Gland
1.Exocrine gland
2.Endocrine gland
Hormones
Functions
Comparison with Nervous system
Regulation of Hormonal secretion
Chemical classification of hormones based on:
1.Solubility
Lipophilic
Lipohobic
2.Synthetic origin
Amine ,Protein (polypeptide) ,Steroid
MOA
Site of synthesis [rER or sER] ,release, transport,
metabolism & excretion:
Endocrine basis of hormone disorders
Major endocrine glands & tissues
1.Central endocrine glands
1. Pineal gland
2. Hypothalamus
3. Pituitary (hypophysis) gland
2.Peripheral endocrine glands
1. Thyroid glands
2. Parathyroid glands
3. Adrenal (suprarenal) glands
4. Thymus gland
5. Part of pancreas (islet of Langerhans)
6. Gonads (reproductive glands)
1. Testis
2. Ovary
1.Adipose tissue (fat cell/tissue)=
2.Small intestine & Skin=
3.Stomach=
4.Kidney=
5.Heart=ANP
6.Liver =IGF (somatomedin-c)
Angiotensinogen
Thrombopoietin
2
Hormone
secretion
as
secondary
function
Learning Objectives
3.
Terminologies
1. Target organorgan that has specific receptors to which the hormone [messenger] binds specifically.
2. Adeno- Gland
3. Hypophysis Pituitary Underneath growth
4. Adenohypophysis Glandular Pituitary gland [Anterior]
5. Neurohypophysis Neural pituitary gland [Posterior]
6. Neuroendocrine cells function as the nervous & endocrine systems (dual functions)
7. Hypophyseal portal system[HPS] Is the conduit that connects the brain to the anterior pituitary.
8. Largest gland thyroid gland
9. Love hormone oxytocin
10. Stress hormone cortisol
11. Master gland pituitary
12. 99% Ca2+ is stored inside bone
13. Seat of the soul pineal gland
14. Active form of thyroid hormone is T3
15. Hashimoto's disease autoimmune disorder of the thyroid gland
3
4.
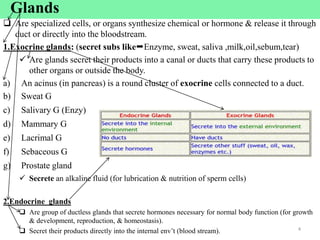
Glands
Are specializedcells, or organs synthesize chemical or hormone & release it through
duct or directly into the bloodstream.
1.Exocrine glands: (secret subs likeEnzyme, sweat, saliva ,milk,oil,sebum,tear)
Are glands secret their products into a canal or ducts that carry these products to
other organs or outside the body.
a) An acinus (in pancreas) is a round cluster of exocrine cells connected to a duct.
b) Sweat G
c) Salivary G (Enzy)
d) Mammary G
e) Lacrimal G
f) Sebaceous G
g) Prostate gland
Secrete an alkaline fluid (for lubrication & nutrition of sperm cells)
2.Endocrine glands
Are group of ductless glands that secrete hormones necessary for normal body function (for growth
& development, reproduction, & homeostasis).
Secret their products directly into the internal env’t (blood stream). 4
5.
What is theEndocrine system?
It is a system of control ,communication & coordination of body functions
It uses chemical signals called hormones for cell to cell communication
Is a collection of ductless glands (endocrine glands) & specific cells that secrete
chemical messengers called hormone [H].
This chemical messenger is transported (circulated) within the body mostly
through blood.
It arrives at distant cells within specific target organs.
The target organs have cells possessing appropriate receptors for that H.
5
6.
What are hormones[H]?
H are chemical messengers or signal molecules:
Synthesized by ductless endocrine cells
Released directly in to the blood stream
Act on target cells that have receptors for that hormone
Their action is slower & long-term.
6
Circadian rhythm:
• Is a biological processes occurring at 24-hr interval
• Is inherent cycle or a daily rhythmic activity cycle, based on 24-hr intervals, that is exhibited by many organisms.
7.
Functions of hormones
1.Regulationof reproduction: gametogenesis, sexual desire, coitus, fertilization.[T,Estrogen,P]
2.Regulation of body growth & development [GH, T3 & T4]
3.Production, utilization & storage of energy [Insulin, T3 & T4]
4.Growth & development of brain [T3 & T4]
5.Response to stress or injury & infections [Cortisol,]
6.Energy metabolism [T3 & T4]
7.Homeostasis: maintenance of the internal environment in the body.
Water (fluid)-electrolyte balance=ADH ,Aldosterone
Regulation of ABP= Renin ,ADH & Aldostrone
Control of BT [T3&T4], emotion (NE)
Change in mass of bone [PTH,calcitonin,Estrogen], muscle [T] ,RBCs [T,ErtPO] & fat [Estrogen]
8.Circadian rhythm [Serotonin or melatonin]
A rhythmic activity cycle, based on 24-hrs interval
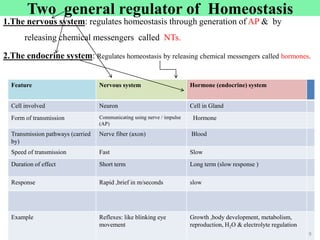
Two general regulatorof Homeostasis
1.The nervous system: regulates homeostasis through generation of AP & by
releasing chemical messengers called NTs.
2.The endocrine system: Regulates homeostasis by releasing chemical messengers called hormones.
Feature Nervous system Hormone (endocrine) system
Cell involved Neuron Cell in Gland
Form of transmission Communicating using nerve / impulse
(AP)
Hormone
Transmission pathways (carried
by)
Nerve fiber (axon) Blood
Speed of transmission Fast Slow
Duration of effect Short term Long term (slow response )
Response Rapid ,brief in m/seconds slow
Example Reflexes: like blinking eye
movement
Growth ,body development, metabolism,
reproduction, H2O & electrolyte regulation
9
10.
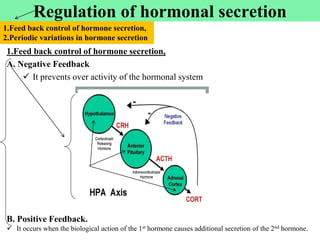
Regulation of hormonalsecretion
1.Feed back control of hormone secretion,
A. Negative Feedback
It prevents over activity of the hormonal system
B. Positive Feedback.
It occurs when the biological action of the 1st hormone causes additional secretion of the 2nd hormone.
1.Feed back control of hormone secretion,
2.Periodic variations in hormone secretion
Cont‘d
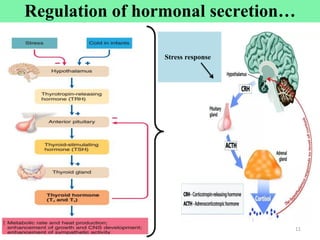
2.Periodic variations inhormone secretion
Hormone secretion influenced by:
A. Seasonal change [serotonin]
B. Various stages of development [T,E] & aging [E],
C. The diurnal or daytime cycle & sleep cycle or at night or nocturnal.
E.g.
I. The secretion of GH increased during the early period of sleep but is reduced
during the later stages of sleep & at day time.
II. Some hormones more secreted in adolescence stage
III. LH surge at ovulation [around 14 day of 28 days]
12
Regulation of hormonal secretion…
13.
Chemical classification ofhormones
Classification based on [Solubility & Synthetic origin]
A. Solubility
1.Lipophilic :(water insoluble=steroid H)
Are lipid hormone made from cholesterol & are fat soluble
Easily cross lipid bilayer part of target organ
Receptor location in cytoplasm or nucleus (intracellular)
No need of 2ndary messenger
2.Lipophobic:amino acid [aa] based hormone made up of aa
Either a single modified amino acid or a protein made up of 3-200aa
Are hydrophilic: amine & peptide hormones
NB:But thyroid hormones (amine) are water insoluble
Receptor locationon surface (on cell membrane)
Bind to a receptor protein on the surface of the target cell & produce
physiological change in the cell.
But need 2ndary messenger 13
Thyroid hormonesT3 & T4
14.
B.Synthetic origin (derivedfrom tyrosine , tryptophan,cholestrol)
3 general classes of hormones:
1.Protein & polypeptide hormones: amino acids linkage
2.Steroid hormones :synthesized from cholesterol in a series of rxns
3.Amine hormones :(derivatives of a single amino acid like tyrosine, tryptophan)
1. Derivatives of the amino acid Amine hormones
Are hormones derived from amino acids tyrosine or tryptophan
Their receptor found on cell surface BUT thyroid hormones in nucleus
Includes : hormones secreted by
Thyroid gland ((thyroxin (T4) & triiodothyronine (T3)) = (lipid soluble)
Adrenal medulla (epinephrine & norepinephrine)
Pineal gland (melatonin & serotonin)
Hypothalamus dopamine
14
Chemical classification of hormones…
Catecholamines (E,NE,Dopamine) hormones used as neurotransmitter [NT]
15.
Cont’d
2.Proteins & polypeptideshormones
Made up of small to many amino acids
Their receptor found on cell surface
Includes : hormones secreted by
Anterior & posterior pituitary gland
Pancreas (insulin & glucagon)
Parathyroid gland (PTH)
Hypothalamic hormones but dopamine is
amine
3. Steroids hormones
These are lipids derived from cholesterol.
Their receptor found intracellular (in target
organ cytoplasm or nucleus)
Includes :hormones secreted by:
Adrenal cortex :(cortisol & aldosterone,
androgen)
Ovaries & Placenta :(estrogen &
progesterone)
Testes: (testosterone)
Vit-D3 [calcitriol]
15
Chemical classification of hormones…
T3 & T4 Tyrosine
Serotonin,melatoninTryptophan
16.
Hormone class ComponentsExample
Amine H
Catecholamine
Amine H
Thyroid hormones
• Amino acid with modified group
• Receptor location =on Plasma membrane [PM]
• Amino acid with modified group
• Receptor location =in nucleus
• NE,E,Dopamine,melatonin
• Serotonin [precursor of melatonin]
T3,T4
Peptide H • Chain of linked amino acids • Oxytocin
• ADH
• Insulin/glucagon
• PTH,GH etc.
Steroid H • Derived from the lipid cholesterol
• Can freely pass through PM
• Receptor location = in Cytoplasm or nucleus
• Testosterone (androgen)
• Progesterone, Estrogen
• Cortisol, aldosterone
• Vit-D
16
Chemical classification of hormones…
17.
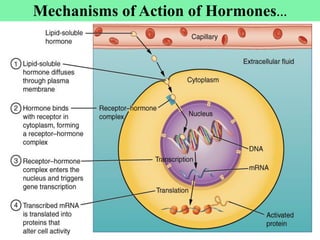
Mechanisms of Actionof Hormones
The first step of a hormone's action is to bind to specific receptors at the target cell [organ].
Cell that lack receptors for the hormones does not respond.
The locations of receptors for the different types of hormones are:
1. Receptors on the surface of the cell membrane.
Such receptors are specific mostly for the protein, peptide, & catecholamine hormones. &
Act through 20 messengers
20 messengers can be:
1. cAMP,DAG
2. cGMP
3. IP3 (inositol 1,4,5 triphosphate)
4. Ca2+ etc.
17
18.
2. Receptors inthe cell, either:
A. In the cell cytoplasm
The primary receptors for the different steroid hormones found mainly in the
cytoplasm. Or
B. In the nucleus
Are receptors for thyroid hormones
Located in direct association with one or more of the chromosomes.
Such hormones are,
Lipid soluble
Readily cross cell membrane &
Interact with receptors in the cytoplasm or nucleus 18
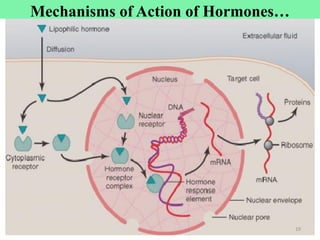
Mechanisms of Action of Hormones…
Hormone: synthesis, release,
transport,metabolism & excretion
Site of synthesis :(in the cell, cell body or soma)
Protein/peptide hormones: in the rER
Steroid hormones: in the sER
Release: Exocytosis
Transport: hormones are transported in blood in two forms:
a. In the free form (dissolving in plasma)have short half life
b. In combination with plasma proteins (or carrier proteins :albumin & globulin).
Have long half life
Metabolism: metabolized in the liver or by target cells [organs]
Excretion: urine, feces, sweat
21
22.
1.Over production ofhormones
a.Gigantism (childhood),Acromegaly (adult )GH
b.Hyperthyroidism Grave’s disease (toxic goiter or exophthalmic goiter) [T3 &T4]
c.Cushing’s syndrome adrenal cortex (cortisol) "buffalo hump") "moon face")
d.Galactorhea prolactin [PRL]
e.Conn’s disease Aldosterone
2.Under production of hormones
a. Dwarfism GH
b. Hypothyroidism Cretinism, myxedema ,Goiter (endemic) & Hashimoto's disease [ T3 &T4]
c. Addison’s disease adrenal cortex [ cortisol & Aldosterone]
d. Diabetes mellitus (IDDM or Type 1-DM) Insulin
e. Diabetic insipidus Posterior pituitary ADH [alcohol]
f. Osteoporosis Estrogen (woman >45yrs) & calcitonin
3.Non-functional receptors for the Hormones
Target cells become insensitive to the hormone
Eg. Diabetes mellitus (NIDDM or type II)
22
Endocrine basis of hormone disorders
RicketsIn Children
Osteomalacia In Adult
23.
The principal endocrineglands & endocrine tissues of the body
1. Hypothalamus
2. Pineal gland
3. Pituitary
4. Thyroid
5. Parathyroid
6. Thymus
7. Adrenal gland
8. Pancreas
9. Ovaries
10. Testes
1. HeartANP
2. KidneyErpo, vit-D (calcitriol),Rennin
3. StomachGastrin, Ghrelin [appetite]
4. Small intestine Motilin,Secretin,CCK, neuropeptide-Y,histamin
5. Adipose tissue (fat cell/tissue)Leptin [appetite]
6. Liver IGF (Somatomedin-c),Angiotensinogen ,Thrombopoietin
Endocrine tissues Or organs
23
Endocrine glands
23
Gonads
24.
24
A. Central endocrineglandsincludes;
1. Hypothalamus
2. Pituitary gland (hypophysis)
3. Pineal gland melatonin amine hormone sleep & weak cycle
(as circadian rhythm or as body biological clock].
B. Peripheral endocrine glands includes:
1. Thyroid glands
2. Parathyroid glands
3. Thymus gland
4. Adrenal gland
5. Pancreas
6. Gonads (Ovaries & Testes)
Endocrine glands: divided in to 2; Central & Peripheral
Location [HT]
HT is part of the diencephalons, which forms the floor & the lateral wall of the
3rd ventricle Or found just under the thalamus. Or
Found above the pituitary gland
It is extremely complex part of brain
It contains many regions (nuclei) with highly specialized functions
HT represents less than 1% of the brain mass, about 5gm (so small but so
important area of brain)
Regardless of its size, it plays most important roles in controlling homeostasis
It is the main brain structure involved in regulating hormonal levels in the body
26
Hypothalamus (HT)…
27.
Functions,
Somefunctions of different parts or regions of HT:
Regulates temperature :(it gives response to cold & heat) for thermal regulation
It has hunger & satiety center if they damaged hyperphagia or starvation.
It has thirst center it regulates drinking
Regulate sexual behavior :(it has sex drive center)
Control circadian rhythms :(control sleep & wake cycle)
Control autonomic NS : (sympathetic vs parasympathetic regulation)
Endocrine function:(HT Releases or secrets hypothalamic releasing & inhibiting hormones)
In turn, those hormones {H} stimulate pituitary H secretion
Etc.[many]. 27
Hypothalamus (HT)...
28.
HT:Relationship withpituitary gland :
The most important function of the HT is to link the nervous system to the
endocrine system via the pituitary gland.
HT is the main coordinating center b/n the endocrine & nervous system.
HT synthesizes & secretes certain neuro-hormones called hypothalamic –
releasing & inhibiting hormones &
These in turn stimulate or inhibit the secretion of pituitary hormones
The hypothalamus & pituitary gland have both anatomical & functional relationships.
28
Hypothalamus (HT)...
29.
The pituitarygland [PG]: is connected to the hypothalamus by stalk like structure called infundibulm.
PG is divided into an anterior lobe (adenohypophysis) & posterior lobe (neurohypophsis).
So, HT exerts its effects on pituitary gland in 2 different ways:
A. Hypothalamo-neurohypophysial axis
B. Hypothalamo-adenohypophysial axis
Hypothalamus & Pituitary
29
29
30.
Cont’d
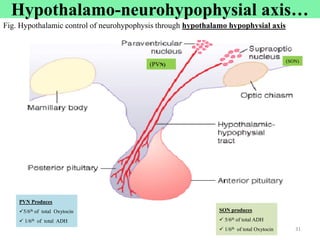
Posterior pituitary:an outgrowth of the hypothalamus composed of neural tissue.
Hypothalamic neurons pass through the neural stalk & end in the posterior pituitary.
Neuroendocrine cells from 2 nuclei in hypothalamus synapse directly on to blood
vessels in posterior pituitary.
These 2 nuclei are:
Supraoptic nucleus (SON) = secrets ADH (5/6th =83% )
Paraventricular nucleus (PVN) = secrets Oxytocin (5/6th =83% )
30
A. Hypothalamo-neurohypophysial axis
Posterior Pituitary Gland [Neurohypophysis]
Is composed mainly of glial-like cells called pituicytes
It does not synthesize hormones, but
Store & secrete 2 hormones:
a. ADH also called ‘Vasopressin’
b. Oxytocin
ADH
Oxy
31.
(SON)
(PVN)
SON produces
5/6thof total ADH
1/6th of total Oxytocin
PVN Produces
5/6th of total Oxytocin
1/6th of total ADH
Fig. Hypothalamic control of neurohypophysis through hypothalamo hypophysial axis
Cont’d
31
Hypothalamo-neurohypophysial axis…
32.
Functions
Regulates waterbalance
Increase water reabsorption by increasing permeability of kidney ducts to
water Reduce volume of urine (diuresis)
That is why it is named as antidiuretic hormone.
Cold & alcohol inhibit the ADH secretion & function means produce high urine output
Factors stimulating release of ADH:
Hyperosmolality (high solute content of blood)
Change in blood volume (high K+)
An increased in Ang-II 32
ADH
Oxytocin
a.ADH
Hypothalamo-neurohypophysial axis…
33.
Cont’d
Hyposecretion ofADH:leads to
Diabetes insipidus=DI :can be neurogenic or nephrogenic
Is caused by deficiency of ADH or ADH receptor insensitivity in Nephron
Manifestation of DI: polyuria & polydipsia
Two types of DI
1. Neurogenic DI
Due to a genetic defect that blocks ADH production
The hypothalamo-hypophysary system is damaged by surgery or disease.
2. Renal [nephrogenic] DI
The renal tubule cells are insensitive to ADH
33
Hypothalamo-neurohypophysial axis…
34.
Cont’d
for parturition &lactation
Function
1.Facilitates transport of sperm in both males & females ductile system
2.Promotion of maternal behavior toward the neonate
In nonhuman mammals, injection of oxytocin induces maternal behavior
3.Induces uterus contraction [Parturition]
Stimulating contraction of the pregnant uterus
Especially toward the end of gestation
34
b.oxytocin
Hypothalamo-neurohypophysial axis…
35.
4. Oxytocin alsoplays an important role in lactation
Baby crying stimulates Oxytocin secretion
Oxy induces myoepithelial contraction (lactation) for milk let-down or milk
ejection in the lactating breast.
In lactation, oxytocin causes milk to be expressed from the alveoli into the ducts
of the breast the baby can obtain it by suckling
Mechanism of milk ejection reflex by oxytocin:
Suckling stimulus on the nipple by the baby
Signals transmitted through sensory nerves to oxytocin neurons in PVN
& SON nuclei in the hypothalamus
Release of oxytocin by the posterior pituitary gland Carried by the blood to
the breasts Causes contraction of myoepithelial cells of breast milk ejection
35
Hypothalamo-neurohypophysial axis…
36.
Cont’d
Special neurons[heterogeneous] in hypothalamus synthesize & secrete neurohormones:
a. Releasing hormones (Librins)
Increase the secretion of hormones from anterior pituitary
b. Inhibiting hormones (Statins)
Inhibit or decrease the secretion of hormones from anterior pituitary
These hormones are carried by hypothalamohypophysial portal vein into adenohypophysis
In the anterior pituitary, librins & statins act on the glandular cells
To control secretion of the anterior pituitary hormones
For each anterior pituitary hormone there is a releasing hormone
For some there is also an inhibiting hormone [GHIH & PRLIH]
36
B. Hypothalamo-adenohypophysial axis [HPA]
37.
The Hypothalamo-anterior pituitaryaxis…
A complex communication system b/n the nervous system & the endocrine system.
1. Hypothalamus
2. Pituitary gland
3. Endocrine glands
37
Negative feedback from the primary target gland modulates the secretion of both
pituitary & hypothalamic hormones.
37
1
Hypothalamo-adenohypophysial axisThe Hypothalamo –anterior Pituitary Axis=HPA
[target gland]
1
38.
The adenohypophysisis connected to HT by a system of blood vessels called the adenohypophyseal portal system. But
The neurohypophsis is connected to HT by a bundle of nerve fibers, called hypothalmo-neurohypophyseal tract.
The anterior pituitary is regulated by hormones secreted by the hypothalamus. However
The posterior pituitary simply stores & releases hormones that are actually produced by the hypothalamus.
Secretion of pituitary is controlled by hypothalamus [HT]
38
Cont’d
2
The Hypothalamo-anterior pituitary axis…
Hormones of Hypothalamus
HT: Produces Or secretes 9 main hormones
7 hormones that travel through portal system & regulate the anterior lobe.
5 of these trigger hormone release & 2 of them inhibit hormone release by the anterior lobe.
The hypothalamus synthesizes oxytocin and ADH that are stored in the posterior pituitary
& released in response to nerve signals.
1. TRH
2. CRH
3. GnRH
4. GHRH
5. PRH
6. GHiH (somatostatin=SST=anti-GH)
7. PIH (Dopamine or anti-prolactin)
8. ADH
9. Oxytocin
40
4
Cont’d
Neuroendocrine cellsin the hypothalamus:
Has axon tract [nerve] on pituitary glands (on both anterior (shorter) & posterior pituitary [longer])
8
Hormones of Hypothalamus…
[SON & PVN]
Heterogeneous [different types of] neurosecretory cells
44.
L & Shormones that regulate the anterior pituitary (glandular cells)
Hypothalamic hormone Effect on pituitary
1.Corticotrophin releasing hormone (CRH) Stimulates ACTH secretion by corticotropes
2.Thyrotropin releasing hormone (TRH) Stimulates TSH secretion by thyrotropes
3.Growth hormone releasing hormone (GHRH)
4.Prolactin releasing hormone (PRH)
Stimulates GH secretion by somatotropes
5.Gonadotropin releasing hormone (GnRH)
1.Growth hormone inhibitory hormone [GHIH=Somatostatin=SST]
Stimulates LH & FSH secretion by gonadotropes
2.Prolactin inhibiting hormone [PIH=dopamine] Inhibits PRL secretion
44
Stimulates Prolactin secretion by lactotropes
Inhibits GH secretion
Releasing=R & Inhibiting=I
Hypothalamic: Librins =L & Statins=S 44
Hormones of Hypothalamus…
45.
Location
Pituitarygland (AKA hypophysis) is a small gland (about the size of a pea)
Lies in the sella turcica, a bony cavity at the base of the brain Sphenoid bone [butterfly-shaped bone]
1cm in diameter & 4gm weight
Is Master gland
Connected to the HT by a stalk of tissue called the infundibulum (hypophysial stalk)
Physiologically, the pituitary gland is divided into 2 distinct portions:
1. Anterior pituitary (AKA adenohypophysis)
Glandular anterior lobe (has endocrine cell or secretory cells)
2. Posterior pituitary (neurohypophysisis an extension of hypothalamus or is a neural tissue)
Neuronal posterior lobe.
45
2.Pituitary gland
Anterior pituitary hormones& functions
Hormones Functions
GH Promotes growth & metabolism
PRL Promotes milk secretion, breast growth, & maintains lactation
ACTH Stimulates adrenal cortex to produce aldosterone & cortisol
TSH Stimulates the thyroid gland to synthesize & secret Calcitonin/ T3/T4/
[For Thermogenesis & metabolism]
LH Promotes ovulation, luteinization
Stimulates Leydig cells for testosterone secretion
FSH Stimulates growth & maturation of ova
Stimulates spermatogenesis
Stimulates secretion of estrogen
49
Cont’d
Pituitary gland…
50.
a. GH
b. Physiologicaleffect of GH
c. Disorders of GH
Hypo & hyper secretion of GH
50
Growth hormone (GH)
51.
Growth hormone (GH)…
a.Growth hormone (GH)
Is an anterior pituitary hormone
Also known as somatotropic hormone.
All the major anterior pituitary hormones, except GH, exert their principal effects
by stimulating target glands.
In contrast ‘GH’ exerts its effects directly on all or almost all tissues of the body.
=IGF-1
Fig. Effects of GH 51
Somatomedin-cIGF-1
IGF-1 Insulin like growth factor-1
52.
Growth hormone (GH)…
b.Physiologicaleffect of GH
Promotes protein deposition in tissues
Stimulates amino acid uptake & protein synthesis in muscle & other tissues.
Stimulates Cartilage & Bone Growth
Enhances [] Fat Utilization for Energy
Carbohydrate utilization
GH has hyperglycemic effect b/c of the beta cells of the islets of
Langerhans prone to degenerate because they become overactive owing to
the hyperglycemia.
Consequently, in about 10% of giants eventually develop diabetes mellitus [DM]
52
GH Hyperglycemic Hormone
53.
Cont’d
Metabolic role ofGH
On CHO metabolism
↓Glucose utilization
↑Gluconeogenesis ↑BGC ( Hyperglycaemic hormone)
↑Glycogenolysis
On protein metabolism (protein anabolic)
↑amino acid transport through the cell membrane
↑DNA transcription
↑RNA translation (protein synthesis)
↓Protein catabolism
On Fat metabolism
↑Lipolysis
↑FFA in plasma
↑Ketogenesis
↑β-oxidation
Other Roles of GH
↑RBC formation
↑Metabolic Rate, thermogenic
Insulin secretion (Diabetogenic effect of GH)
↑Secretion of Somatomedin-C (IGF)
On Electrolytes
↑Absorption of Na+, K+ & Ca2+
53
Growth hormone (GH)…
54.
Cont’d
C.Disorders (abnormalities ofGH secretion)
Hyposecretion
Dwarfism
Hypo-secretion (deficiency) of GH during childhood.
All the physical parts of the body develop inappropriate proportion to one another
Rate of development is greatly decreased.
This abnormality resulting in short limbs & short stature
54
54
Growth hormone (GH)…
55.
Cont’d
Hypersecretion: excessive GHsecretion
1. Gigantism (during active growth)
Caused by over-production of GH during childhood
Somatotrops become excessively active
Usually caused by a tumor on the pituitary gland of the brain (Tumor of
somatotrops)
All body tissues grow rapidly
It causes over growth of the hands, face, & feet
2. Acromegaly (after)
Results when the anterior pituitary gland produces excess GH after epiphyseal
plate closure at puberty (occurs after adolescence)
That means after the epiphyses of the long bones have fused with the shafts
The person cannot grow taller (no vertical growth), but the bones can become
thicker & internal soft tissues continue to grow
Enlargement of nose & ear due to excessive growth of cartilages
Prominent eye brow & face 55
55
Growth hormone (GH)…
56.
Acromegaly…
Marked enlargementin the bones of the:
Hands, jaw and feet
Cranium, nose, forehead, supraorbital ridges
Changes in the vertebrae - hunched back (kyphosis)
Projection of the lower jaw (prognathism)
Enlargement & broadening of hands & feet
56
56
57.
Is anteriorpituitary lactogenic hormone
Function of PRL
It Promotes growth & development of breast (mammary glands)
It Stimulates & maintains the secretion of milk (maintain lactation after parturition)
It Delays ovulation & suppresses fertility by inhibiting the action of LH & FSH.
57
Prolactin [PRL]
58.
3.Pineal gland [Alsocalled epiphysis]
Is located in the brain
A small, cone-shaped organ in the brain of vertebrates
Secretes the hormone melatonin (derived from serotonin)
Serotonin is precursor for melatonin
Formed from tryptophan
Melatonin is involved in:
Circadian rhythm (biorhythms)
Sleep & wake cycle [body clock = biological clock]
Seasonal breeding of animals (reproductive cycle)
58
Serotoninmelatonin
Pineal gland Is a tiny gland in the midbrain. It regulates mating behaviors & day-night cycles.
Pineal gland circadian rhythm & sleep induction. In animals it is known to play a major role in sexual development & seasonal breeding.
1.Thymus gland
Locatedin the mediastinum superior to the heart Behind the sternum & b/n
our lungs.
Unlike most organs, it is larger in children (it is only active until puberty).
After puberty, the thymus starts to shrink & become replaced by fat.
The thymus is the site of T cell differentiation, development & maturation.
T cells originate (born) in the bone marrow & soon after their born they migrate
to the thymus gland.
T-cells mature in the thymus gland & in the lymph nodes. Since the thymus is
only 10-15% functional in the adult, the lymph nodes take on greater
importance in the maturation process.
60
61.
Cont’d
Hormones inthe thymus stimulate the production, differentiation ,development ,
multiplication & maturation of disease-fighting T cells into different types.
Into:
T-Helper, regulatory, cytotoxic ,natural killer & memory T cells
The thymus gland produces (secrete) hormones like:
1.Thymopoietin
2.Thymosin
3.Thymulin
They regulate the development & later activation of disease fighting blood cells
called T lymphocytes.
61
Thymus gland…
62.
2.Gonads (ovaries &testes)
Gonads important for :
1.Gonadal cells development
Female ovum
Male sperm cells
2.Hormone secretion (sex hormones)
Female Estrogen & Progesterone
Male Testosterone
62
63.
1. Oogenesis formation& maturation of the egg
2. Hormonogenesis: Estrogen [E] & progesterone [P]
Control growth & development of female reproductive system or organ
Estrogen [E]
For egg maturation & for dev’t of 20 sexual characteristics
Body hair growth , narrow shoulder, broad hip, converging thigh.
Stimulates growth of breasts, particularly of the ductal part of breast.
↑Osteoblastic activity→↑rate bone growth
↑Bone matrix, ↑Ca2+ + Phosphate deposition inside bone.
Progesterone [P]
Thickens uterine lining or endometrium (Prepare the uterus to receive a fertilized egg)
Ovary for
64.
1. SpermatogenesisFormation &development of sperm or spermatozoa
2. Hormone → Testosterone
It regulates sperm cell production
It controls growth & development of male reproductive system
For dev’t Male secondary sexual characteristics
Stimulation of growth of pubic + Facial + axillary hair
Maintain sexual drive activity
64
Testes for
65.
Pancreas has2 major types of cells,
Acini produce pancreatic juices
Islets of Langerhans produce hormones
Islets contain 4 types of cells
1. Alpha Constituting about 25% of the total
Secretes glucagon
2. Beta Constituting about 60%
Lie mainly in the middle of each islet
Secrete insulin
3. Delta about 10% of the total
Secrete somatostatin [SS]
SS Has paracrine depressant effect on both insulin & glucagon secretion
4. PP cells present in small numbers in the islets
Secretes pancreatic polypeptide
A hormone of uncertain function 65
3.Endocrine pancreas
66.
Insulin and Itsmetabolic Effects
Affects carbohydrate , fat & protein metabolism
Effects of insulin on carbohydrate
Insulin is secreted in great quantity in response to high glucose concentration.
It increases cellular uptake of glucose
It causes glucose to be stored as glycogen mainly in the liver & muscles
Excess glucose that cannot be stored as glycogen are converted into fat,
Fat under the stimulus of insulin stored in the adipose tissue.
Insulin has a direct effect in promoting amino acid uptake by cells &
conversion of amino acids into protein
It inhibits breakdown of proteins 66
Effects of insulin on carbohydrate
Effects of insulin on Fat [adipose]
Effects of insulin on proteins
Endocrine pancreas…
Insulin and Its metabolic Effects
67.
Cont’d
Normal bloodglucose level (fasting level) is 70-110mg/dl of blood [90mg/dl]
When the blood [glucose] falls too low, into the range of 20-50mg/dl,
Symptoms of hypoglycemic shock develop,
Characterized by;
Progressive nervous irritability that leads to fainting, seizures, & even coma.
In the absence of insulin
Fat breakdown and use for providing energy are greatly enhanced.
This occurs even normally b/n meals when secretion of insulin is minimal,
But it becomes extreme in diabetes mellitus when secretion of insulin is almost zero.
The brain cells are permeable to glucose:
Use glucose as the only energy source without the intermediation of insulin
67
Insulin & Its metabolic Effects…
68.
Cont’d
Insulin isThe Only Hormone that Can Lower Blood Glucose
Muscle, fat & liver tissues require insulin to transport glucose into the cells;
In these tissues insulin the # of ‘GLUT2 transporter’ in the cell membrane
Many other tissues, like brain, do not require insulin to transport glucose
Insulin also activity of enzymes [glycogen synthase]that cause storage of sugar as glycogen or lipid
After a meal blood sugar rises stimulates the release of insulin;
Insulin then causes the sugar to enter the cells & Extra become stored as glycogen.
68
Insulin and Its metabolic Effects…
Several Hormones Can Raise Blood Glucose:
5 major hormones raise blood glucose are:
Glucagon, Cortisol, E(NE), GH & T3 & T4 [TH]
In vigorous exercise all of these hormones increase.
69.
Cont’d
Insulin secretionis associated with energy abundance.
When there is greater amount of energy-giving foods in the diet, especially
excess amounts of carbohydrates [CHOs], insulin is secreted in great quantity.
BCZ insulin plays an important role in storing this excess amount.
In the case of excess CHOs, Insulin causes them to be stored as glycogen
mainly in the liver & muscles.
Also, under the stimulus of insulin, excess CHOs converted into fats & stored
in the adipose tissue.
69
Insulin and Its metabolic Effects…
Glucagon issecreted by alpha () cells of the islets of Langerhans
When the blood [glucose] falls:
Diametrically oppose the function of insulin
Effects of glucagon on Metabolism
The major effects of glucagon on glucose metabolism are:
1. Breakdown of liver glycogen (glycogenolysis) to glucose
2. Increase gluconeogenesis in the liver
Both of these effects greatly enhance the glucose availability to the other organs of the body
And increase blood glucose concentration.
72
Glucagon and Its Functions
Effects of glucagon on Metabolism
73.
Is asyndrome of impaired carbohydrate, fat, & protein metabolism
Caused by:
Either lack of insulin secretion or
Decreased sensitivity of the tissues to insulin.
a. Type I diabetes, also called insulin-dependent diabetes mellitus (IDDM)
Is caused by sever, absolute lack of insulin secretion
Results from reduction in the cell mass
Due to autoimmune destruction of cells
Assumed to occur following an environmental trigger in genetically
susceptible individuals
Age of onset is <20 years, hence called juvenile onset DM
In type I diabetes, plasma insulin levels are very low or undetectable during fasting & even
after a meal.
There are 2 general types of DM:
Diabetes Mellitus (DM)
74.
b. Type IIdiabetes: non-insulin-dependent diabetes mellitus (NIDDM),
Age of onset usually > 30 years
Is caused by decreased sensitivity of target tissues to the metabolic effect of
insulin.
This reduced sensitivity to insulin is often called insulin resistance.
Is More common than type I
Is about 90% of all cases of DM.
Type II , in contrast to type I, is associated with increased plasma [insulin] hyperinsulinemia
The in insulin sensitivity weakens carbohydrate utilization & storage,
Raising blood glucose & stimulating a compensatory increase in insulin secretion.
74
There are 2 general types of DM…
75.
75
Classical featuresof DM
Glucose in the urine exerts osmotic gradient that draws water with it
Glucosuria
Polyuria & Polydipsia
B/c polyuria results in water loss thirst polydipsia
Polyphagia
B/c glucose is lost via urine causing high demand for fuel polyphagia
Muscle Wasting
To meet the challenge of high demand of fuel endogenous proteins are
catabolized into glucose.
This causes loss of muscle mass
Classical features of DM
Paresthesia
Poor wound healing
76.
76
1. For typeI DM administer enough insulin
2. In persons with type II DM, dieting & exercise are usually recommended
Weight loss will reverse the insulin resistance.
If this fails, drugs may be administered Metformin [Glucophage]
To increase insulin sensitivity (type 2)
Treatment of Diabetes
77.
1. Location
2. Cells
3.Hormones
4. Functions & metabolism
5. Disorders
Hypo & hyper secretion
Location:
Located immediately below the larynx on each sides anterior to the trachea
Has 2 lobes connected by thyroid tissue called isthmus
The largest endocrine gland
Is well vascularized has highest rates of blood flow per gram of tissue
Weighing 15 to 20 grams in adults
Hyoid bone
77
4.Thyroid gland
78.
Cells & Hormones
Have 2 secretary cells (many spherical sacs called thyroid follicles)
The interior of follicles contains a protein rich fluid called colloid.
The major constituent of colloid is thyroglobulin, which contains the thyroid hormones.
A. Follicular cells
Secretes 2 major hormones: thyroxine (T4) & triiodothyronine (T3)
in T4 &T3, the basal metabolic rate of the body to 60-100% above normal
B. Para follicular cells
Secrete Calcitonin regulates Ca2+ homeostasis
Which plasma Ca2+ concentration
bone Ca2+ (bone resorption)
78
2 secretary cells thyroid follicles (sacs) colloid thyroglobulin [TG] thyroid hormones
Cells & Hormones of [thyroid gland]
79.
Formation & secretionof thyroid hormones [TH]
Thyroid follicles accumulate iodide from blood & secrete into the colloid
Iodide oxidized to iodine & attached to amino acid tyrosine within
thyroglobulin
The attachment of 1 iodine to tyrosine produces monoiodotyrosine(MIT)
The attachment of 2 iodine to tyrosine produces diiodotyrosine(DIT)
MIT + DIT produces triiodothyronine (T3)
DIT + DIT produces tetraiodothyronine (T4) or thyroxine
T3 has 3 iodine atoms and T4 has 4 iodine atoms
Dietary iodine is essential for the normal production of TH
More T4 [93%] than T3 [7%] is secreted from thyroid cells 79
80.
On body metabolism& Energy formation
Cellular metabolic activities of almost all the tissues of the body.
The rate of cellular respiration
TH: basal metabolic rate (BMR)
Oxygen consumption
Number & activity of mitochondria
The rate of formation of ATP to energize cellular function
Heat production
The rate of utilization of foods for energy [Appetite]
On heart
Cardiac output & heart rate ( blood flow ,vasodilatation in most tissues)
Heart strength (force of contraction)
Sympathetic Effects
Pulmonary effects
The rate and depth of respiration.
Hematopoietic Effects:
Cellular demand for O2 leads to
Production of erythropoietin & RBC production (erythropoiesis).
Physiologic Functions of Thyroid hormone [TH]
80
81.
TH:Effects on Protein,Lipid & Carbohydrate Metabolism
On CHO metabolism
Glycogenolysis
Gluconeogenesis (Hyperglycemic effect)
Glucose absorption from the GIT
On protein metabolism
Transcription of large numbers of genes high protein synthesis [like GH]
On fat metabolism
Increase lipolysis (lipids mobilization)
81
82.
Required for:
Normal development & maturation of NS (brain) in the fetus & infants
Normal functioning of nervous system [NS] in adults
Normal body growth & development
Secretion of GH
82
Thyroid hormones [TH=T3 & T4]
Hypo &hyper secretion
Diseases of the thyroid can be primary or secondary in nature
1. Primary disease is one in which the gland itself is affected.
2. Secondary Disease is when the anterior pituitary or the hypothalamus is not
functioning properly.
Disorders of the Thyroid can be:
1. Thyroid gland enlargement
2. Hormone deficiency, or hypothyroidism
3. Hormone excess, or hyperthyroidism
Deficiency mentally retarded & physically slow [lethargic]
Low BMR, cold intolerant, lack of appetite
Excess restlessness, irritability, anxiety, insomnia
High BMR, heat intolerant 85
Disorders
Hypo & hyper secretion
86.
1.Hypothyroidism
thyroid hormones(T3 & T4)endemic goiter
Mechanism for dev’t of endemic colloid goiter
Iodine is a raw material for production of T3 & T4
Lack of iodine prevents production of both T3 & T4
No T3 & T4 to inhibit production of TSH
Secretion of excessively large quantities of TSH
TSH continuously stimulates thyroid cells [gland] to secrete TH,
The gland grows larger & larger
But because of lack of iodine, T3 & T4 production does not occur
Therefore no T3 & T4 normal negative feedback suppression of TSH production
Follicles become large in size, & thyroid gland may increase to 10-20x normal size
86
Iodine,T3,T4TSH endemic Goiter
1.Hypothyroidism
Mechanism for dev’t of Endemic colloid goiter
87.
Cretinism
Congenital abnormalextreme hypothyroidism during fetal life, infancy, or childhood
Characterized by failure of body growth (stunted growth, deformity) & mental retardation
Resulted from:
Inborn lack of thyroid gland or
Failure of the thyroid gland to produce thyroid hormone
Because of a genetic defect of the gland AKA congenital cretinism
Genetic defect of the gland,
Unless the cretinism is treated within a few weeks after birth,
Mental growth remains permanently retarded (mental handicap , disability)
Disordered Or a low metabolism.
Myxedema - extreme adult hypothyroidism [caused by decreased activity of the thyroid gland in adults]
Develops in the patient with almost total lack of thyroid hormone function.
Characterized by bagginess under the eyes & swelling of the face.
Swellings around the lips & nose, mental deterioration, & slow metabolism (BMR).
87
1.Hypothyroidism…
Myxedema:
• Low levels of thyroid hormone in adults, either due to: thyroid-gland removal,
lack of function, or atrophy, or secondary to a pituitary-gland disorder.
88.
Secretion ofhigh levels of thyroid hormones [T3 & T4=TH]
Symptoms of Hyperthyroidism:
A high state of excitability & ↑ HR
Intolerance to heat
Increased sweating
Nervousness or psychic disorders & inability to sleep
Etc.
88
2. Hyperthyroidism
89.
Hyperthyroidism (thyrotoxicosis,Graves' Disease Toxic Goiter)
Is excessive secretion of thyroid hormones (T3 & T4)
Characterized by an enlarged thyroid gland
Protrusion of the eyeballs, a rapid heartbeat, & nervous excitability.
Result in:
2-3 times normal size of the thyroid gland, with tremendous hyperplasia
The number of cells are increased greatly [T3 & T4]
Increased rate of thyroid hormone secretion [T3 & T4]
But plasma [TSH] is less than normal
2. Hyperthyroidism…
90.
Graves' diseaseaccountsfor about 80% of all cases of hyperthyroidism
In these patients there is immunoglobulin that have actions similar to TSH
It is called Thyroid-stimulating immunoglobulin (TSI)
Occur as a result of autoimmunity that has developed against thyroid tissue
TSI binds with the same receptors that bind with TSH
Induce continual activation of the follicular cells
This Results development of hyperthyroidism
TSI is not precisely subjected to negative feedback [unlike TSH]
i.e No negative feedback relationship b/n TH (T3 & T4) & TSI
90
T3,T4TSH ,but TSIToxic Goiter
2. Hyperthyroidism…
91.
Exophthalmos
Is protrusionof the eyeballs due to hyperthyroidism (thyrotoxicosis)
Occurs in most people with hyperthyroidism
Can be so severe that the eyeball protrusion stretches the optic nerve damage vision
Eyes damage can also be due to;
Eyelids do not close completely when the person blink or sleep
Epithelial surfaces of the eyes become dry , irritated & often infected,
Resulting in ulceration of the cornea of eye
91
OphthalmosEye
Exophthalmos
92.
Thyroid disorders
Hypersecretion Hyposecretion
HyperthyroidismHypothyroidism
1. Graves’ disease 1. Myxedema adult
2. Exophthalmos goitor 2. Cretinism fetal & infant
3. Goiter (toxic goiter)
4. Thyrotoxicosis
5. Protrusion of eye ball
3. Goiter (non-toxic goiter, endemic goiter)
4. Hashmoto’s disease
T4 T3
Thyroid gland synthesizes 93% of T4 Thyroid gland synthesizes 7% of T3
Not active Functionally Active
T4 Functionally active when liberate one iodine in target organ
tissue By iodinase enzyme to T3
Active
T3 Vs T4
92
93.
Location:
Located immediatelybehind the thyroid gland
6mm long, 3 mm wide & 2 mm thick
Difficult to locate during thyroid operations
Since they often look like just another lobule of the thyroid gland
Hormone:
The gland contains mainly chief cells & a small number of Oxyphil cells
Chief cells secrete parathyroid hormone [PTH]
Function of the Oxyphil cells is not certain,
But believed to be modified or depleted chief cells that no longer secrete hormone
93
5.Parathyroid gland
1. Bone :
It increases the movement of Ca2+ & phosphate from bone into ECF [Blood].
Stimulates osteoclasts & depresses osteoblasts
The net effect is ↑[Ca2+] in the plasma [blood]
2. Kidney :
↑Reabsorption of Ca2+ in the DT & CD BUT Reabsorption of phosphate
↑Formation of 1,25-dihydroxyvitamin D (1, 25 (OH)2 D3)
Role of 1, 25 (OH)2 D3
↑Release of Ca2+ from Bone,SI & Renal tubules to blood
3. Gut : ↑Absorption of Ca2+ & Phosphate in small intestine
The effects of PTH on 3 target tissues result in a higher Ca2+ blood concentration.
PTH: a hypercalcemic hormone 95
The major physiological effects of PTH on 3 Target organs
96.
Calcitonin
Secreted bythe parafollicular cells of the thyroid gland
Has effects opposite to that of PTH.
Calcitonin lowers the blood Ca2+ & phosphate levels.
Action: it is a hypocalcemic hormone (↓Ca2+ level in blood)
Target organs: bone, renal tubules & GIT
1. Effect of Calcitonin on renal tubules: ↓Reabsorption of Ca2+
2. Effect of Calcitonin on GIT: ↓Absorption & transport
3. Effect of Calcitonin on bone:
↓activities of osteoclasts
↓formation of new osteoclasts
↑activates osteoblasts 96
Net effect ↓ Ca2+ level in blood
97.
Calcium regulator hormones[3]
3 hormones are primarily concerned with the regulation of Ca2+ metabolism
1. 1,25-Dihydroxy-cholecalciferol [active form of vitamin-D] vitamin-D3
It increases Ca2+ absorption from the intestine
2. Parathyroid hormone [PTH]
Reabsorbs Ca2+ & increases urinary phosphate excretion.
3. Calcitonin
Inhibits bone resorption [Inhibits osteoclast activities]
Stimulates osteoblasts & bone calcification or formation.
97
97
98.
Excess PTHcauses rapid resorption of Ca2+ from bones hypercalcemia
Hypofunction of parathyroid glands Hypocalcemia
Often with resultant tetany [muscular spasms & tremors]
Hypoparathyroidism
Causes:
Autoimmune disease to the gland
Surgical removal of PTGs along with thyroid gland
During thyroidectomy or Para thyroidectomy
Congenital absence of the gland
Consequences:
↓Plasma Ca2+ level hypocalcemia
Among the muscles of the body especially sensitive to tetanic spasm are the laryngeal muscles
Spasm of these muscles obstruct respiration,
Is common cause of death in tetany unless appropriate treatment is applied
Disorders
98
Low PTH
99.
Hyperparathyroidism
1.Primary PTH excess(primary hyperparathyroidism)
Causes:
Due to parathyroid gland adenoma or hyperplasia
Leads to:
Bone resorption
Hypercalcemia
Kidney stones formation [Ca2+ Precipitate formation]
2.Secondary Hyperparathyroidism
High level of PTH occur as a compensation for hypocalcemia rather than as a
primary abnormality of the parathyroid glands
Caused by vitamin D deficiency or chronic renal disease
For example, damaged kidneys unable to produce sufficient amounts of active form
of vitamin D (due to chronic renal disease].
Disorders…
100.
Results fromCa2+ or phosphate deficiency in ECF
In which the bones soften ,bend & deformed caused by
An inadequate intake of vitamin-D &
Insufficient exposure to sunlight [lack of vitamin-D]
7-dehydrocholesterol in the skin by UV to vitamin-D3,
Activated vitamin D3 prevents rickets
By promoting Ca2+ & phosphate absorption from the intestines [GIT]
Children who remain indoors do not receive adequate quantities of vitamin-D
100
Osteomalaciasoftening of the bones a deficiency of vitamin D or Ca2+ .
RicketsVitamin-D Deficiency
Osteomalacia
Rickets
101.
Prolonged rickets compensatory increase in PTH secretion
Extreme resorption of bone (mobilization of Ca2+ from bone to blood)
Causes bone to become progressively weaker
Treatment of rickets
Supplying adequate Ca2+ & phosphate in the diet
Administering large amounts of vitamin-D
101
Rickets-Vitamin D Deficiency…
102.
PTH greatlyenhances both Ca2+ & phosphate absorption from the intestines
This is by increasing the formation of 1,25-dihydroxycholecalciferol from vitamin-D in the kidneys
7-dehydrocholesterol in the skin
UV light
Fig. Role of PTH in intestinal
absorption of Ca2+
102
PTH Increases Intestinal of Ca2+ & Phosphate Absorption
103.
6.Adrenal gland [AG]
Location
Suprarenal glands
Two adrenal glands,
Each of which weighs about 4 grams,
Placed at the superior poles of the two Kidneys suprarenal glands
Hormones
AG Composed of 2 distinct parts
1. adrenal medulla (inner] 20%)
Functionally related to the sympathetic nervous system [SNS]
Medulla secretes amine E & NE in response to sympathetic stimulation
These hormones cause almost the same effects as SNS in all parts of the body
2. adrenal cortex (outer zone)
Secretes steroid hormones collectively called corticosteroids (corticoids).
These hormones are all synthesized from the steroid cholesterol.
103
A. adrenal medulla
Hormones of Adrenal Medullary Hormones
Cells in the adrenal medulla synthesize & secrete,
Epinephrine &
Norepinephrine.
These hormones bind adrenergic receptors on target cells
They induce the same effects as sympathetic nervous stimulation.
Help the body to prepare for "fight-or-flight" reactions.
105
106.
Action of E& NE
1.On cardiovascular system
Heart (β1): ↑Inotropic activity (contractility)=contraction
↑Chronotropic activity (heart rate)=time
Blood vessels: α1-R = Vasoconstriction
2.On Respiratory system:
β2-R = Bronchodilation
3.On GIT: Inhibit GI activity
4.On CNS : ↑Mental alertnessLeads to nervousness in excess
106
107.
B. adrenal Cortex[AC]
Has 3 Distinct Layers
1. The zona glomerulosa
A thin outer layer
Secrets mineralocorticoids (aldosterone)
Essential to the maintenance of ‘minerals 'of the ECF (Na & K balance) & ECF volume
2. The zona fasciculata
Secrete the glucocorticoids (cortisol )
Are steroids & have effects on the metabolism of CHO ,fat & protein
3. The zona reticularis (Gonadocorticoids)
Are deeper layer of the cortex,
Secretes the adrenal androgens dehydroepiandrosterone (DHEA)
Exert minor effects on reproductive function.
Adrenocortical [AC] secretion is controlled primarily by ACTH from the anterior
pituitary.
107
108.
Cont’d
Corticosteroids from theadrenal cortex includes:
1. Mineralocorticoids
2. Glucocorticoids &
3. Gonadocorticoid [Adrenal androgens DHEAS]
Abnormalities of Adrenal gland Secretion
1. Cushing’s Syndrome hypersecretion of corticosteroids (cortisol)
2. Addison’s Disease hyposecretion of corticosteroids (cortisol & aldosterone)
3. Conn's syndromeexcess secretion of aldosteronedisturbances in salt-water
balance
4. Adreno-genital syndromehyposecrtion of adrenal androgen
5. Pheo-chromocytomais tumor of adrenal medulla which causes
hypersecretion of E & NEleads to Hypertension [BP]
108
109.
1.The zona glomerulosa
Functions,
These cells are responsible for secreting aldosterone [Aldo].
Aldosterone ↑ the reabsorption of Na+ & removal of K+ & H+ from the kidney tubules.
The secretion of these cells is controlled mainly by Ang II & K+
Both of them stimulate aldosterone secretion.
Hypersecretion of Aldo,
Excess aldosterone increases ECF volume & ABP
Cause a serious in the plasma K+ concentration hypokalemia.
Hyposecretion of Aldo,
If low , large amounts of salt (like NaCl) will lost in the urine.
It results in severe ECF depletion & low blood volume, leading to circulatory shock.
ECF K+ & H+ concentration can rise far above normal ,blood acidosis & hyperkalemia.
109
110.
4 factorsplay essential roles in the regulation of aldosterone.
Aldosterone secretion will when:
1. K+ concentration in the ECF
2. Angiotensin II
3. ACTH from the anterior pituitary gland &
4. Na ion conc/n in the ECF
110
Cont’d
111.
2. The zonareticularis (inner)
Hormone
Adrenal Androgens
It is male sex hormone.
It also exert mild effects in the female (responsible for sex drive )
Some of the adrenal androgens can converted to testosterone & estrogens.
Function of adrenal androgen [AA]:
Initiate the development of 2ry-sexual characteristics includes:
Enlargement of genital organs
Voice change
Growth of hairs in the axillary & Pubital areas
But the concentration of AA is so low & its effect is almost insignificant.
Androgen is high in the Testis.
111
2. The zona reticularis (inner)
112.
3.The zona fasciculata
Functions
Is the middle & widest layer,
Constitutes about 75 % of the adrenal cortex &
Secretes mainly cortisol but also lesser adrenal androgens & estrogens.
Secretion controlled by (ACTH) from the pituitary gland.
112
113.
1.On Carbohydrate Metabolism
1.Stimulation of Gluconeogenesis by the liver
2. Decreased Glucose Utilization by Cells.
Elevated Blood Glucose Concentration
Both the of its effects cause the blood glucose concentrations to rise.
This high levels of cortisol reduce the sensitivity of tissues to the
stimulatory effects of insulin on glucose uptake & utilization.
The condition is called adrenal diabetes.
113
Physiological effects cortisol
114.
Cortisol…
2. Effects ofCortisol on Protein Metabolism
Increased catabolism of protein (decreased protein synthesis)
Cortisol promotes amino acid mobilization from muscle.
3.Effects of Cortisol on Fat Metabolism
A. Mobilization of Fatty Acids [FA]
Cortisol promotes mobilization of FA from adipose tissue.
This increases the concentration of free FA in the plasma, which also
increases their utilization for energy.
B. Obesity Caused by Excess Cortisol.
Excess cortisol secretion develop abnormal type of obesity, with excess
deposition of fat in the chest & head regions of the body
Giving a buffalo-like torso (trunk, chest, upper body) & a rounded “moon face.”
114
115.
Cortisol…
4.Cortisol is Importantin Resisting Inflammation
It has anti-inflammatory effects [Anti-allergic Or Anti-stress]
It suppresses (block) inflammatory reactions by
Stabilizes lysosomal membrane
Inhibits formation of inflammatory mediators
5. Immunosuppressant action [side effect of cortisol]
Inhibits activation & proliferation of both T-lymphocytes & B-lymphocytes
Leads to a general depression of Immunity
115
• Cortisol :as anti-inflammatory , as Anti-allergic Or Anti-stress BUT it has side effects [depress our Immunity]
• Cortisol enhances synthesis & release of catecholamines
116.
Summary for theeffect of cortisol on metabolism
A. On CHO metabolism
↑Gluconeogenesis ↑BGC
↓Glucose utilization
B. On Protein metabolism D. Fat metabolism
↑Protein catabolism ↑Lipolysis
↓Protein synthesis ↑Mobilization of fat & deposition to unusual area
↓Amino acid uptake
C. Anti-inflammatory action [Anti-stress]
Regulation of Cortisol Secretion By:
a.ACTH
Stimulate Cortisol Secretion
b.Stress
Stress increase secretion of ACTH & Cortisol
116
↑BGC
{Hyperglycemia}
117.
Hypoadrenalism Addison’sDisease
Results from failure of the adrenal Cortex to produce aldosterone & cortisol.
Causes
Autoimmune problem or infection to the gland
Damage or surgical removal of the gland
117
Disorders
1.Hyposecretion
118.
Mineralocorticoid [aldosterone] deficiency
Lack of aldosterone secretion
Hyponatremia/Hypotension ,Hyperkalemia & plasma volume falls (ECF depleted)
CO decreases
Acidosis develops BCZ of failure of H ions excretion.
Glucocorticoid [cortisol] deficiency
Lack of cortisol secretion
Highly susceptible for different types of stress, & even a mild respiratory
infection can cause death.
Gonadocorticoid [Androgen] deficiency
Lack of androgen secretion
Fail secondary sexual characteristics (but insignificant effect)
118
Hypo-secretion…
![The Endocrine Physiology
[Lecturer,AAU]
[Feb ,2017 E.C]
1](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-1-320.jpg)
![The Endocrine Physiology
[Lecturer,AAU]
[Feb ,2017 E.C]
1](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/75/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-1-2048.jpg)
![Gland
1.Exocrine gland
2.Endocrine gland
Hormones
Functions
Comparison with Nervous system
Regulation of Hormonal secretion
Chemical classification of hormones based on:
1.Solubility
Lipophilic
Lipohobic
2.Synthetic origin
Amine ,Protein (polypeptide) ,Steroid
MOA
Site of synthesis [rER or sER] ,release, transport,
metabolism & excretion:
Endocrine basis of hormone disorders
Major endocrine glands & tissues
1.Central endocrine glands
1. Pineal gland
2. Hypothalamus
3. Pituitary (hypophysis) gland
2.Peripheral endocrine glands
1. Thyroid glands
2. Parathyroid glands
3. Adrenal (suprarenal) glands
4. Thymus gland
5. Part of pancreas (islet of Langerhans)
6. Gonads (reproductive glands)
1. Testis
2. Ovary
1.Adipose tissue (fat cell/tissue)=
2.Small intestine & Skin=
3.Stomach=
4.Kidney=
5.Heart=ANP
6.Liver =IGF (somatomedin-c)
Angiotensinogen
Thrombopoietin
2
Hormone
secretion
as
secondary
function
Learning Objectives](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-2-320.jpg)
![Terminologies
1. Target organ organ that has specific receptors to which the hormone [messenger] binds specifically.
2. Adeno- Gland
3. Hypophysis Pituitary Underneath growth
4. Adenohypophysis Glandular Pituitary gland [Anterior]
5. Neurohypophysis Neural pituitary gland [Posterior]
6. Neuroendocrine cells function as the nervous & endocrine systems (dual functions)
7. Hypophyseal portal system[HPS] Is the conduit that connects the brain to the anterior pituitary.
8. Largest gland thyroid gland
9. Love hormone oxytocin
10. Stress hormone cortisol
11. Master gland pituitary
12. 99% Ca2+ is stored inside bone
13. Seat of the soul pineal gland
14. Active form of thyroid hormone is T3
15. Hashimoto's disease autoimmune disorder of the thyroid gland
3](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-3-320.jpg)
![What is the Endocrine system?
It is a system of control ,communication & coordination of body functions
It uses chemical signals called hormones for cell to cell communication
Is a collection of ductless glands (endocrine glands) & specific cells that secrete
chemical messengers called hormone [H].
This chemical messenger is transported (circulated) within the body mostly
through blood.
It arrives at distant cells within specific target organs.
The target organs have cells possessing appropriate receptors for that H.
5](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-5-320.jpg)
![What are hormones [H]?
H are chemical messengers or signal molecules:
Synthesized by ductless endocrine cells
Released directly in to the blood stream
Act on target cells that have receptors for that hormone
Their action is slower & long-term.
6
Circadian rhythm:
• Is a biological processes occurring at 24-hr interval
• Is inherent cycle or a daily rhythmic activity cycle, based on 24-hr intervals, that is exhibited by many organisms.](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-6-320.jpg)
![Functions of hormones
1.Regulation of reproduction: gametogenesis, sexual desire, coitus, fertilization.[T,Estrogen,P]
2.Regulation of body growth & development [GH, T3 & T4]
3.Production, utilization & storage of energy [Insulin, T3 & T4]
4.Growth & development of brain [T3 & T4]
5.Response to stress or injury & infections [Cortisol,]
6.Energy metabolism [T3 & T4]
7.Homeostasis: maintenance of the internal environment in the body.
Water (fluid)-electrolyte balance=ADH ,Aldosterone
Regulation of ABP= Renin ,ADH & Aldostrone
Control of BT [T3&T4], emotion (NE)
Change in mass of bone [PTH,calcitonin,Estrogen], muscle [T] ,RBCs [T,ErtPO] & fat [Estrogen]
8.Circadian rhythm [Serotonin or melatonin]
A rhythmic activity cycle, based on 24-hrs interval](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-7-320.jpg)
![Hormone Functions…
Behavior [T,E,P]
Immune system
8
8](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-8-320.jpg)
![Cont‘d
2.Periodic variations in hormone secretion
Hormone secretion influenced by:
A. Seasonal change [serotonin]
B. Various stages of development [T,E] & aging [E],
C. The diurnal or daytime cycle & sleep cycle or at night or nocturnal.
E.g.
I. The secretion of GH increased during the early period of sleep but is reduced
during the later stages of sleep & at day time.
II. Some hormones more secreted in adolescence stage
III. LH surge at ovulation [around 14 day of 28 days]
12
Regulation of hormonal secretion…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-12-320.jpg)
![Chemical classification of hormones
Classification based on [Solubility & Synthetic origin]
A. Solubility
1.Lipophilic :(water insoluble=steroid H)
Are lipid hormone made from cholesterol & are fat soluble
Easily cross lipid bilayer part of target organ
Receptor location in cytoplasm or nucleus (intracellular)
No need of 2ndary messenger
2.Lipophobic:amino acid [aa] based hormone made up of aa
Either a single modified amino acid or a protein made up of 3-200aa
Are hydrophilic: amine & peptide hormones
NB:But thyroid hormones (amine) are water insoluble
Receptor locationon surface (on cell membrane)
Bind to a receptor protein on the surface of the target cell & produce
physiological change in the cell.
But need 2ndary messenger 13
Thyroid hormonesT3 & T4](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-13-320.jpg)
![B.Synthetic origin (derived from tyrosine , tryptophan,cholestrol)
3 general classes of hormones:
1.Protein & polypeptide hormones: amino acids linkage
2.Steroid hormones :synthesized from cholesterol in a series of rxns
3.Amine hormones :(derivatives of a single amino acid like tyrosine, tryptophan)
1. Derivatives of the amino acid Amine hormones
Are hormones derived from amino acids tyrosine or tryptophan
Their receptor found on cell surface BUT thyroid hormones in nucleus
Includes : hormones secreted by
Thyroid gland ((thyroxin (T4) & triiodothyronine (T3)) = (lipid soluble)
Adrenal medulla (epinephrine & norepinephrine)
Pineal gland (melatonin & serotonin)
Hypothalamus dopamine
14
Chemical classification of hormones…
Catecholamines (E,NE,Dopamine) hormones used as neurotransmitter [NT]](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-14-320.jpg)
![Cont’d
2.Proteins & polypeptides hormones
Made up of small to many amino acids
Their receptor found on cell surface
Includes : hormones secreted by
Anterior & posterior pituitary gland
Pancreas (insulin & glucagon)
Parathyroid gland (PTH)
Hypothalamic hormones but dopamine is
amine
3. Steroids hormones
These are lipids derived from cholesterol.
Their receptor found intracellular (in target
organ cytoplasm or nucleus)
Includes :hormones secreted by:
Adrenal cortex :(cortisol & aldosterone,
androgen)
Ovaries & Placenta :(estrogen &
progesterone)
Testes: (testosterone)
Vit-D3 [calcitriol]
15
Chemical classification of hormones…
T3 & T4 Tyrosine
Serotonin,melatoninTryptophan](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-15-320.jpg)
![Hormone class Components Example
Amine H
Catecholamine
Amine H
Thyroid hormones
• Amino acid with modified group
• Receptor location =on Plasma membrane [PM]
• Amino acid with modified group
• Receptor location =in nucleus
• NE,E,Dopamine,melatonin
• Serotonin [precursor of melatonin]
T3,T4
Peptide H • Chain of linked amino acids • Oxytocin
• ADH
• Insulin/glucagon
• PTH,GH etc.
Steroid H • Derived from the lipid cholesterol
• Can freely pass through PM
• Receptor location = in Cytoplasm or nucleus
• Testosterone (androgen)
• Progesterone, Estrogen
• Cortisol, aldosterone
• Vit-D
16
Chemical classification of hormones…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-16-320.jpg)
![Mechanisms of Action of Hormones
The first step of a hormone's action is to bind to specific receptors at the target cell [organ].
Cell that lack receptors for the hormones does not respond.
The locations of receptors for the different types of hormones are:
1. Receptors on the surface of the cell membrane.
Such receptors are specific mostly for the protein, peptide, & catecholamine hormones. &
Act through 20 messengers
20 messengers can be:
1. cAMP,DAG
2. cGMP
3. IP3 (inositol 1,4,5 triphosphate)
4. Ca2+ etc.
17](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-17-320.jpg)
![Hormone: synthesis, release ,
transport,metabolism & excretion
Site of synthesis :(in the cell, cell body or soma)
Protein/peptide hormones: in the rER
Steroid hormones: in the sER
Release: Exocytosis
Transport: hormones are transported in blood in two forms:
a. In the free form (dissolving in plasma)have short half life
b. In combination with plasma proteins (or carrier proteins :albumin & globulin).
Have long half life
Metabolism: metabolized in the liver or by target cells [organs]
Excretion: urine, feces, sweat
21](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-21-320.jpg)
![1.Over production of hormones
a.Gigantism (childhood),Acromegaly (adult )GH
b.Hyperthyroidism Grave’s disease (toxic goiter or exophthalmic goiter) [T3 &T4]
c.Cushing’s syndrome adrenal cortex (cortisol) "buffalo hump") "moon face")
d.Galactorhea prolactin [PRL]
e.Conn’s disease Aldosterone
2.Under production of hormones
a. Dwarfism GH
b. Hypothyroidism Cretinism, myxedema ,Goiter (endemic) & Hashimoto's disease [ T3 &T4]
c. Addison’s disease adrenal cortex [ cortisol & Aldosterone]
d. Diabetes mellitus (IDDM or Type 1-DM) Insulin
e. Diabetic insipidus Posterior pituitary ADH [alcohol]
f. Osteoporosis Estrogen (woman >45yrs) & calcitonin
3.Non-functional receptors for the Hormones
Target cells become insensitive to the hormone
Eg. Diabetes mellitus (NIDDM or type II)
22
Endocrine basis of hormone disorders
RicketsIn Children
Osteomalacia In Adult](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-22-320.jpg)
![The principal endocrine glands & endocrine tissues of the body
1. Hypothalamus
2. Pineal gland
3. Pituitary
4. Thyroid
5. Parathyroid
6. Thymus
7. Adrenal gland
8. Pancreas
9. Ovaries
10. Testes
1. HeartANP
2. KidneyErpo, vit-D (calcitriol),Rennin
3. StomachGastrin, Ghrelin [appetite]
4. Small intestine Motilin,Secretin,CCK, neuropeptide-Y,histamin
5. Adipose tissue (fat cell/tissue)Leptin [appetite]
6. Liver IGF (Somatomedin-c),Angiotensinogen ,Thrombopoietin
Endocrine tissues Or organs
23
Endocrine glands
23
Gonads](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-23-320.jpg)
![24
A. Central endocrine glandsincludes;
1. Hypothalamus
2. Pituitary gland (hypophysis)
3. Pineal gland melatonin amine hormone sleep & weak cycle
(as circadian rhythm or as body biological clock].
B. Peripheral endocrine glands includes:
1. Thyroid glands
2. Parathyroid glands
3. Thymus gland
4. Adrenal gland
5. Pancreas
6. Gonads (Ovaries & Testes)
Endocrine glands: divided in to 2; Central & Peripheral](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-24-320.jpg)
![ Location [HT]
HT is part of the diencephalons, which forms the floor & the lateral wall of the
3rd ventricle Or found just under the thalamus. Or
Found above the pituitary gland
It is extremely complex part of brain
It contains many regions (nuclei) with highly specialized functions
HT represents less than 1% of the brain mass, about 5gm (so small but so
important area of brain)
Regardless of its size, it plays most important roles in controlling homeostasis
It is the main brain structure involved in regulating hormonal levels in the body
26
Hypothalamus (HT)…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-26-320.jpg)
![ Functions,
Some functions of different parts or regions of HT:
Regulates temperature :(it gives response to cold & heat) for thermal regulation
It has hunger & satiety center if they damaged hyperphagia or starvation.
It has thirst center it regulates drinking
Regulate sexual behavior :(it has sex drive center)
Control circadian rhythms :(control sleep & wake cycle)
Control autonomic NS : (sympathetic vs parasympathetic regulation)
Endocrine function:(HT Releases or secrets hypothalamic releasing & inhibiting hormones)
In turn, those hormones {H} stimulate pituitary H secretion
Etc.[many]. 27
Hypothalamus (HT)...](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-27-320.jpg)
![ The pituitary gland [PG]: is connected to the hypothalamus by stalk like structure called infundibulm.
PG is divided into an anterior lobe (adenohypophysis) & posterior lobe (neurohypophsis).
So, HT exerts its effects on pituitary gland in 2 different ways:
A. Hypothalamo-neurohypophysial axis
B. Hypothalamo-adenohypophysial axis
Hypothalamus & Pituitary
29
29](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-29-320.jpg)
![Cont’d
Posterior pituitary: an outgrowth of the hypothalamus composed of neural tissue.
Hypothalamic neurons pass through the neural stalk & end in the posterior pituitary.
Neuroendocrine cells from 2 nuclei in hypothalamus synapse directly on to blood
vessels in posterior pituitary.
These 2 nuclei are:
Supraoptic nucleus (SON) = secrets ADH (5/6th =83% )
Paraventricular nucleus (PVN) = secrets Oxytocin (5/6th =83% )
30
A. Hypothalamo-neurohypophysial axis
Posterior Pituitary Gland [Neurohypophysis]
Is composed mainly of glial-like cells called pituicytes
It does not synthesize hormones, but
Store & secrete 2 hormones:
a. ADH also called ‘Vasopressin’
b. Oxytocin
ADH
Oxy](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-30-320.jpg)
![Cont’d
Hyposecretion of ADH:leads to
Diabetes insipidus=DI :can be neurogenic or nephrogenic
Is caused by deficiency of ADH or ADH receptor insensitivity in Nephron
Manifestation of DI: polyuria & polydipsia
Two types of DI
1. Neurogenic DI
Due to a genetic defect that blocks ADH production
The hypothalamo-hypophysary system is damaged by surgery or disease.
2. Renal [nephrogenic] DI
The renal tubule cells are insensitive to ADH
33
Hypothalamo-neurohypophysial axis…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-33-320.jpg)
![Cont’d
for parturition & lactation
Function
1.Facilitates transport of sperm in both males & females ductile system
2.Promotion of maternal behavior toward the neonate
In nonhuman mammals, injection of oxytocin induces maternal behavior
3.Induces uterus contraction [Parturition]
Stimulating contraction of the pregnant uterus
Especially toward the end of gestation
34
b.oxytocin
Hypothalamo-neurohypophysial axis…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-34-320.jpg)
![Cont’d
Special neurons [heterogeneous] in hypothalamus synthesize & secrete neurohormones:
a. Releasing hormones (Librins)
Increase the secretion of hormones from anterior pituitary
b. Inhibiting hormones (Statins)
Inhibit or decrease the secretion of hormones from anterior pituitary
These hormones are carried by hypothalamohypophysial portal vein into adenohypophysis
In the anterior pituitary, librins & statins act on the glandular cells
To control secretion of the anterior pituitary hormones
For each anterior pituitary hormone there is a releasing hormone
For some there is also an inhibiting hormone [GHIH & PRLIH]
36
B. Hypothalamo-adenohypophysial axis [HPA]](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-36-320.jpg)
![The Hypothalamo-anterior pituitary axis…
A complex communication system b/n the nervous system & the endocrine system.
1. Hypothalamus
2. Pituitary gland
3. Endocrine glands
37
Negative feedback from the primary target gland modulates the secretion of both
pituitary & hypothalamic hormones.
37
1
Hypothalamo-adenohypophysial axisThe Hypothalamo –anterior Pituitary Axis=HPA
[target gland]
1](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-37-320.jpg)
![ The adenohypophysis is connected to HT by a system of blood vessels called the adenohypophyseal portal system. But
The neurohypophsis is connected to HT by a bundle of nerve fibers, called hypothalmo-neurohypophyseal tract.
The anterior pituitary is regulated by hormones secreted by the hypothalamus. However
The posterior pituitary simply stores & releases hormones that are actually produced by the hypothalamus.
Secretion of pituitary is controlled by hypothalamus [HT]
38
Cont’d
2
The Hypothalamo-anterior pituitary axis…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-38-320.jpg)
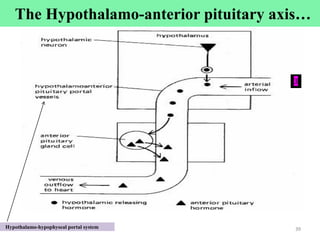
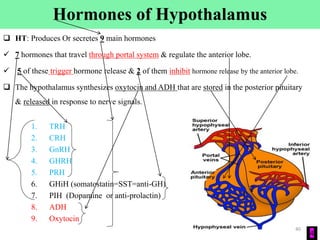
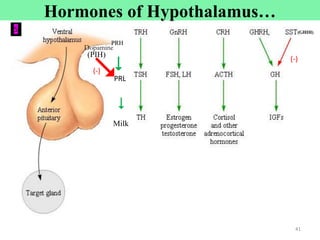
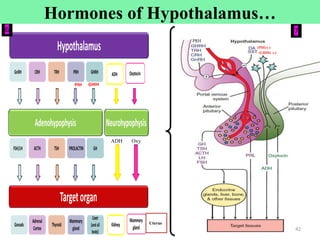
![Cont’d
Neuroendocrine cells in the hypothalamus:
Has axon tract [nerve] on pituitary glands (on both anterior (shorter) & posterior pituitary [longer])
8
Hormones of Hypothalamus…
[SON & PVN]
Heterogeneous [different types of] neurosecretory cells](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-43-320.jpg)
![L & S hormones that regulate the anterior pituitary (glandular cells)
Hypothalamic hormone Effect on pituitary
1.Corticotrophin releasing hormone (CRH) Stimulates ACTH secretion by corticotropes
2.Thyrotropin releasing hormone (TRH) Stimulates TSH secretion by thyrotropes
3.Growth hormone releasing hormone (GHRH)
4.Prolactin releasing hormone (PRH)
Stimulates GH secretion by somatotropes
5.Gonadotropin releasing hormone (GnRH)
1.Growth hormone inhibitory hormone [GHIH=Somatostatin=SST]
Stimulates LH & FSH secretion by gonadotropes
2.Prolactin inhibiting hormone [PIH=dopamine] Inhibits PRL secretion
44
Stimulates Prolactin secretion by lactotropes
Inhibits GH secretion
Releasing=R & Inhibiting=I
Hypothalamic: Librins =L & Statins=S 44
Hormones of Hypothalamus…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-44-320.jpg)
![ Location
Pituitary gland (AKA hypophysis) is a small gland (about the size of a pea)
Lies in the sella turcica, a bony cavity at the base of the brain Sphenoid bone [butterfly-shaped bone]
1cm in diameter & 4gm weight
Is Master gland
Connected to the HT by a stalk of tissue called the infundibulum (hypophysial stalk)
Physiologically, the pituitary gland is divided into 2 distinct portions:
1. Anterior pituitary (AKA adenohypophysis)
Glandular anterior lobe (has endocrine cell or secretory cells)
2. Posterior pituitary (neurohypophysisis an extension of hypothalamus or is a neural tissue)
Neuronal posterior lobe.
45
2.Pituitary gland](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-45-320.jpg)
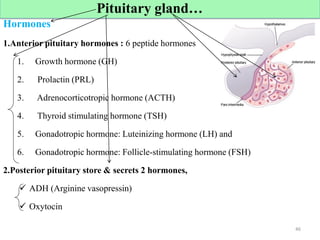
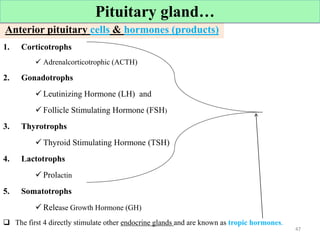
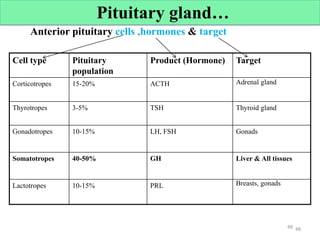
![Anterior pituitary hormones & functions
Hormones Functions
GH Promotes growth & metabolism
PRL Promotes milk secretion, breast growth, & maintains lactation
ACTH Stimulates adrenal cortex to produce aldosterone & cortisol
TSH Stimulates the thyroid gland to synthesize & secret Calcitonin/ T3/T4/
[For Thermogenesis & metabolism]
LH Promotes ovulation, luteinization
Stimulates Leydig cells for testosterone secretion
FSH Stimulates growth & maturation of ova
Stimulates spermatogenesis
Stimulates secretion of estrogen
49
Cont’d
Pituitary gland…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-49-320.jpg)
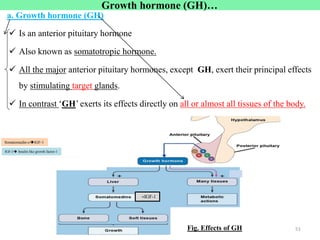
![Growth hormone (GH)…
b.Physiological effect of GH
Promotes protein deposition in tissues
Stimulates amino acid uptake & protein synthesis in muscle & other tissues.
Stimulates Cartilage & Bone Growth
Enhances [] Fat Utilization for Energy
Carbohydrate utilization
GH has hyperglycemic effect b/c of the beta cells of the islets of
Langerhans prone to degenerate because they become overactive owing to
the hyperglycemia.
Consequently, in about 10% of giants eventually develop diabetes mellitus [DM]
52
GH Hyperglycemic Hormone](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-52-320.jpg)
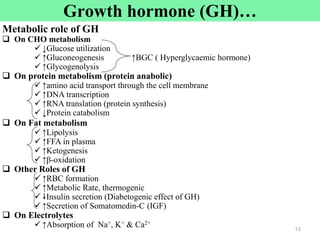
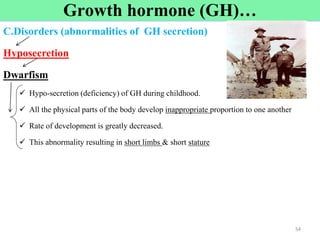
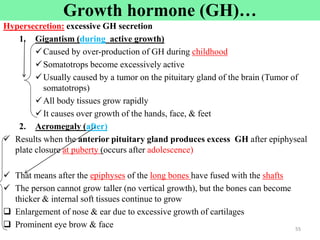
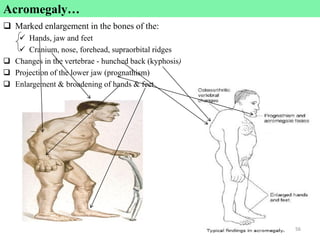
![ Is anterior pituitary lactogenic hormone
Function of PRL
It Promotes growth & development of breast (mammary glands)
It Stimulates & maintains the secretion of milk (maintain lactation after parturition)
It Delays ovulation & suppresses fertility by inhibiting the action of LH & FSH.
57
Prolactin [PRL]](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-57-320.jpg)
![3.Pineal gland [Also called epiphysis]
Is located in the brain
A small, cone-shaped organ in the brain of vertebrates
Secretes the hormone melatonin (derived from serotonin)
Serotonin is precursor for melatonin
Formed from tryptophan
Melatonin is involved in:
Circadian rhythm (biorhythms)
Sleep & wake cycle [body clock = biological clock]
Seasonal breeding of animals (reproductive cycle)
58
Serotoninmelatonin
Pineal gland Is a tiny gland in the midbrain. It regulates mating behaviors & day-night cycles.
Pineal gland circadian rhythm & sleep induction. In animals it is known to play a major role in sexual development & seasonal breeding.](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-58-320.jpg)
![Peripheral Endocrine glands-include
1. Thyroid glands
2. Parathyroid glands
3. Thymus gland
4. Adrenal gland [add + renal]
5. Pancreas
6. Gonads [sex organs= reproductive organs]
59](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-59-320.jpg)
![1. Oogenesis formation & maturation of the egg
2. Hormonogenesis: Estrogen [E] & progesterone [P]
Control growth & development of female reproductive system or organ
Estrogen [E]
For egg maturation & for dev’t of 20 sexual characteristics
Body hair growth , narrow shoulder, broad hip, converging thigh.
Stimulates growth of breasts, particularly of the ductal part of breast.
↑Osteoblastic activity→↑rate bone growth
↑Bone matrix, ↑Ca2+ + Phosphate deposition inside bone.
Progesterone [P]
Thickens uterine lining or endometrium (Prepare the uterus to receive a fertilized egg)
Ovary for](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-63-320.jpg)
![ Pancreas has 2 major types of cells,
Acini produce pancreatic juices
Islets of Langerhans produce hormones
Islets contain 4 types of cells
1. Alpha Constituting about 25% of the total
Secretes glucagon
2. Beta Constituting about 60%
Lie mainly in the middle of each islet
Secrete insulin
3. Delta about 10% of the total
Secrete somatostatin [SS]
SS Has paracrine depressant effect on both insulin & glucagon secretion
4. PP cells present in small numbers in the islets
Secretes pancreatic polypeptide
A hormone of uncertain function 65
3.Endocrine pancreas](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-65-320.jpg)
![Insulin and Its metabolic Effects
Affects carbohydrate , fat & protein metabolism
Effects of insulin on carbohydrate
Insulin is secreted in great quantity in response to high glucose concentration.
It increases cellular uptake of glucose
It causes glucose to be stored as glycogen mainly in the liver & muscles
Excess glucose that cannot be stored as glycogen are converted into fat,
Fat under the stimulus of insulin stored in the adipose tissue.
Insulin has a direct effect in promoting amino acid uptake by cells &
conversion of amino acids into protein
It inhibits breakdown of proteins 66
Effects of insulin on carbohydrate
Effects of insulin on Fat [adipose]
Effects of insulin on proteins
Endocrine pancreas…
Insulin and Its metabolic Effects](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-66-320.jpg)
![Cont’d
Normal blood glucose level (fasting level) is 70-110mg/dl of blood [90mg/dl]
When the blood [glucose] falls too low, into the range of 20-50mg/dl,
Symptoms of hypoglycemic shock develop,
Characterized by;
Progressive nervous irritability that leads to fainting, seizures, & even coma.
In the absence of insulin
Fat breakdown and use for providing energy are greatly enhanced.
This occurs even normally b/n meals when secretion of insulin is minimal,
But it becomes extreme in diabetes mellitus when secretion of insulin is almost zero.
The brain cells are permeable to glucose:
Use glucose as the only energy source without the intermediation of insulin
67
Insulin & Its metabolic Effects…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-67-320.jpg)
![Cont’d
Insulin is The Only Hormone that Can Lower Blood Glucose
Muscle, fat & liver tissues require insulin to transport glucose into the cells;
In these tissues insulin the # of ‘GLUT2 transporter’ in the cell membrane
Many other tissues, like brain, do not require insulin to transport glucose
Insulin also activity of enzymes [glycogen synthase]that cause storage of sugar as glycogen or lipid
After a meal blood sugar rises stimulates the release of insulin;
Insulin then causes the sugar to enter the cells & Extra become stored as glycogen.
68
Insulin and Its metabolic Effects…
Several Hormones Can Raise Blood Glucose:
5 major hormones raise blood glucose are:
Glucagon, Cortisol, E(NE), GH & T3 & T4 [TH]
In vigorous exercise all of these hormones increase.](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-68-320.jpg)
![Cont’d
Insulin secretion is associated with energy abundance.
When there is greater amount of energy-giving foods in the diet, especially
excess amounts of carbohydrates [CHOs], insulin is secreted in great quantity.
BCZ insulin plays an important role in storing this excess amount.
In the case of excess CHOs, Insulin causes them to be stored as glycogen
mainly in the liver & muscles.
Also, under the stimulus of insulin, excess CHOs converted into fats & stored
in the adipose tissue.
69
Insulin and Its metabolic Effects…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-69-320.jpg)
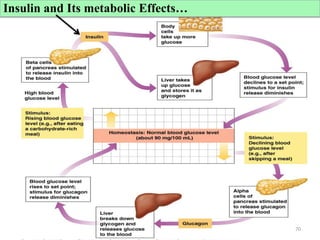
![Factors Affecting Insulin Secretion
Increase insulin secretion Decrease insulin secretion
• Increase blood glucose
• Increase blood free fatty acids & amino
acids
• Insulin resistant state
• Glucagon ,cortisol,GH,TH,E & NE
• Decrease blood glucose
• Fasting
• Somatostatin [SST]
71](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-71-320.jpg)
![ Glucagon is secreted by alpha () cells of the islets of Langerhans
When the blood [glucose] falls:
Diametrically oppose the function of insulin
Effects of glucagon on Metabolism
The major effects of glucagon on glucose metabolism are:
1. Breakdown of liver glycogen (glycogenolysis) to glucose
2. Increase gluconeogenesis in the liver
Both of these effects greatly enhance the glucose availability to the other organs of the body
And increase blood glucose concentration.
72
Glucagon and Its Functions
Effects of glucagon on Metabolism](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-72-320.jpg)
![b. Type II diabetes: non-insulin-dependent diabetes mellitus (NIDDM),
Age of onset usually > 30 years
Is caused by decreased sensitivity of target tissues to the metabolic effect of
insulin.
This reduced sensitivity to insulin is often called insulin resistance.
Is More common than type I
Is about 90% of all cases of DM.
Type II , in contrast to type I, is associated with increased plasma [insulin] hyperinsulinemia
The in insulin sensitivity weakens carbohydrate utilization & storage,
Raising blood glucose & stimulating a compensatory increase in insulin secretion.
74
There are 2 general types of DM…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-74-320.jpg)
![76
1. For type I DM administer enough insulin
2. In persons with type II DM, dieting & exercise are usually recommended
Weight loss will reverse the insulin resistance.
If this fails, drugs may be administered Metformin [Glucophage]
To increase insulin sensitivity (type 2)
Treatment of Diabetes](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-76-320.jpg)
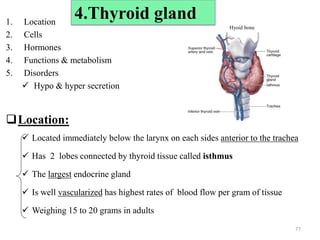
![Cells & Hormones
Have 2 secretary cells (many spherical sacs called thyroid follicles)
The interior of follicles contains a protein rich fluid called colloid.
The major constituent of colloid is thyroglobulin, which contains the thyroid hormones.
A. Follicular cells
Secretes 2 major hormones: thyroxine (T4) & triiodothyronine (T3)
in T4 &T3, the basal metabolic rate of the body to 60-100% above normal
B. Para follicular cells
Secrete Calcitonin regulates Ca2+ homeostasis
Which plasma Ca2+ concentration
bone Ca2+ (bone resorption)
78
2 secretary cells thyroid follicles (sacs) colloid thyroglobulin [TG] thyroid hormones
Cells & Hormones of [thyroid gland]](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-78-320.jpg)
![Formation & secretion of thyroid hormones [TH]
Thyroid follicles accumulate iodide from blood & secrete into the colloid
Iodide oxidized to iodine & attached to amino acid tyrosine within
thyroglobulin
The attachment of 1 iodine to tyrosine produces monoiodotyrosine(MIT)
The attachment of 2 iodine to tyrosine produces diiodotyrosine(DIT)
MIT + DIT produces triiodothyronine (T3)
DIT + DIT produces tetraiodothyronine (T4) or thyroxine
T3 has 3 iodine atoms and T4 has 4 iodine atoms
Dietary iodine is essential for the normal production of TH
More T4 [93%] than T3 [7%] is secreted from thyroid cells 79](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-79-320.jpg)
![On body metabolism & Energy formation
Cellular metabolic activities of almost all the tissues of the body.
The rate of cellular respiration
TH: basal metabolic rate (BMR)
Oxygen consumption
Number & activity of mitochondria
The rate of formation of ATP to energize cellular function
Heat production
The rate of utilization of foods for energy [Appetite]
On heart
Cardiac output & heart rate ( blood flow ,vasodilatation in most tissues)
Heart strength (force of contraction)
Sympathetic Effects
Pulmonary effects
The rate and depth of respiration.
Hematopoietic Effects:
Cellular demand for O2 leads to
Production of erythropoietin & RBC production (erythropoiesis).
Physiologic Functions of Thyroid hormone [TH]
80](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-80-320.jpg)
![TH:Effects on Protein, Lipid & Carbohydrate Metabolism
On CHO metabolism
Glycogenolysis
Gluconeogenesis (Hyperglycemic effect)
Glucose absorption from the GIT
On protein metabolism
Transcription of large numbers of genes high protein synthesis [like GH]
On fat metabolism
Increase lipolysis (lipids mobilization)
81](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-81-320.jpg)
![ Required for:
Normal development & maturation of NS (brain) in the fetus & infants
Normal functioning of nervous system [NS] in adults
Normal body growth & development
Secretion of GH
82
Thyroid hormones [TH=T3 & T4]](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-82-320.jpg)
![83
Thyroid hormones [TH]](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-83-320.jpg)
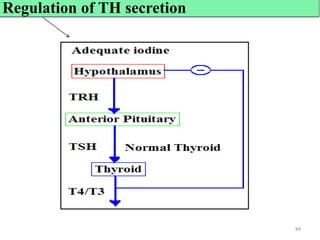
![ Hypo & hyper secretion
Diseases of the thyroid can be primary or secondary in nature
1. Primary disease is one in which the gland itself is affected.
2. Secondary Disease is when the anterior pituitary or the hypothalamus is not
functioning properly.
Disorders of the Thyroid can be:
1. Thyroid gland enlargement
2. Hormone deficiency, or hypothyroidism
3. Hormone excess, or hyperthyroidism
Deficiency mentally retarded & physically slow [lethargic]
Low BMR, cold intolerant, lack of appetite
Excess restlessness, irritability, anxiety, insomnia
High BMR, heat intolerant 85
Disorders
Hypo & hyper secretion](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-85-320.jpg)
![1.Hypothyroidism
thyroid hormones (T3 & T4)endemic goiter
Mechanism for dev’t of endemic colloid goiter
Iodine is a raw material for production of T3 & T4
Lack of iodine prevents production of both T3 & T4
No T3 & T4 to inhibit production of TSH
Secretion of excessively large quantities of TSH
TSH continuously stimulates thyroid cells [gland] to secrete TH,
The gland grows larger & larger
But because of lack of iodine, T3 & T4 production does not occur
Therefore no T3 & T4 normal negative feedback suppression of TSH production
Follicles become large in size, & thyroid gland may increase to 10-20x normal size
86
Iodine,T3,T4TSH endemic Goiter
1.Hypothyroidism
Mechanism for dev’t of Endemic colloid goiter](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-86-320.jpg)
![Cretinism
Congenital abnormal extreme hypothyroidism during fetal life, infancy, or childhood
Characterized by failure of body growth (stunted growth, deformity) & mental retardation
Resulted from:
Inborn lack of thyroid gland or
Failure of the thyroid gland to produce thyroid hormone
Because of a genetic defect of the gland AKA congenital cretinism
Genetic defect of the gland,
Unless the cretinism is treated within a few weeks after birth,
Mental growth remains permanently retarded (mental handicap , disability)
Disordered Or a low metabolism.
Myxedema - extreme adult hypothyroidism [caused by decreased activity of the thyroid gland in adults]
Develops in the patient with almost total lack of thyroid hormone function.
Characterized by bagginess under the eyes & swelling of the face.
Swellings around the lips & nose, mental deterioration, & slow metabolism (BMR).
87
1.Hypothyroidism…
Myxedema:
• Low levels of thyroid hormone in adults, either due to: thyroid-gland removal,
lack of function, or atrophy, or secondary to a pituitary-gland disorder.](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-87-320.jpg)
![ Secretion of high levels of thyroid hormones [T3 & T4=TH]
Symptoms of Hyperthyroidism:
A high state of excitability & ↑ HR
Intolerance to heat
Increased sweating
Nervousness or psychic disorders & inability to sleep
Etc.
88
2. Hyperthyroidism](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-88-320.jpg)
![ Hyperthyroidism (thyrotoxicosis, Graves' Disease Toxic Goiter)
Is excessive secretion of thyroid hormones (T3 & T4)
Characterized by an enlarged thyroid gland
Protrusion of the eyeballs, a rapid heartbeat, & nervous excitability.
Result in:
2-3 times normal size of the thyroid gland, with tremendous hyperplasia
The number of cells are increased greatly [T3 & T4]
Increased rate of thyroid hormone secretion [T3 & T4]
But plasma [TSH] is less than normal
2. Hyperthyroidism…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-89-320.jpg)
![ Graves' diseaseaccounts for about 80% of all cases of hyperthyroidism
In these patients there is immunoglobulin that have actions similar to TSH
It is called Thyroid-stimulating immunoglobulin (TSI)
Occur as a result of autoimmunity that has developed against thyroid tissue
TSI binds with the same receptors that bind with TSH
Induce continual activation of the follicular cells
This Results development of hyperthyroidism
TSI is not precisely subjected to negative feedback [unlike TSH]
i.e No negative feedback relationship b/n TH (T3 & T4) & TSI
90
T3,T4TSH ,but TSIToxic Goiter
2. Hyperthyroidism…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-90-320.jpg)
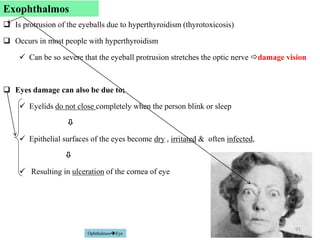
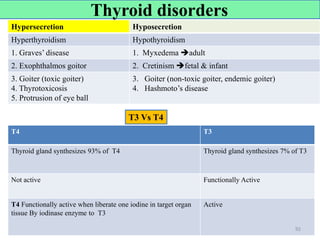
![ Location:
Located immediately behind the thyroid gland
6mm long, 3 mm wide & 2 mm thick
Difficult to locate during thyroid operations
Since they often look like just another lobule of the thyroid gland
Hormone:
The gland contains mainly chief cells & a small number of Oxyphil cells
Chief cells secrete parathyroid hormone [PTH]
Function of the Oxyphil cells is not certain,
But believed to be modified or depleted chief cells that no longer secrete hormone
93
5.Parathyroid gland](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-93-320.jpg)
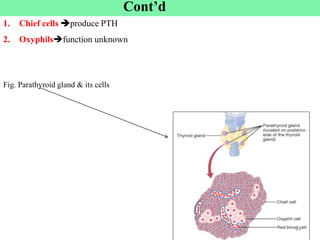
![1. Bone :
It increases the movement of Ca2+ & phosphate from bone into ECF [Blood].
Stimulates osteoclasts & depresses osteoblasts
The net effect is ↑[Ca2+] in the plasma [blood]
2. Kidney :
↑Reabsorption of Ca2+ in the DT & CD BUT Reabsorption of phosphate
↑Formation of 1,25-dihydroxyvitamin D (1, 25 (OH)2 D3)
Role of 1, 25 (OH)2 D3
↑Release of Ca2+ from Bone,SI & Renal tubules to blood
3. Gut : ↑Absorption of Ca2+ & Phosphate in small intestine
The effects of PTH on 3 target tissues result in a higher Ca2+ blood concentration.
PTH: a hypercalcemic hormone 95
The major physiological effects of PTH on 3 Target organs](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-95-320.jpg)
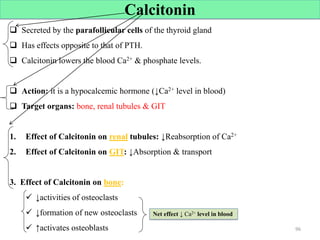
![Calcium regulator hormones [3]
3 hormones are primarily concerned with the regulation of Ca2+ metabolism
1. 1,25-Dihydroxy-cholecalciferol [active form of vitamin-D] vitamin-D3
It increases Ca2+ absorption from the intestine
2. Parathyroid hormone [PTH]
Reabsorbs Ca2+ & increases urinary phosphate excretion.
3. Calcitonin
Inhibits bone resorption [Inhibits osteoclast activities]
Stimulates osteoblasts & bone calcification or formation.
97
97](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-97-320.jpg)
![ Excess PTH causes rapid resorption of Ca2+ from bones hypercalcemia
Hypofunction of parathyroid glands Hypocalcemia
Often with resultant tetany [muscular spasms & tremors]
Hypoparathyroidism
Causes:
Autoimmune disease to the gland
Surgical removal of PTGs along with thyroid gland
During thyroidectomy or Para thyroidectomy
Congenital absence of the gland
Consequences:
↓Plasma Ca2+ level hypocalcemia
Among the muscles of the body especially sensitive to tetanic spasm are the laryngeal muscles
Spasm of these muscles obstruct respiration,
Is common cause of death in tetany unless appropriate treatment is applied
Disorders
98
Low PTH](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-98-320.jpg)
![Hyperparathyroidism
1.Primary PTH excess (primary hyperparathyroidism)
Causes:
Due to parathyroid gland adenoma or hyperplasia
Leads to:
Bone resorption
Hypercalcemia
Kidney stones formation [Ca2+ Precipitate formation]
2.Secondary Hyperparathyroidism
High level of PTH occur as a compensation for hypocalcemia rather than as a
primary abnormality of the parathyroid glands
Caused by vitamin D deficiency or chronic renal disease
For example, damaged kidneys unable to produce sufficient amounts of active form
of vitamin D (due to chronic renal disease].
Disorders…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-99-320.jpg)
![ Results from Ca2+ or phosphate deficiency in ECF
In which the bones soften ,bend & deformed caused by
An inadequate intake of vitamin-D &
Insufficient exposure to sunlight [lack of vitamin-D]
7-dehydrocholesterol in the skin by UV to vitamin-D3,
Activated vitamin D3 prevents rickets
By promoting Ca2+ & phosphate absorption from the intestines [GIT]
Children who remain indoors do not receive adequate quantities of vitamin-D
100
Osteomalaciasoftening of the bones a deficiency of vitamin D or Ca2+ .
RicketsVitamin-D Deficiency
Osteomalacia
Rickets](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-100-320.jpg)
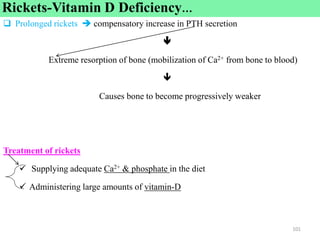
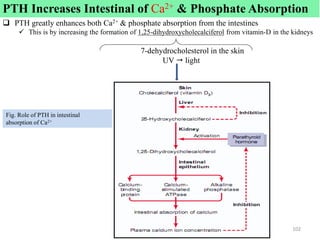
![6.Adrenal gland [AG]
Location
Suprarenal glands
Two adrenal glands,
Each of which weighs about 4 grams,
Placed at the superior poles of the two Kidneys suprarenal glands
Hormones
AG Composed of 2 distinct parts
1. adrenal medulla (inner] 20%)
Functionally related to the sympathetic nervous system [SNS]
Medulla secretes amine E & NE in response to sympathetic stimulation
These hormones cause almost the same effects as SNS in all parts of the body
2. adrenal cortex (outer zone)
Secretes steroid hormones collectively called corticosteroids (corticoids).
These hormones are all synthesized from the steroid cholesterol.
103](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-103-320.jpg)
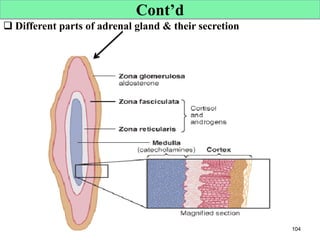
![B. adrenal Cortex [AC]
Has 3 Distinct Layers
1. The zona glomerulosa
A thin outer layer
Secrets mineralocorticoids (aldosterone)
Essential to the maintenance of ‘minerals 'of the ECF (Na & K balance) & ECF volume
2. The zona fasciculata
Secrete the glucocorticoids (cortisol )
Are steroids & have effects on the metabolism of CHO ,fat & protein
3. The zona reticularis (Gonadocorticoids)
Are deeper layer of the cortex,
Secretes the adrenal androgens dehydroepiandrosterone (DHEA)
Exert minor effects on reproductive function.
Adrenocortical [AC] secretion is controlled primarily by ACTH from the anterior
pituitary.
107](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-107-320.jpg)
![Cont’d
Corticosteroids from the adrenal cortex includes:
1. Mineralocorticoids
2. Glucocorticoids &
3. Gonadocorticoid [Adrenal androgens DHEAS]
Abnormalities of Adrenal gland Secretion
1. Cushing’s Syndrome hypersecretion of corticosteroids (cortisol)
2. Addison’s Disease hyposecretion of corticosteroids (cortisol & aldosterone)
3. Conn's syndromeexcess secretion of aldosteronedisturbances in salt-water
balance
4. Adreno-genital syndromehyposecrtion of adrenal androgen
5. Pheo-chromocytomais tumor of adrenal medulla which causes
hypersecretion of E & NEleads to Hypertension [BP]
108](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-108-320.jpg)
![1.The zona glomerulosa
Functions,
These cells are responsible for secreting aldosterone [Aldo].
Aldosterone ↑ the reabsorption of Na+ & removal of K+ & H+ from the kidney tubules.
The secretion of these cells is controlled mainly by Ang II & K+
Both of them stimulate aldosterone secretion.
Hypersecretion of Aldo,
Excess aldosterone increases ECF volume & ABP
Cause a serious in the plasma K+ concentration hypokalemia.
Hyposecretion of Aldo,
If low , large amounts of salt (like NaCl) will lost in the urine.
It results in severe ECF depletion & low blood volume, leading to circulatory shock.
ECF K+ & H+ concentration can rise far above normal ,blood acidosis & hyperkalemia.
109](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-109-320.jpg)
![2. The zona reticularis (inner)
Hormone
Adrenal Androgens
It is male sex hormone.
It also exert mild effects in the female (responsible for sex drive )
Some of the adrenal androgens can converted to testosterone & estrogens.
Function of adrenal androgen [AA]:
Initiate the development of 2ry-sexual characteristics includes:
Enlargement of genital organs
Voice change
Growth of hairs in the axillary & Pubital areas
But the concentration of AA is so low & its effect is almost insignificant.
Androgen is high in the Testis.
111
2. The zona reticularis (inner)](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-111-320.jpg)
![Cortisol…
2. Effects of Cortisol on Protein Metabolism
Increased catabolism of protein (decreased protein synthesis)
Cortisol promotes amino acid mobilization from muscle.
3.Effects of Cortisol on Fat Metabolism
A. Mobilization of Fatty Acids [FA]
Cortisol promotes mobilization of FA from adipose tissue.
This increases the concentration of free FA in the plasma, which also
increases their utilization for energy.
B. Obesity Caused by Excess Cortisol.
Excess cortisol secretion develop abnormal type of obesity, with excess
deposition of fat in the chest & head regions of the body
Giving a buffalo-like torso (trunk, chest, upper body) & a rounded “moon face.”
114](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-114-320.jpg)
![Cortisol…
4.Cortisol is Important in Resisting Inflammation
It has anti-inflammatory effects [Anti-allergic Or Anti-stress]
It suppresses (block) inflammatory reactions by
Stabilizes lysosomal membrane
Inhibits formation of inflammatory mediators
5. Immunosuppressant action [side effect of cortisol]
Inhibits activation & proliferation of both T-lymphocytes & B-lymphocytes
Leads to a general depression of Immunity
115
• Cortisol :as anti-inflammatory , as Anti-allergic Or Anti-stress BUT it has side effects [depress our Immunity]
• Cortisol enhances synthesis & release of catecholamines](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-115-320.jpg)
![Summary for the effect of cortisol on metabolism
A. On CHO metabolism
↑Gluconeogenesis ↑BGC
↓Glucose utilization
B. On Protein metabolism D. Fat metabolism
↑Protein catabolism ↑Lipolysis
↓Protein synthesis ↑Mobilization of fat & deposition to unusual area
↓Amino acid uptake
C. Anti-inflammatory action [Anti-stress]
Regulation of Cortisol Secretion By:
a.ACTH
Stimulate Cortisol Secretion
b.Stress
Stress increase secretion of ACTH & Cortisol
116
↑BGC
{Hyperglycemia}](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-116-320.jpg)
![Mineralocorticoid [aldosterone] deficiency
Lack of aldosterone secretion
Hyponatremia/Hypotension ,Hyperkalemia & plasma volume falls (ECF depleted)
CO decreases
Acidosis develops BCZ of failure of H ions excretion.
Glucocorticoid [cortisol] deficiency
Lack of cortisol secretion
Highly susceptible for different types of stress, & even a mild respiratory
infection can cause death.
Gonadocorticoid [Androgen] deficiency
Lack of androgen secretion
Fail secondary sexual characteristics (but insignificant effect)
118
Hypo-secretion…](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-118-320.jpg)
![HyperadrenalismCushing’s Syndrome
Hypersecretion of glucocorticoids (cortisol)
Clinical features of Cushing’s disease
Obesity: moon face, buffalo hump (torso), trunkal obesity (enlarged abdomen)
Hyperglycemia: adrenal diabetes mellitus [DM]
Poor (delayed) wound healing, susceptible to infection
119
2.Hypersecretion](https://image.slidesharecdn.com/unit9endocrinesystemanest2017-250402223206-ca0423a1/85/Unit-9-Endocrine-System-Anesthesia-students-2025-AAU-119-320.jpg)
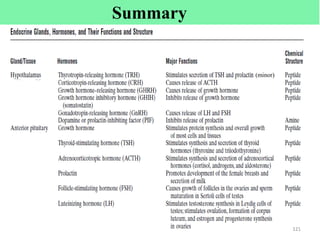
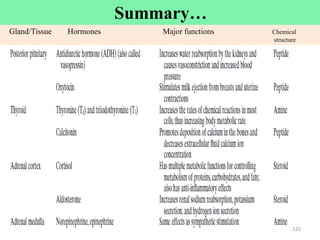
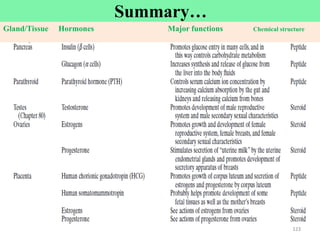
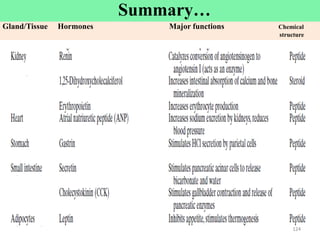





























![Unit=4=Nervous system Physiology=AAU=2017 [Recovered].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/unit4nervoussystemphysiologyaau2017recovered-250402223207-dbf86133-thumbnail.jpg?width=640&height=640&fit=bounds)







![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)














