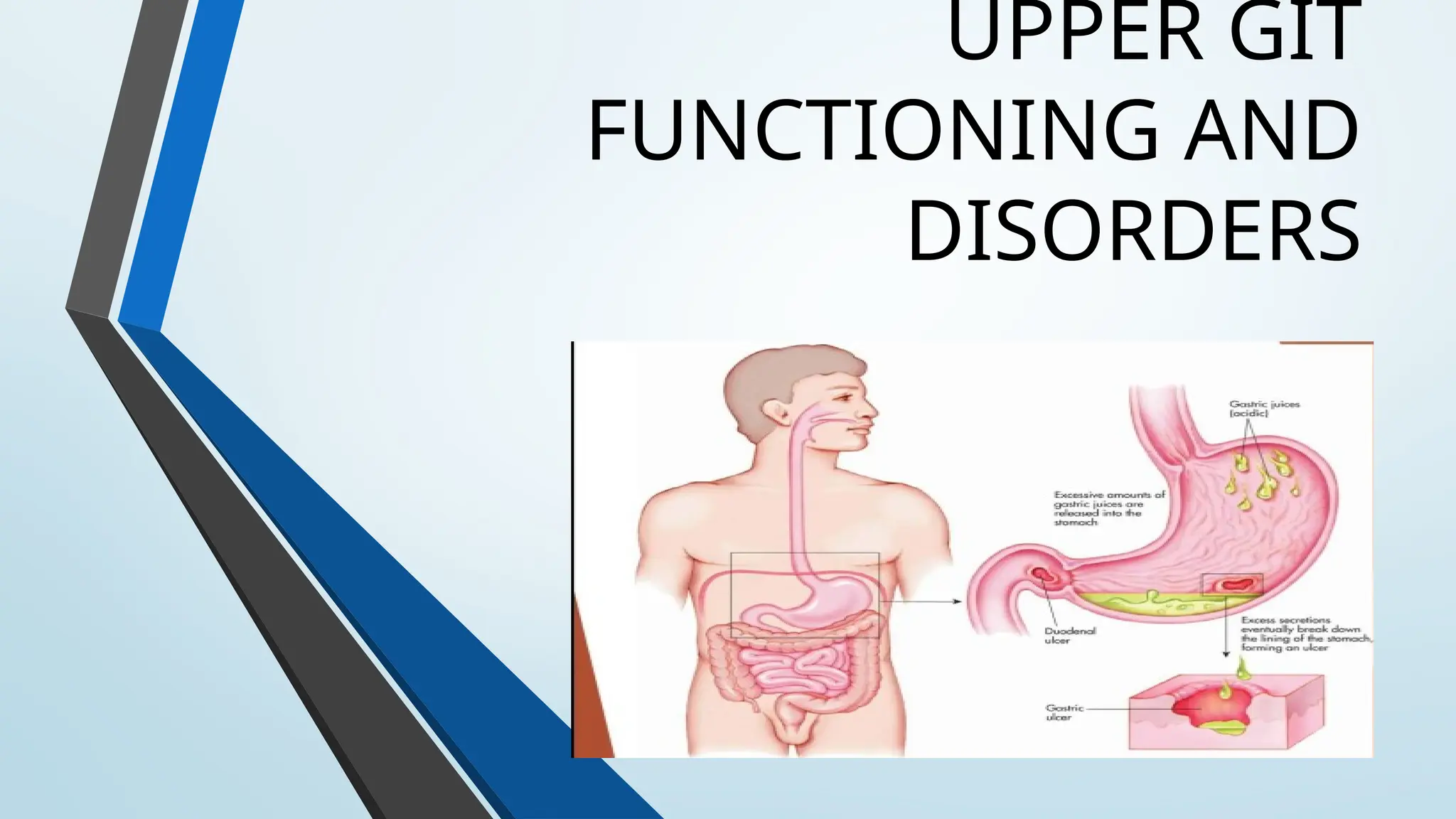
INTRODUCTION
The upper gastrointestinaltract consists of the esophagus, stomach, and
duodenum. The exact demarcation between upper and lower can vary. The
upper gastrointestinal tract includes the:
• Esophagus, the fibromuscular tube that food passes through—aided by
peristaltic contractions—the pharynx to the stomach.
• Stomach, which secretes protein -digesting enzymes called proteases
and strong acids to aid in food digestion, before sending the partially digested
food to the small intestines.
• Duodenum, the first section of the small intestine that may be the
principal site for iron absorption. [Kierszenbaum, A. L.].
4.
UPPER GIT DISORDERS
•The most common problem with the esophagus is GERD (gastroesophageal
reflux disease).
• Hiatal hernia
• Dysphagia
• Common digestive problems include heartburn/GERD, IBD, and IBS.
• Symptoms may include bloating, diarrhea, gas, stomach pain, and stomach
cramps.
• According to the U.S. National Library of Medicine (NLM), disorders of the
small intestine include bleeding, celiac disease, , intestinal cancer, intestinal
obstruction and blockage, ibs, ulcers, pain, and bacterial overgrowth.
5.
Disruption of thisbalance caused by too much acid (or weakened defense) can
result in erosions or ulcers with symptoms including upper abdominal pain,
indigestion or heartburn, nausea and/or vomiting.
In other patients, symptoms may result from problems with stomach emptying.
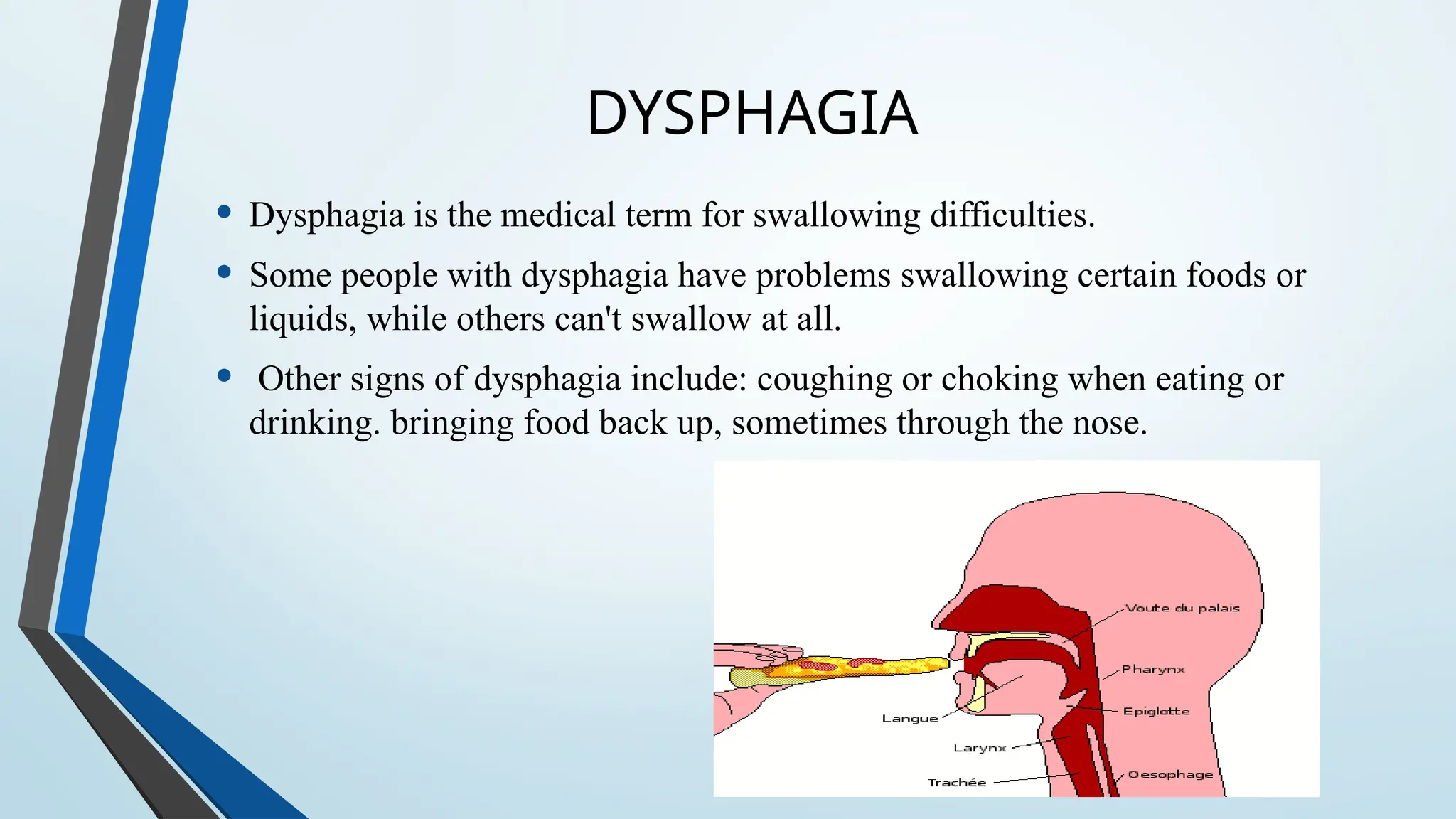
DYSPHAGIA
• Dysphagia isthe medical term for swallowing difficulties.
• Some people with dysphagia have problems swallowing certain foods or
liquids, while others can't swallow at all.
• Other signs of dysphagia include: coughing or choking when eating or
drinking. bringing food back up, sometimes through the nose.
8.
PREVALENCE
• Oropharyngeal dysphagiain the general population varies between 2.3% and
16%.7-12 These data are based on self-reported questionnaires and surveys.
• Dysphagia occurs more commonly in the ageing population and is frequently
because of accompaning medical problems. Prevalence data increased with
ageing up to 26.7% for participants above the age of 76.
SIGN AND SYMPTOMS
.Signs and symptoms associated with dysphagia may include:
•Having pain while swallowing (odynophagia)
•Having the sensation of food getting stuck in your throat or chest or behind your
breastbone (sternum)
•Drooling
•Being hoarse
•Bringing food back up (regurgitation)
•Having frequent heartburn
•Having food or stomach acid back up into your throat
•Unexpectedly losing weight
•Coughing or gagging when swallowing
•Having to cut food into smaller pieces or avoiding certain foods because of trouble
swallowing
11.
CAUSES
One of themost common problems is coughing or choking, when food goes
down the "wrong way" and blocks your airway. This can lead to chest
infections, such as aspiration pneumonia, which require urgent medical
treatment.
• Dysphagia may mean that you avoid eating and drinking due to a fear of
choking, which can lead to malnutrition and dehydration.
• Dysphagia can also affect your quality of life because it may prevent you
from enjoying meals and social occasions.
12.
ESOPHAGEAL DYSPHAGIA
Esophageal dysphagiarefers to the sensation of food sticking or getting hung
up in the base of your throat or in your chest after you've started to swallow.
Some of the causes of esophageal dysphagia .
• Aschalasia
• Diffuse spasm
• Oesophageal stricture
• Oesophageal tumors
• Esophageal ring
• GERD
• Eosinophilic esophagitis
[ Martino R, Foley N, Bhogal S, et al]
13.
OROPHARYNGEAL DYSPHAGIA
Certain conditionscan weaken your throat muscles, making it
difficult to move food from your mouth into your throat and
esophagus when you start to swallow.
• You may choke, gag or cough when you try to swallow or
have the sensation of food or fluids going down your
windpipe (trachea) or up your nose.
• This may lead to pneumonia.
Causes of oropharyngeal dysphagia include:
•Neurological disorders.
•Neurological damage.
•Pharyngoesophageal diverticulum (Zenker's diverticulum).
•Cancer.[ Miller RM, Chang MW]
GERD
Gastroesophageal reflux disease(GERD) is a common disease characterized by
reflux of stomach contents into the esophagus.[Vakil, et al, 2006]
PREVELENCE:
• GERD ranged from
18.1% to 27.8% in North America
8.8% to 25.9% in Europe
2.5% to 7.8% in East Asia
8.7% to 33.1% in the Middle East
11.6% in Australia
23.0% in South America.[El-Serag, et al, 2014]
17.
SYMPTOMS
• The symptomsof GERD are heartburn and regurgitation.[Nasrollah, et al,
2015]
GERD may have other symptoms, including
Mouth sours
chest pain or discomfort
epigastric pain
Nausea
bloating
throat pain or burning
sleep disturbances.
18.
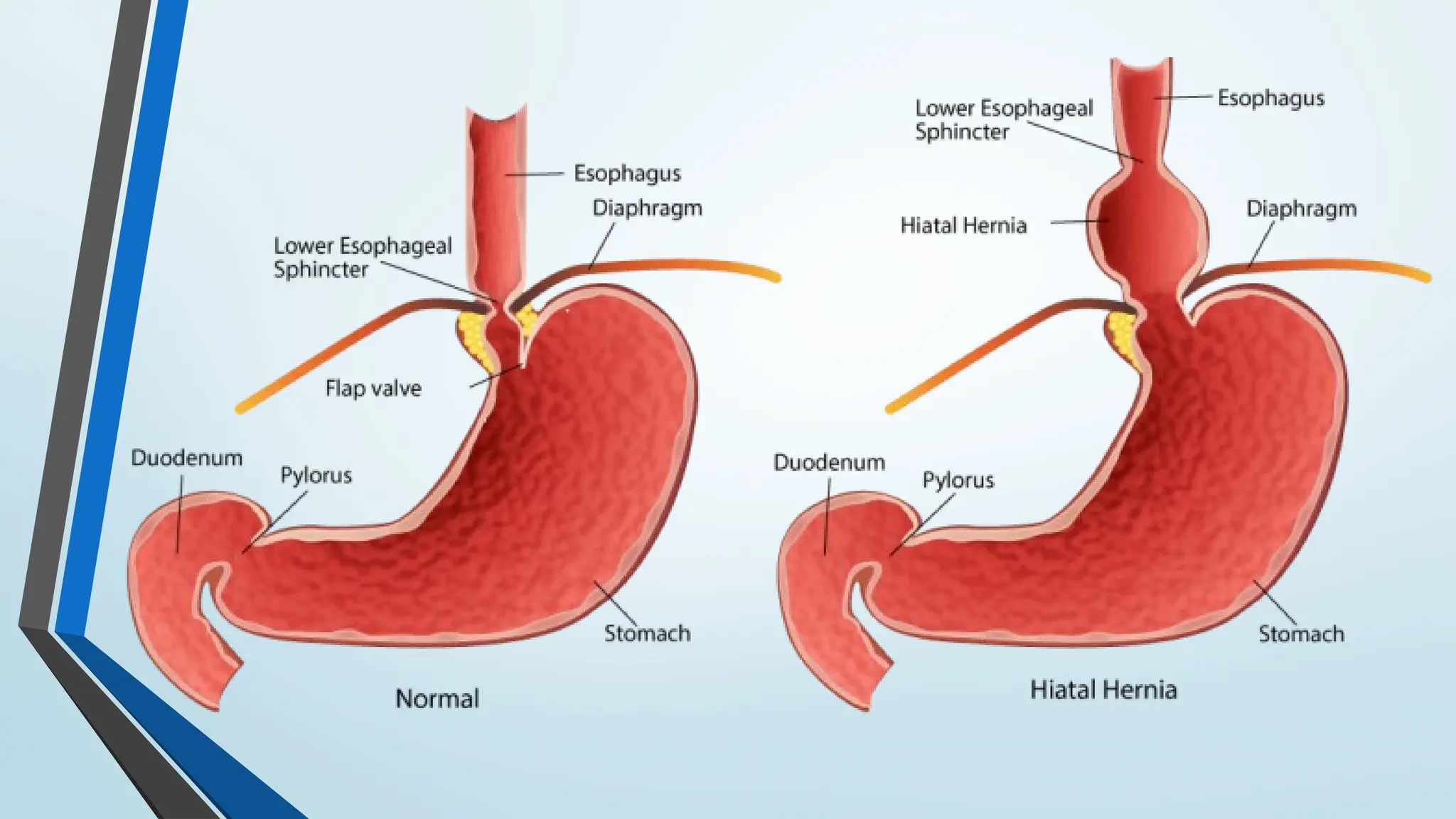
CAUSES
• Weakening orinappropriate relaxation of
lower esophageal sphincter
• overweight or obese because of increased
pressure on the abdomen
• Pregnant, due to the same increased pressure
• Associated with hiatal hernia (a condition in
which the upper portion of the stomach
protrudes above the diaphragm )[Dore, et al,
2008]
20.
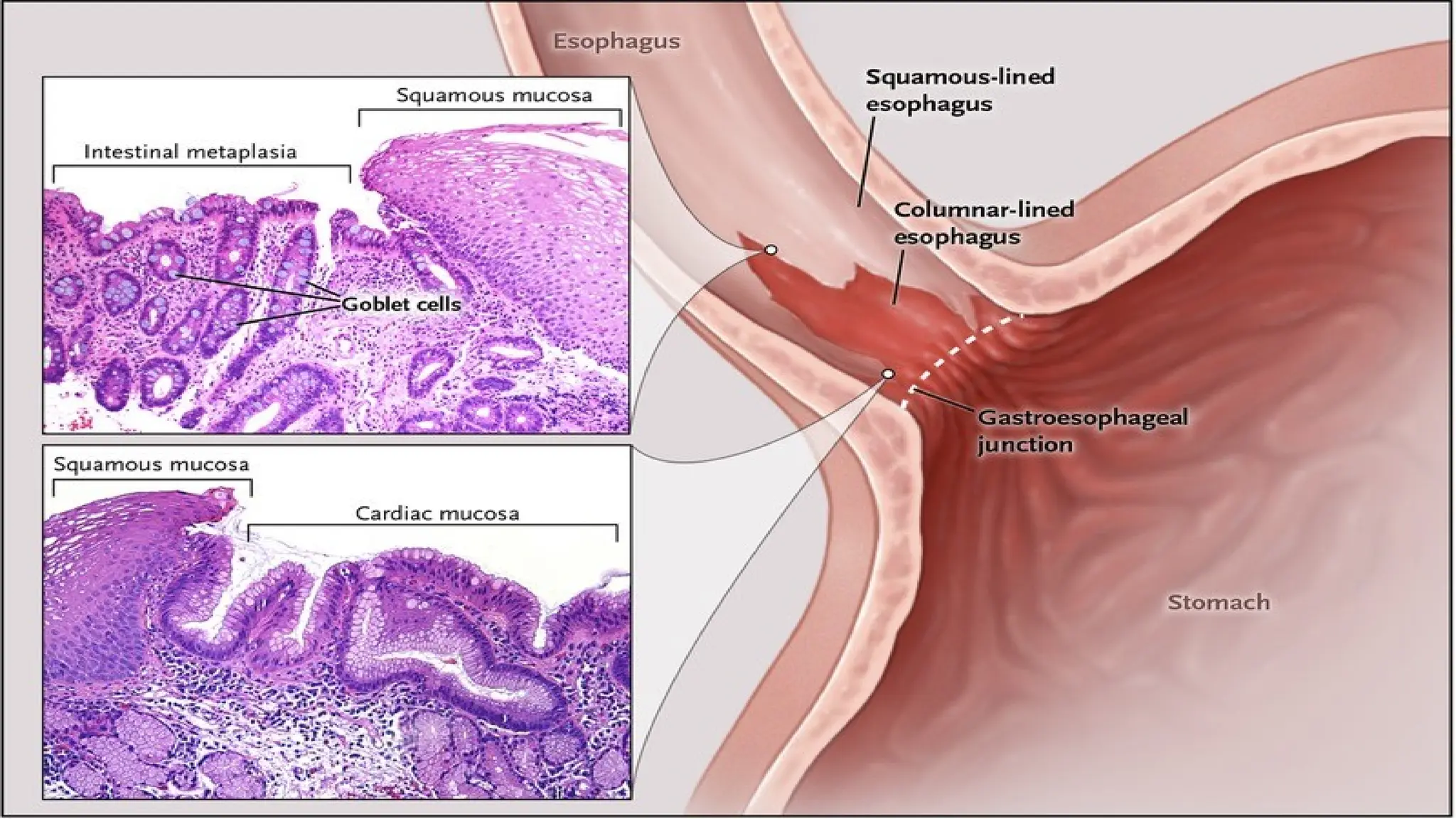
Complications
GERD can worsenand turn into other conditions
if left untreated.
These include:
Esophagitis: This is an inflammation of the
esophagus.
Esophageal stricture: In this condition, the
esophagus becomes narrow, making it difficult
to swallow.
Barrett's esophagus: The cells lining the
esophagus can change into cells similar to the
lining of the intestine. This can develop into
cancer.[Spechler, et al, 2011]
22.
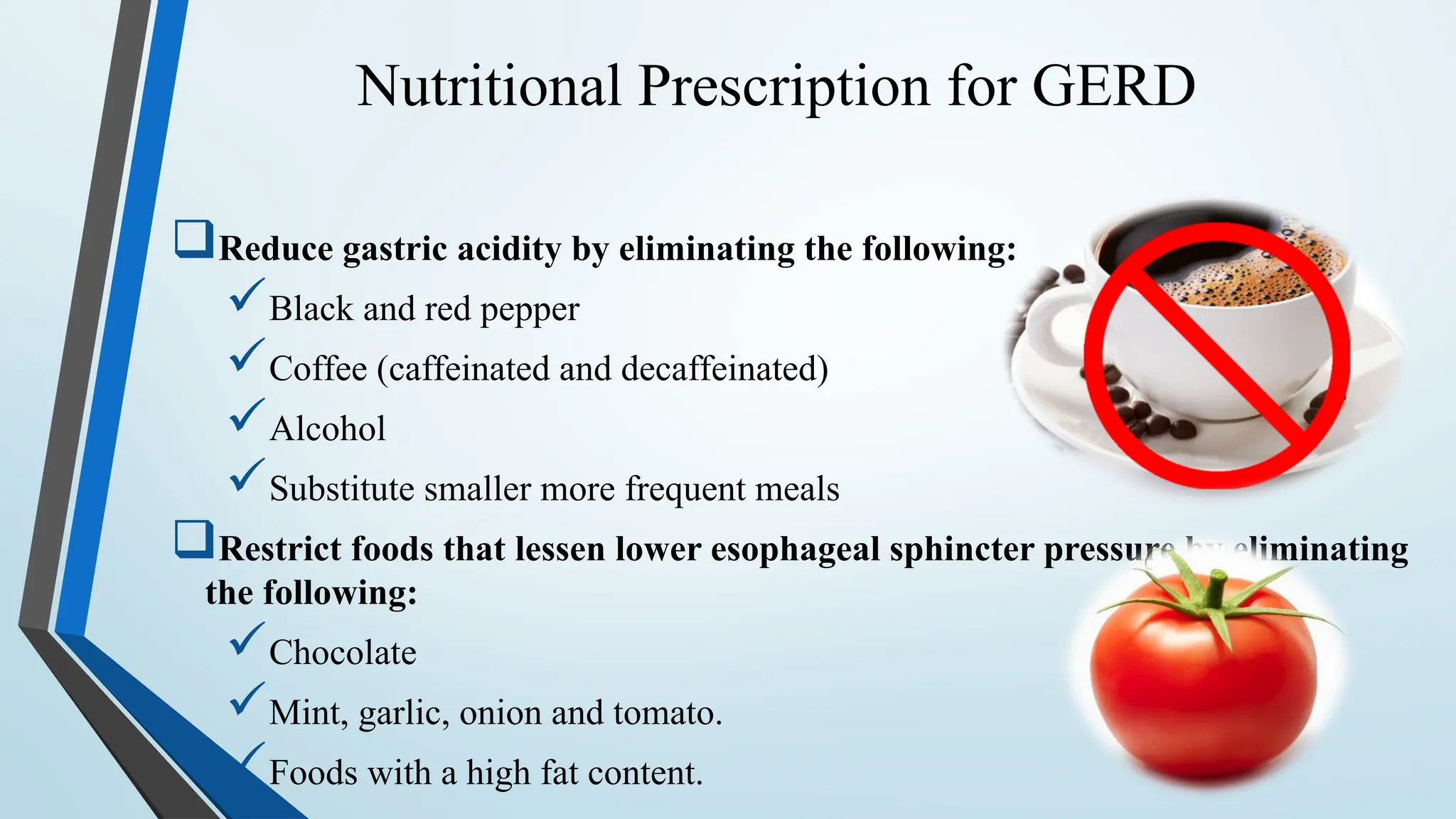
Nutritional Prescription forGERD
Reduce gastric acidity by eliminating the following:
Black and red pepper
Coffee (caffeinated and decaffeinated)
Alcohol
Substitute smaller more frequent meals
Restrict foods that lessen lower esophageal sphincter pressure by eliminating
the following:
Chocolate
Mint, garlic, onion and tomato.
Foods with a high fat content.
24.
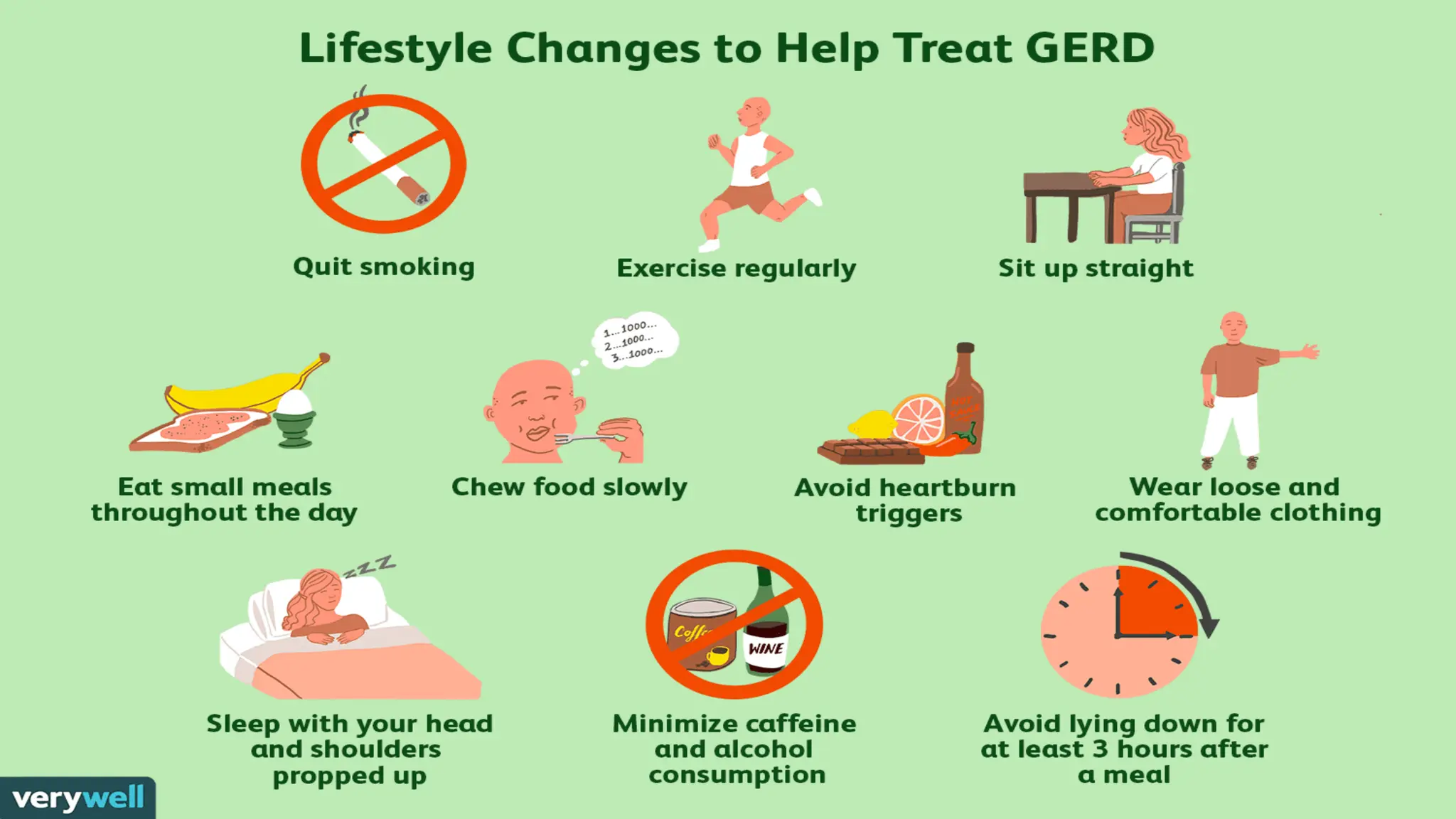
Treatment of GERD- lifestyle
modifications
Lifestyle changes: [Kaltenbach, et al, 2006]
Lifestyle and diet modification traditionally have included:
• Lose weight if needed because weight loss decreases intra-abdominal
pressure.
• Consume meals 2-3 hours before bedtime.
• Avoid eating bedtime snacks or lying down immediately after meals
Remain upright for 45 to 60 minutes after eating.
• Prop pillows under the head and upper torso during sleeping.
• Avoid wearing tight clothing that increases pressure in the stomach.
26.
CONT….
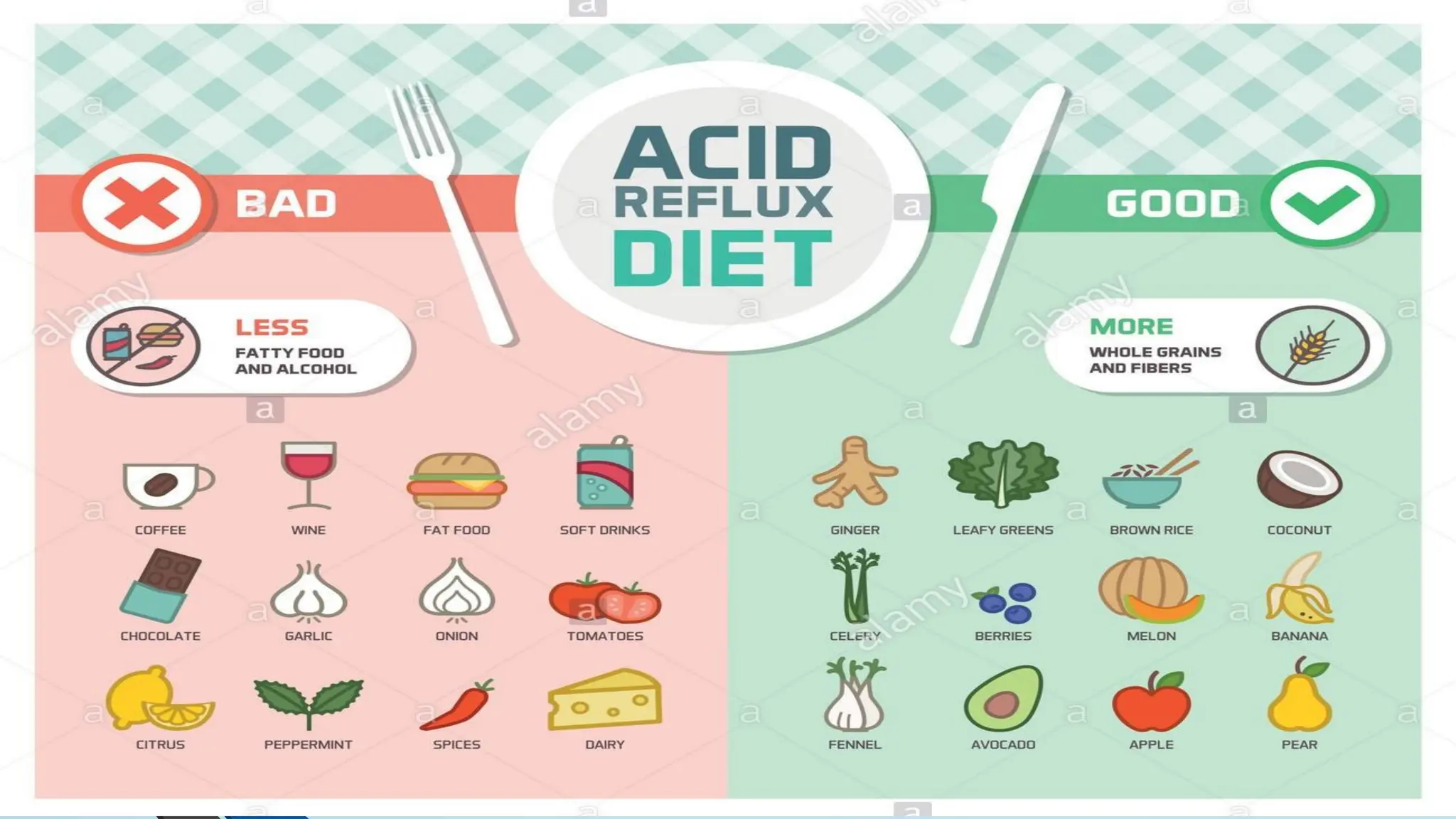
• During timesof esophagitis, avoid items that
may irritate the esophagus such as
carbonated beverages, citrus fruits and juices,
spicy foods, tomato products, and any other
individual intolerances.
• People who avoid citrus juices and tomato
products because of their acidity should be
encouraged to eat other sources of vitamin
C.
• Avoid use of non-steroidal anti inflammatory
drugs (NSAIDS)
Definition:
• Defined asa persistent or recurrent pain
or discomfort in the upper abdomen.
Also called Indigestion is often a sign of an underlying problem, such as gastro
esophageal reflux disease (GERD), ulcers, or gallbladder disease.
The term refers to a group of symptoms that often include bloating, discomfort, nausea,
and burping.
In the majority of cases, indigestion is linked to eating or drinking. It can also be caused
by infections or the use of certain medications.
Pathophysiology:
Indigestion may be caused by a disease, but it primarily occurs
because of stress or improper eating habits excessive smoking, exorbitant consumption
29.
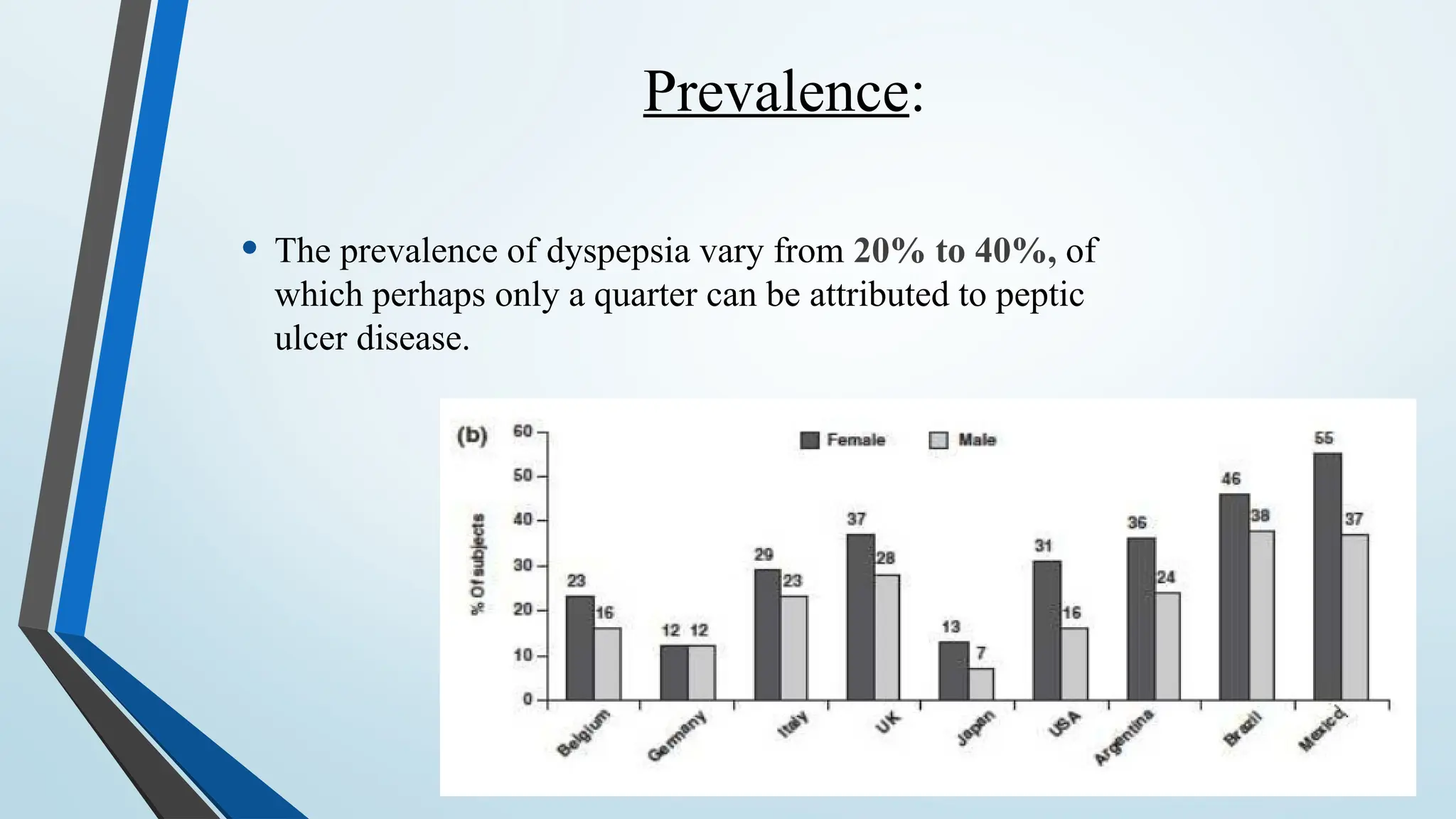
Prevalence:
• The prevalenceof dyspepsia vary from 20% to 40%, of
which perhaps only a quarter can be attributed to peptic
ulcer disease.
30.
Symptoms:
• The followingsymptoms of dyspepsia are also common
• Heartburn and dyspepsia are often
confused for one another, but they
are two separate conditions despite
regularly occurring at the same time.
Heartburn is a symptom of acid reflux
described as a burning feeling behind
the breastbone that usually occurs
after eating.
• Pain
• Nausea
• Vomiting
• Sweating
• Shortness of breath
• Feeling bloated
• Chest pain
• Inability to
swallow
31.
Causes:
• Indigestion isusually caused by the lifestyle of an individual and the foods
they eat.
Symptoms are normally triggered by stomach acid
coming into contact with the mucosa.
Gallstones
Infection, especially with a bacteria called
Helicobacter pylori (H. pylori)
Nervousness
Obesity
Pancreatitis, or inflammation of the pancreas
Peptic ulcers
Smoking
32.
Dietary management:
• Ahigh-fiber diet is a good way to manage digestive health. It has the effect of
clearing out the intestine and making digestion a smoother, cleaner process.
• Fruits, nuts, legumes, and wholegrain
foods are packed with fiber and an
excellent choice for protecting against
indigestion. Many yogurts and cereals
have also been fortified with fiber.
• Eating a balanced diet that excludes spicy or greasy foods is key. Be sure to
consume fluids with every meal, as this helps to move food through the digestive
tract.
33.
Treatment
• Treatment forindigestion depends on the cause and severity of symptoms.
• If symptoms are mild and infrequent, lifestyle changes will probably
ease them. This usually involves consuming fewer fatty and spicy
foods and less caffeine, alcohol, and chocolate. Sleeping for at
least 7 hours every night may also help to ease mild indigestion.
• Exercising regularly and quitting smoking are also important lifestyle changes in treating
indigestion.
Introduction:
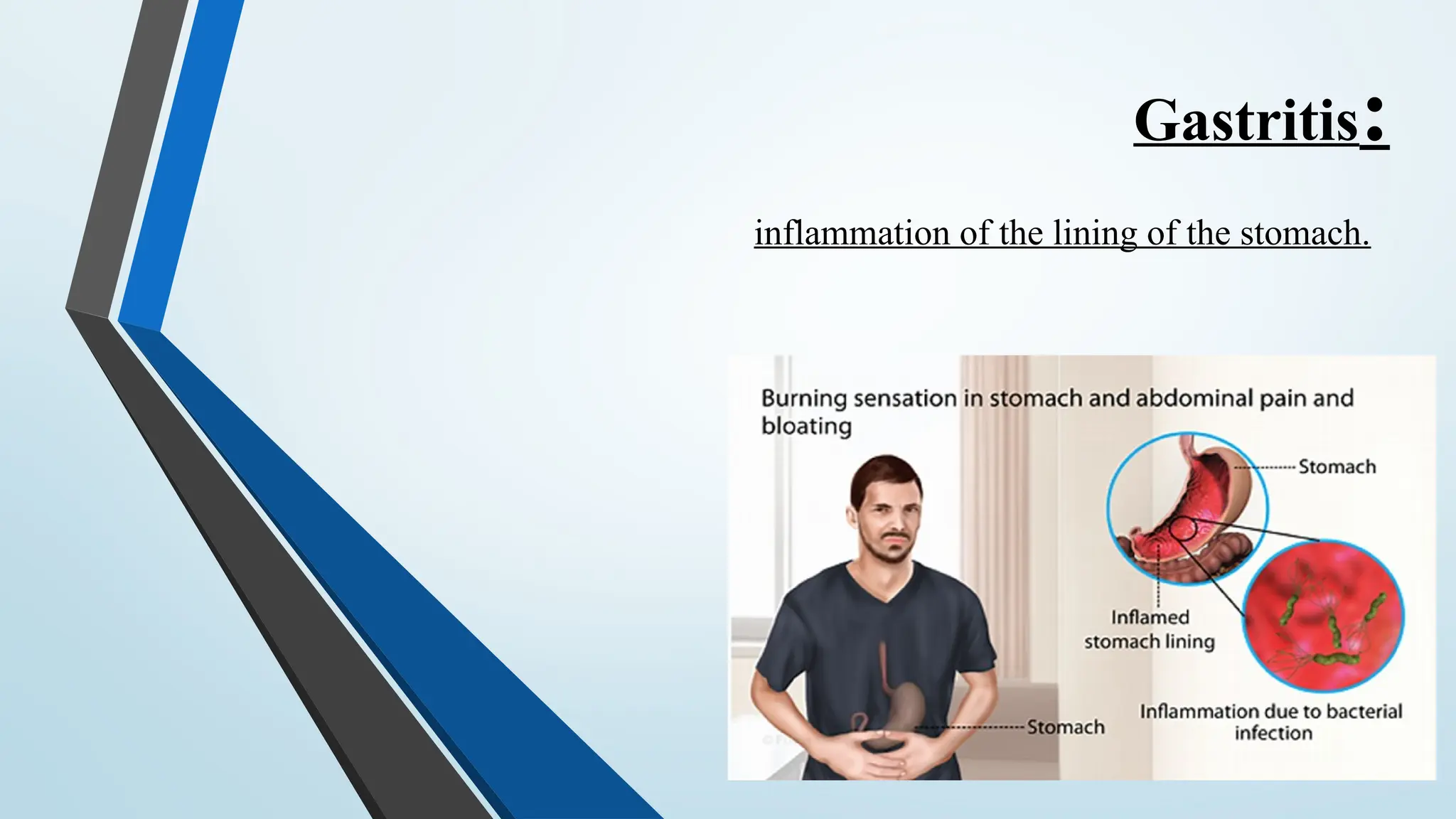
• Gastritis isa group of diseases that cause inflammation of the lining of the
stomach.
• There are two types of gastritis:
oAcute gastritis: occurs suddenly, and will frequently respond to appropriate
therapy, while
oChronic gastritis: develops slowly. .
Erosive gastritis: Erosive gastritis leads to small breaks in the stomach
lining (erosions) or ulcers, Non-erosive gastritis: Non-erosive gastritis
results in inflammation of the stomach lining, but no ulcers.
The inflammation of the stomach lining is most frequently caused by a
bacterium called H. pylori. Gastritis can vary greatly from mild gastritis to
severe gastritis. Symptoms might not always be correlated with the severity
of the disease.
36.
Gastritis prevalence:
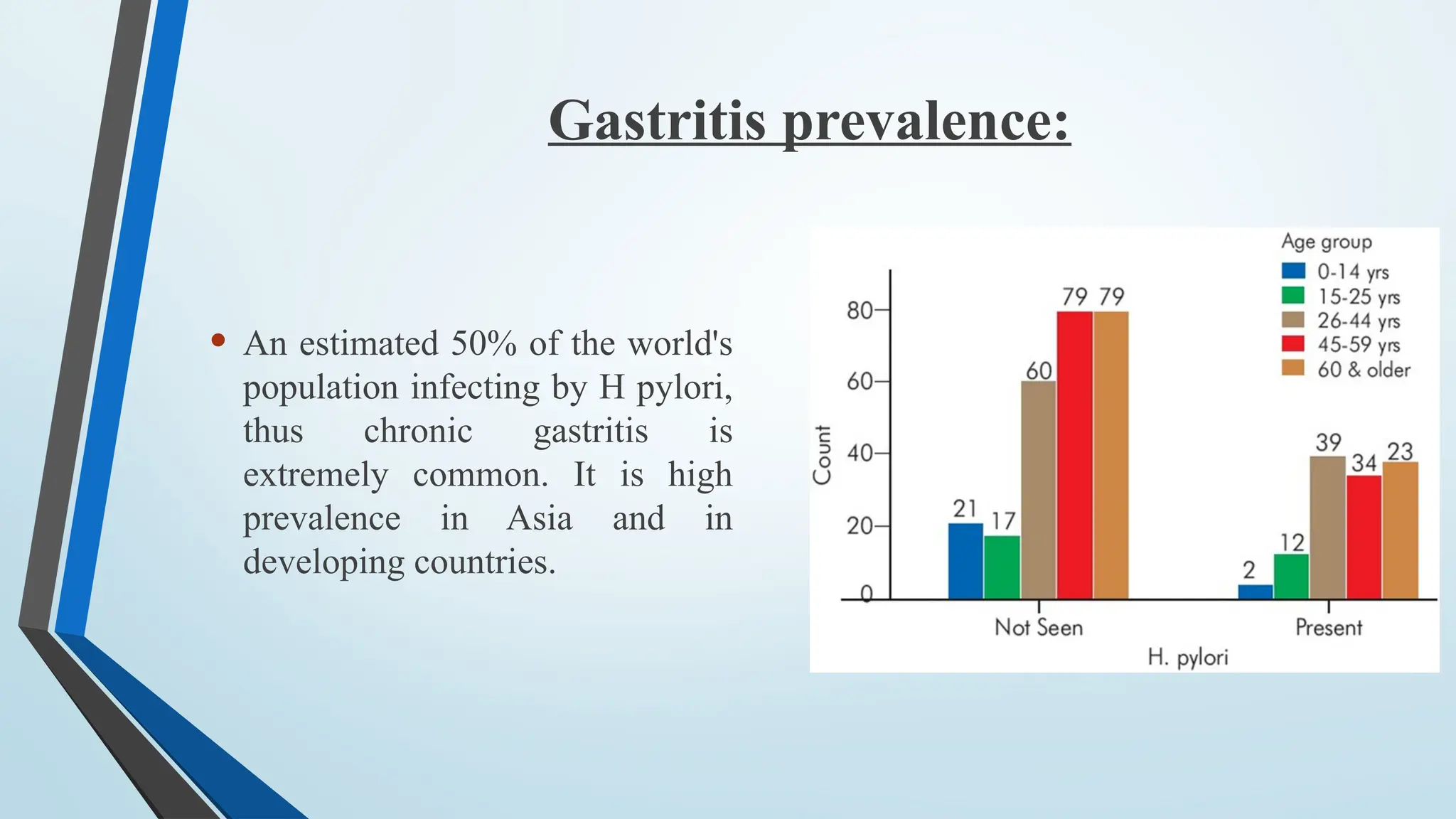
• Anestimated 50% of the world's
population infecting by H pylori,
thus chronic gastritis is
extremely common. It is high
prevalence in Asia and in
developing countries.
37.
Causes of Gastritis:
•Gastritis, acute or chronic inflammation of
the mucosal layers of the stomach.
o Acute gastritis may be caused by excessive
intake of alcohol, ingestion of irritating drugs,
food poisoning, and infectious diseases.
oChronic gastritis may be caused by
prolonged use of aspirin or nonsteroidal anti-
inflammatory drugs (NSAIDs), infection with
Helicobacter pylori, or pernicious anemia
38.
Symptoms:
Some ofthe most common symptoms of gastritis include:
• Abdominal pain, especially in the upper abdomen
• Changes in bowel habits or abdominal upset
• Indigestion
• Abdominal bloating
• Nausea
• Vomiting
• Poor apatite.
39.
Diet therapy:
• AcuteGastritis: The only treatment necessary is temporary avoidance of
food, like acidic foods.
• Chronic Gastritis: The treatment for chronic gastritis depends on its cause;
antacids will usually eliminate symptoms and promote healing. Antibiotics
are used to treat chronic gastritis caused by H. pylori infection. Chronic
gastritis caused by pernicious anemia is treated with cobalamine [1].
• Food should avoided: These include very acidic foods, spicy or hot foods,
alcohol , caffeine, and processed/packaged foods.
• foods should take: foods high in fiber, antioxidants like vitamin C,
electrolytes like magnesium and calcium, vitamin B12, probiotics and
omega-3 fatty acids can help lower inflammation and boost digestive health.
40.
Continue…
• A healinggastritis diet that features mostly vegetables, fruits, high-quality
proteins and healthy fats can help manage painful symptoms, allow you to
maintain a healthy weight, and prevent deficiencies in critical vitamins,
minerals and antioxidants that can lead to further complications down the
road [2].
• Precautions :
• Avoid eating too close to bedtime,
• Eat smaller meals,
• Drink enough water:
• Reduce stress,
• Quit smoking and lower toxin exposure
INTRODUCTION
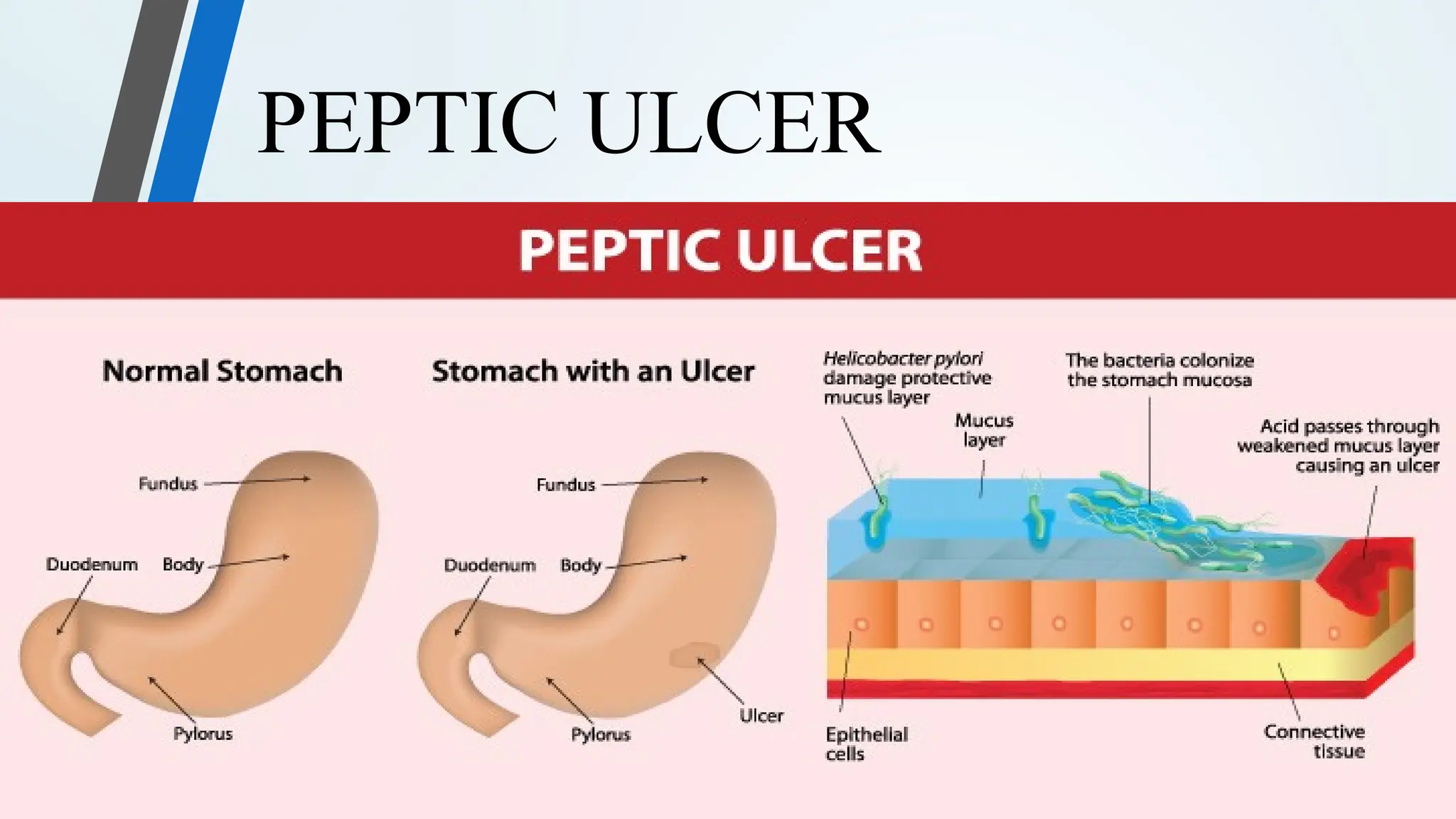
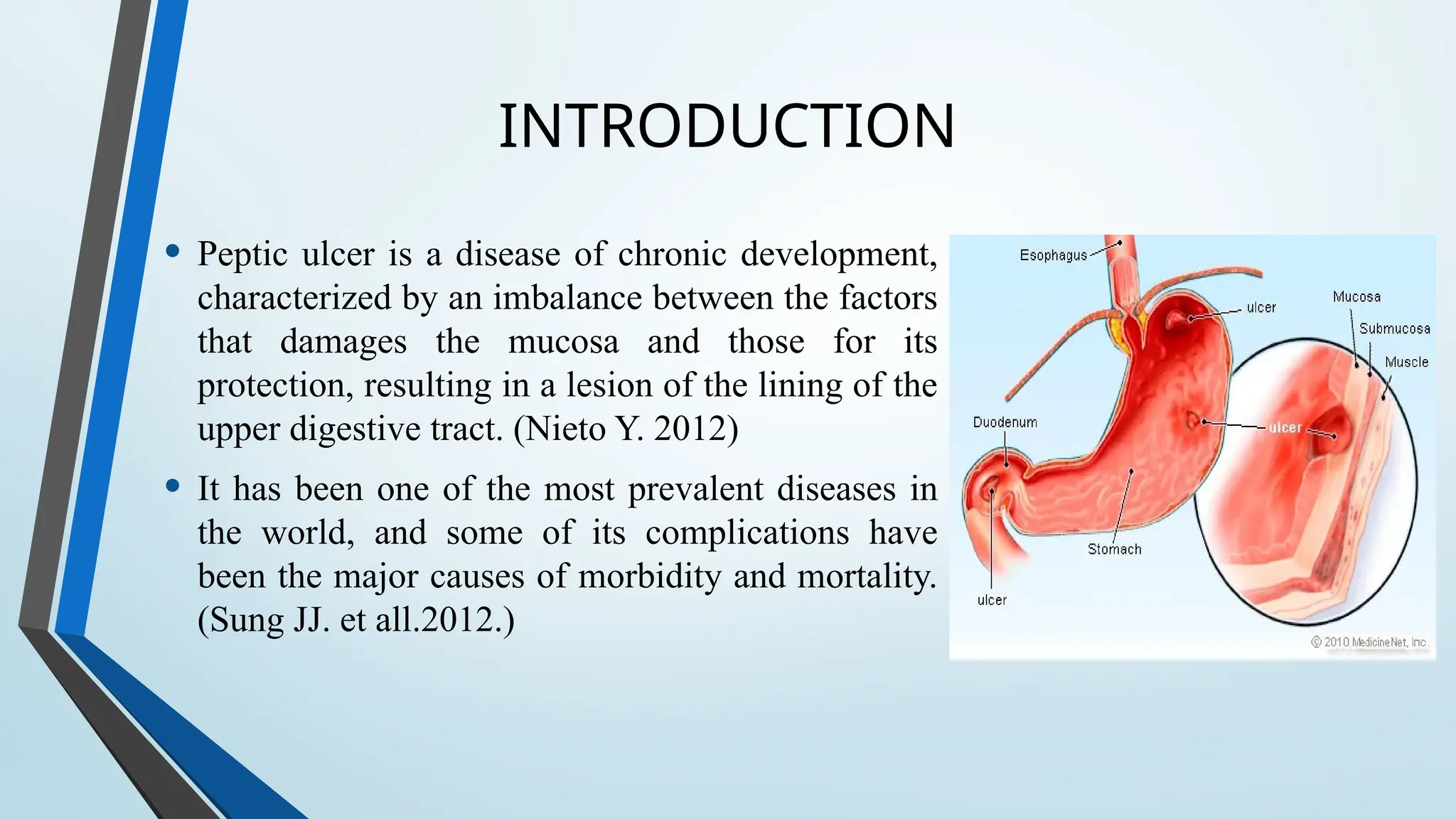
• Peptic ulceris a disease of chronic development,
characterized by an imbalance between the factors
that damages the mucosa and those for its
protection, resulting in a lesion of the lining of the
upper digestive tract. (Nieto Y. 2012)
• It has been one of the most prevalent diseases in
the world, and some of its complications have
been the major causes of morbidity and mortality.
(Sung JJ. et all.2012.)
43.
PREVALENCE
• The prevalencediffers in the world population between the duodenal and
gastric ulcers, and the mean age of people with the disease is between 30 and
60 years, but it can happen in any age.
• The prevalence of peptic ulcer disease in the United States is estimated to be
8.4%. (Chey WD, et all. 2017)
44.
PATHOPHYSIOLOGY
• Peptic ulceris characterized by a solution of continuity the upper digestive
tract mucosa exposed to chloride peptic secretion. It often occurs in the
duodenum (5-10% of the population), stomach or esophagus. (Toneto M. et
all. 2011)
• It is a chronic disease, with activation and remission periods and its
pathogenesis is characterized by the imbalance between the factors that
damages the mucosa (chloride acid, pepsin, and ulcerogenic drugs) and those
that protect it (mucosal barrier, prostaglandins, and mucosal secretion).
(Marotta K. et all. 2006)
45.
SYMPTOMS: CAUSES
• Clinicalmanifestations are
characterized by
epigastric discomfort,
burning or severe and continuous
pain, which tends to be worse at night.
Pain usually happens one to three
hours after eating,
• and may be followed by nauseas,
vomiting, discomfort in the
gastrointestinal tract, flatulence, and
significant loss of body weight.
(Nieto Y.2012.)
• Peptic ulcer has a multifactor etiology.
Environmental elements such as
alcohol
nicotine
Helicobacter pylori
• Genetic factors can influence, and
children of parents with duodenal ulcer
are three times more likely to have ulcer
than the population.
• Non steroidal anti inflammatory drugs.
(Lafortuna CL. et all. 2006)
46.
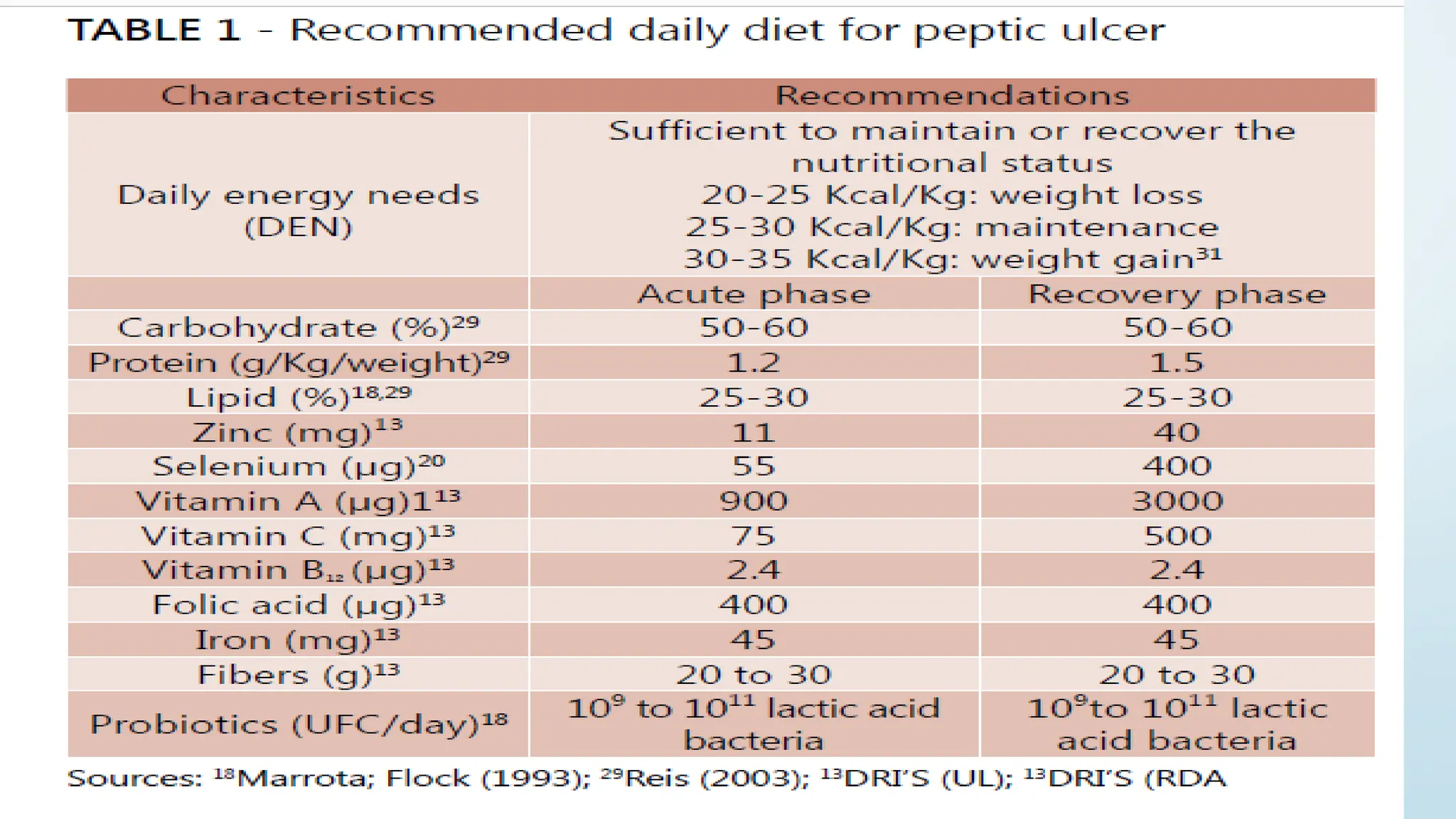
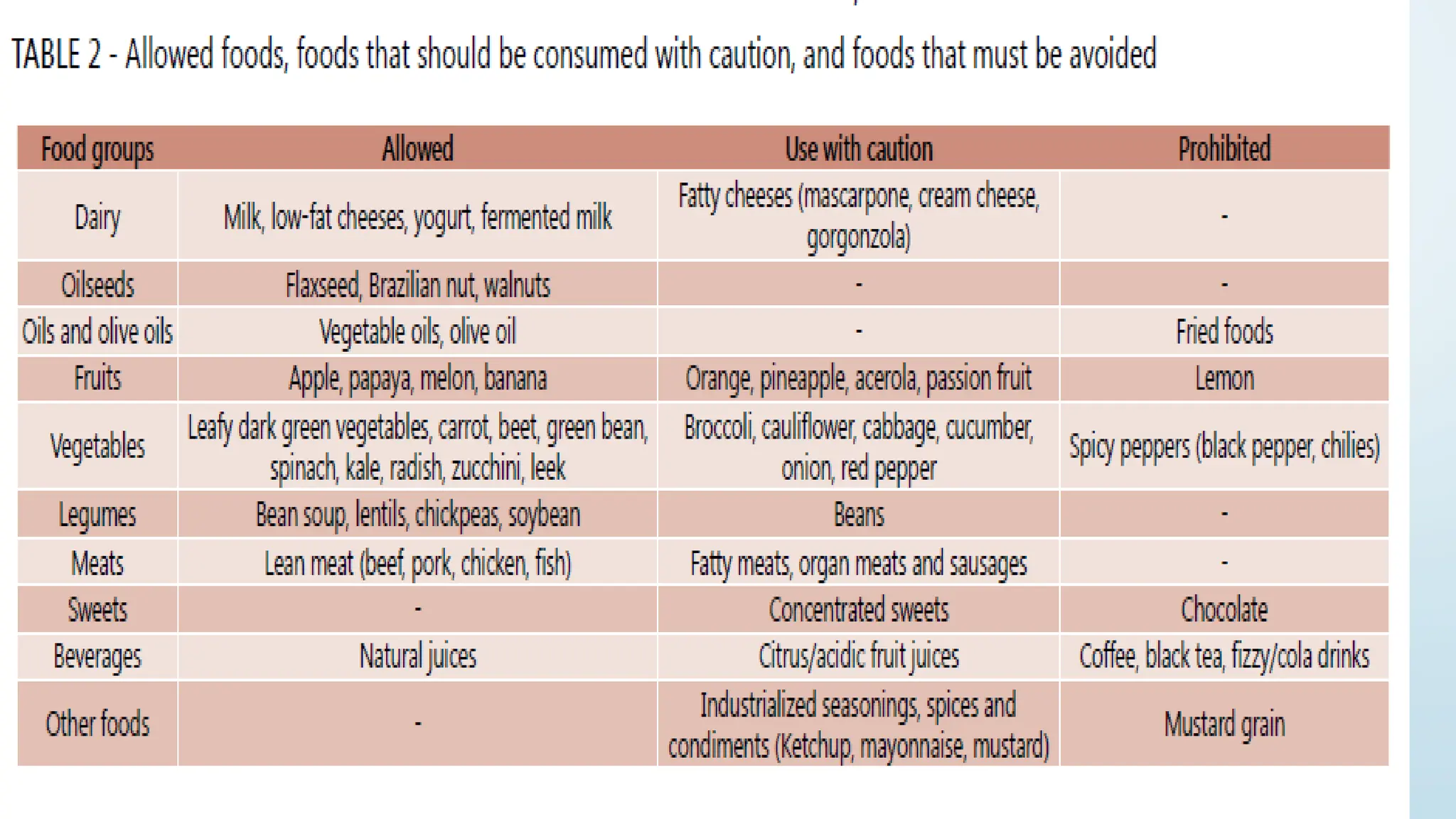
DIET THERAPY FORPEPTIC ULCER:
• Calories distribution
• Use of food fibers in peptic ulcer treatment
• Use of antioxidants to eradicate Helicobacter pylori
• Use of probiotics in peptic ulcer
• Antacids versus nutrients bioavailability
• Avoid substances that potentiate peptic ulcer symptoms
49.
REFERENCES
• 1:Vakil N,van Zanten SV, Kahrilas P, Dent J, Jones R; Global
Consensus Group. The Montreal definition and classification of
gastroesophageal reflux disease: a global evidence-based
consensus. Am J Gastroenterol 2006;101:1900-1920.
• 2:El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the
epidemiology of gastro-oesophageal reflux disease: a systematic
review. Gut 2014;63:871-880.
• 3:Nasrollah L, Maradey-Romero C, Jha LK, Gadam R, Quan SF, Fass
R. Naps are associated more commonly with gastroesophageal
reflux, compared with nocturnal sleep. Clin Gastroenterol Hepatol
2015;13:94-99.
50.
CONT….
• 4:Dore MP,Maragkoudakis E, Fraley K, et al. Diet, lifestyle and
gender in gastro-esophageal reflux disease. Dig Dis Sci
2008;53:2027-2032.
• 5:Spechler SJ, Sharma P, Souza RF, Inadomi JM, Shaheen NJ.
American Gastroenterological Association medical position
statement on the management of Barrett’s esophagus.
Gastroenterology 2011; 140: 1084-1091 [PMID: 21376940
DOI:10.1053/j.gastro.2011.01.030]
• 6:Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures
effective in patients with gastroesophageal reflux disease? An
evidence-based approach. Arch Intern Med 2006; 166:965-971
[PMID: 16682569 DOI: 10.1001/archinte.166.9.965]
51.
Reference
Dandy B.C., WilsonS., Rolfed A., Roberts L., Redman V., Warn A., et
al. (2000)
Cost effectiveness of initial endoscopy for dyspepsia in patients
over age 50 years: a randomized controlled trial in primary care
What to know about indigestion or dyspepsia
Last updated Thu 7 December 2017 By Christian Nordqvist Reviewed by Michele Cho-Dorado,
MD
1.https://www.britannica.com/science/gastritis
2.Jillian Levy, CHHC (May 16, 2016 ), By https://draxe.com/gastritis-diet
52.
• Toneto M,Oliveira F, Lopes MH. Evolução histórica da úlcera péptica:
da etiologia ao tratamento. Scientia Medica. 2011;21:23-30.
• Sung JJ, Tsoi KK, Ma TK, Yung MY, Lau JY, Chiu PW. Causes of mortality
in patients with peptic ulcer bleeding: a prospective cohort study of
10,428 cases. Journal Gastroenterol. 2012;105:84-89.
• Nieto Y. Protocolo terapéutico de la úlcera péptica. Medicine.
2012;11:179-82.
• ABCD Arq Bras Cir Dig 2014;27(4):298-302

![INTRODUCTION
The upper gastrointestinal tract consists of the esophagus, stomach, and
duodenum. The exact demarcation between upper and lower can vary. The
upper gastrointestinal tract includes the:
• Esophagus, the fibromuscular tube that food passes through—aided by
peristaltic contractions—the pharynx to the stomach.
• Stomach, which secretes protein -digesting enzymes called proteases
and strong acids to aid in food digestion, before sending the partially digested
food to the small intestines.
• Duodenum, the first section of the small intestine that may be the
principal site for iron absorption. [Kierszenbaum, A. L.].](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-3-2048.jpg)

![ESOPHAGEAL DYSPHAGIA
Esophageal dysphagia refers to the sensation of food sticking or getting hung
up in the base of your throat or in your chest after you've started to swallow.
Some of the causes of esophageal dysphagia .
• Aschalasia
• Diffuse spasm
• Oesophageal stricture
• Oesophageal tumors
• Esophageal ring
• GERD
• Eosinophilic esophagitis
[ Martino R, Foley N, Bhogal S, et al]](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-12-2048.jpg)
![OROPHARYNGEAL DYSPHAGIA
Certain conditions can weaken your throat muscles, making it
difficult to move food from your mouth into your throat and
esophagus when you start to swallow.
• You may choke, gag or cough when you try to swallow or
have the sensation of food or fluids going down your
windpipe (trachea) or up your nose.
• This may lead to pneumonia.
Causes of oropharyngeal dysphagia include:
•Neurological disorders.
•Neurological damage.
•Pharyngoesophageal diverticulum (Zenker's diverticulum).
•Cancer.[ Miller RM, Chang MW]](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-13-2048.jpg)
![GERD
Gastroesophageal reflux disease (GERD) is a common disease characterized by
reflux of stomach contents into the esophagus.[Vakil, et al, 2006]
PREVELENCE:
• GERD ranged from
18.1% to 27.8% in North America
8.8% to 25.9% in Europe
2.5% to 7.8% in East Asia
8.7% to 33.1% in the Middle East
11.6% in Australia
23.0% in South America.[El-Serag, et al, 2014]](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-16-2048.jpg)
![SYMPTOMS
• The symptoms of GERD are heartburn and regurgitation.[Nasrollah, et al,
2015]
GERD may have other symptoms, including
Mouth sours
chest pain or discomfort
epigastric pain
Nausea
bloating
throat pain or burning
sleep disturbances.](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-17-2048.jpg)
![CAUSES
• Weakening or inappropriate relaxation of
lower esophageal sphincter
• overweight or obese because of increased
pressure on the abdomen
• Pregnant, due to the same increased pressure
• Associated with hiatal hernia (a condition in
which the upper portion of the stomach
protrudes above the diaphragm )[Dore, et al,
2008]](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-18-2048.jpg)
![Complications
GERD can worsen and turn into other conditions
if left untreated.
These include:
Esophagitis: This is an inflammation of the
esophagus.
Esophageal stricture: In this condition, the
esophagus becomes narrow, making it difficult
to swallow.
Barrett's esophagus: The cells lining the
esophagus can change into cells similar to the
lining of the intestine. This can develop into
cancer.[Spechler, et al, 2011]](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-20-2048.jpg)
![Treatment of GERD - lifestyle
modifications
Lifestyle changes: [Kaltenbach, et al, 2006]
Lifestyle and diet modification traditionally have included:
• Lose weight if needed because weight loss decreases intra-abdominal
pressure.
• Consume meals 2-3 hours before bedtime.
• Avoid eating bedtime snacks or lying down immediately after meals
Remain upright for 45 to 60 minutes after eating.
• Prop pillows under the head and upper torso during sleeping.
• Avoid wearing tight clothing that increases pressure in the stomach.](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-24-2048.jpg)
![Diet therapy:
• Acute Gastritis: The only treatment necessary is temporary avoidance of
food, like acidic foods.
• Chronic Gastritis: The treatment for chronic gastritis depends on its cause;
antacids will usually eliminate symptoms and promote healing. Antibiotics
are used to treat chronic gastritis caused by H. pylori infection. Chronic
gastritis caused by pernicious anemia is treated with cobalamine [1].
• Food should avoided: These include very acidic foods, spicy or hot foods,
alcohol , caffeine, and processed/packaged foods.
• foods should take: foods high in fiber, antioxidants like vitamin C,
electrolytes like magnesium and calcium, vitamin B12, probiotics and
omega-3 fatty acids can help lower inflammation and boost digestive health.](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-39-2048.jpg)
![Continue…
• A healing gastritis diet that features mostly vegetables, fruits, high-quality
proteins and healthy fats can help manage painful symptoms, allow you to
maintain a healthy weight, and prevent deficiencies in critical vitamins,
minerals and antioxidants that can lead to further complications down the
road [2].
• Precautions :
• Avoid eating too close to bedtime,
• Eat smaller meals,
• Drink enough water:
• Reduce stress,
• Quit smoking and lower toxin exposure](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-40-2048.jpg)
![CONT….
• 4:Dore MP, Maragkoudakis E, Fraley K, et al. Diet, lifestyle and
gender in gastro-esophageal reflux disease. Dig Dis Sci
2008;53:2027-2032.
• 5:Spechler SJ, Sharma P, Souza RF, Inadomi JM, Shaheen NJ.
American Gastroenterological Association medical position
statement on the management of Barrett’s esophagus.
Gastroenterology 2011; 140: 1084-1091 [PMID: 21376940
DOI:10.1053/j.gastro.2011.01.030]
• 6:Kaltenbach T, Crockett S, Gerson LB. Are lifestyle measures
effective in patients with gastroesophageal reflux disease? An
evidence-based approach. Arch Intern Med 2006; 166:965-971
[PMID: 16682569 DOI: 10.1001/archinte.166.9.965]](https://image.slidesharecdn.com/uppergitjax-250629083716-b5d91634/75/UPPER-GIT-presentation-Gastrointestinal-tract-50-2048.jpg)