2004.
Objectives:
PRIMARY OBJECTIVE: Identify predictors of 30-day
readmission for patients undergoing surgery for
gynecologic malignancies
SECONDARY OBJECTIVE: Establish a readmission
prediction scoring system with information available at the
time of discharge to categorize risk of readmission
Results:
Overall readmission rate was 7.4% (339/4581 patients)
Variables found to be significant for predicting
readmission at the time of discharge on logistic regression
modeling were
• Occurrence of at least one complication prior
to discharge
• Wide spread cancer
• Non-laparoscopic surgery
Patients experiencing post-discharge complications were
20 times more likely to be readmitted
Exploratory analysis of post-discharge complications
revealed 124 (36.5%) of patients readmitted had developed
infectious complications
• 32 (9.4%) were admitted with septic shock
• 25 (7.3%) had thromboembolic complications
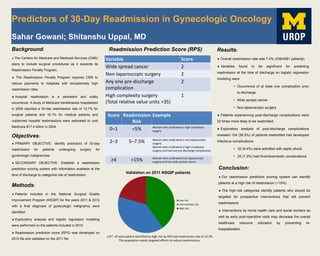
Readmission Prediction Score (RPS)
Methods:
Patients included in the National Surgical Quality
Improvement Program (NSQIP) for the years 2011 & 2012
with a final diagnosis of gynecologic malignancy were
identified.
Exploratory analysis and logistic regression modeling
were performed on the patients included in 2012
Readmission prediction score (RPS) was developed on
2012 file and validated on the 2011 file
Variable Score
Wide spread cancer 2
Non-laparoscopic surgery 2
Any one pre-discharge
complication
2
High complexity surgery
(Total relative value units >35)
1
Score Readmission
Risk
Example
0–1 <5% Woman who underwent a high complexity
surgery
2–3 5–7.5% Woman who underwent a non-laparoscopic
surgery
Woman who underwent a high complexity
surgery and had one pre-discharge complication
≥4 >15% Woman who underwent non-laparoscopic
surgery and has wide spread cancer
Validation on 2011 NSQIP patients
Low risk
Intermediate risk
High risk
1/5th of total patient identified as high risk by RPS had readmission rate of 14.5%
This population needs targeted efforts to reduce readmissions.
Conclusion:
Our readmission prediction scoring system can identify
patients at a high risk of readmission (~15%)
The high-risk categories identify patients who should be
targeted for prospective interventions that will prevent
readmissions
Interventions by home health care and social workers as
well as early post-operative visits may decrease the overall
healthcare resource utilization by preventing re-
hospitalization